Everything u need to know about shunts
Reading File
Finding Sources
Searching the Web
medical shunts types CSF vascular portosystemic overview 2024
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
I meant vp shunts
Reading File
Finding Sources
Finding Sources
Searching PubMed
ventriculoperitoneal shunt hydrocephalus complications management
I now have comprehensive information from multiple authoritative textbooks. Here is a full clinical overview of VP shunts:
Ventriculoperitoneal (VP) Shunts - Everything You Need to Know
What Is a VP Shunt?
A VP shunt is a surgically implanted device that diverts excess cerebrospinal fluid (CSF) from the cerebral ventricles to the peritoneal cavity, where it is absorbed by the body. It is the most common long-term treatment for hydrocephalus - the accumulation of CSF that raises intracranial pressure (ICP).
Other shunt variants include:
- Ventriculoatrial (VA) - drains to the right atrium
- Ventriculopleural - drains to the pleural space
- Lumboperitoneal (LP) - drains from the lumbar subarachnoid space to the peritoneum (used in normal-pressure hydrocephalus and idiopathic intracranial hypertension)
Indications
- Obstructive (non-communicating) hydrocephalus - e.g., aqueductal stenosis, posterior fossa tumors
- Communicating hydrocephalus - e.g., post-hemorrhagic, post-meningitic, idiopathic
- Normal pressure hydrocephalus (NPH) - classic triad: gait disturbance, dementia, urinary incontinence
- Idiopathic intracranial hypertension (IIH) - when medical therapy fails and vision is threatened
- Posthemorrhagic ventricular dilatation (premature neonates)
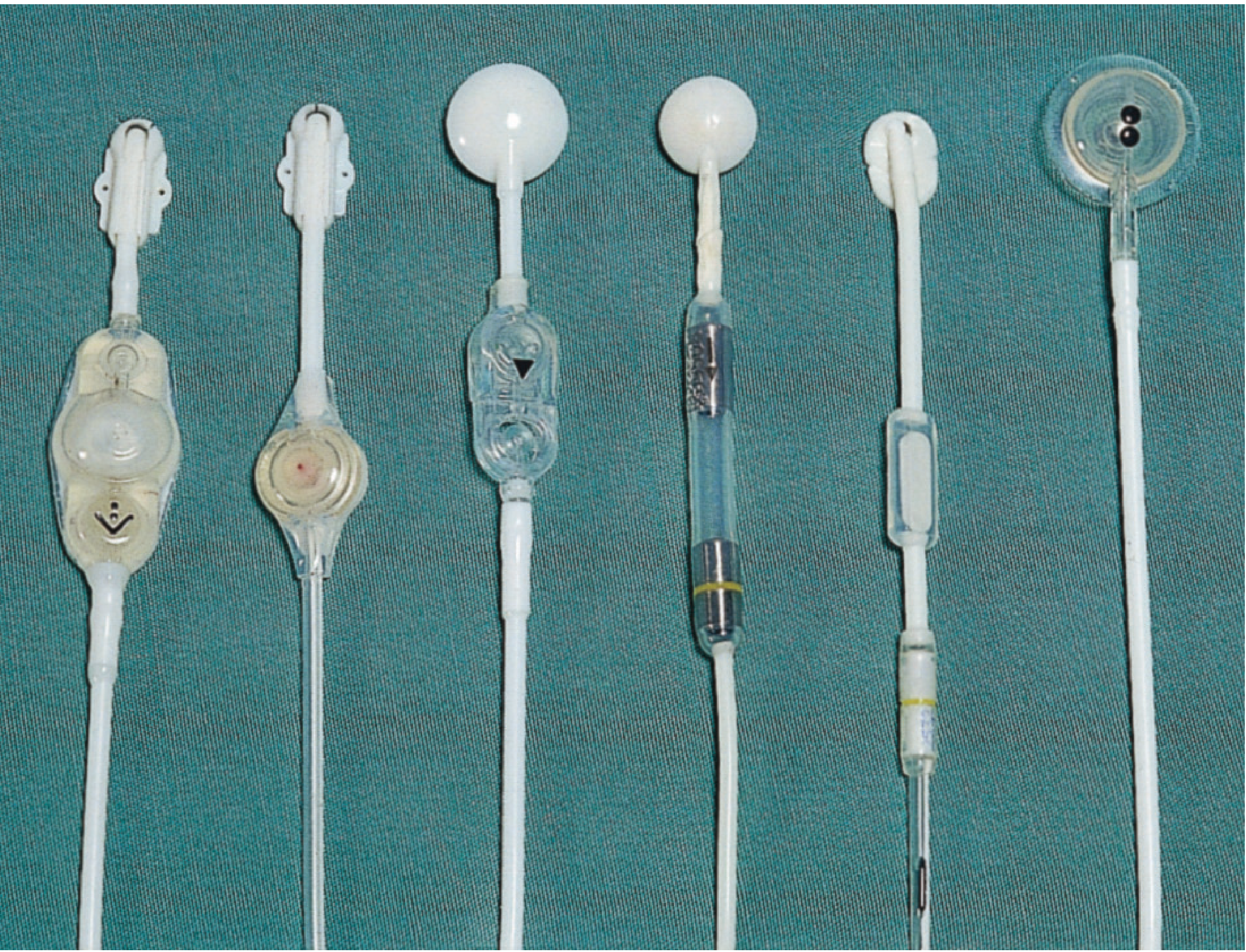
Components of the System
A VP shunt has three main parts (per Bailey & Love's Surgery, p. 726):
| Component | Function |
|---|---|
| Proximal (ventricular) catheter | Inserted into the lateral ventricle |
| Valve | Regulates CSF flow; opens at a preset pressure |
| Distal (peritoneal) catheter | Tunnelled subcutaneously to the abdomen |
Valve types:
- Fixed-pressure valves - open when CSF pressure exceeds a set threshold (low, medium, high resistance)
- Programmable (adjustable) valves - opening pressure changed non-invasively with an external magnetic device; preferred because overdrainage can be corrected without surgery
- Anti-siphon device - prevents excessive drainage when the patient stands upright
- The valve typically incorporates a CSF reservoir dome that can be percutaneously tapped for sampling or pressure measurement
How It Works
CSF is produced at ~500 mL/day by the choroid plexus. When absorption is impaired or flow is blocked, pressure rises. The shunt creates a pressure-dependent bypass: when ICP exceeds the valve's set pressure, the valve opens and CSF flows from ventricle → valve → peritoneal cavity, where it is reabsorbed across the peritoneal membrane.
Surgical Technique (overview)
- A small burr hole is made in the skull (typically right parietal or right frontal)
- The ventricular catheter is passed into the ipsilateral lateral ventricle
- The valve/reservoir is secured to the skull
- The distal catheter is tunnelled subcutaneously (neck → chest → abdomen)
- The distal tip is placed in the peritoneal cavity via a small abdominal incision
After placement, ventricles begin to shrink within ~1 week in high-pressure hydrocephalus. If ventricles remain large despite adequate drainage (as in NPH), this does NOT necessarily indicate malfunction.
Complications
15-20% of VP shunts require replacement within 3 years. - Bailey & Love's, p. 727
1. Obstruction (Most Common)
- Most common cause of shunt failure
- Usually at the ventricular catheter tip or at the valve
- Proximal causes: choroid plexus adhesion, blood clot, proteinaceous debris, infection
- Distal causes: omental wrapping, peritonitis, thrombus, catheter migration, pseudocyst formation
- Presentation: features of raised ICP - headache (worse on waking), vomiting, drowsiness, papilledema; in infants - bulging fontanelle, sunsetting eyes, irritability
- Emergency if obstructive/congenital hydrocephalus - rapid deterioration from uncontrolled ICP rise
2. Infection (Most Serious)
- Occurs in 2-10% of cases
- ~70% present within 2 months of placement (colonization at time of surgery is the main mechanism)
- Common organisms: Staphylococcus epidermidis, S. aureus, gram-negative bacilli
- S. epidermidis adheres to shunt surfaces and produces a biofilm (mucoid substance) that protects it from host defenses; the Silastic material also impairs leukocyte adherence
- Presentation: fever, headache, meningism; may be subtle/indolent
- Diagnosis: CSF tap from shunt reservoir (lumbar puncture if safe); note - culture may be negative even in proven infection
- Treatment: Remove shunt + external ventricular drainage (EVD) + antibiotics; reinsert new shunt once CSF clears
3. Overdrainage
- Rapid decompression of enlarged ventricles can tear bridging veins
- Causes: subdural hygroma or subdural haematoma
- Slit ventricle syndrome (SVS): chronic overdrainage in children leads to underdeveloped ventricles/subarachnoid spaces and poor brain compliance; normal ICP fluctuations become exaggerated; symptoms (headache, nausea) are positional - worse upright, better supine; CT shows slit-like ventricles
- Extra-axial fluid collection: estimated in ~3.4% of cases
- Treatment: raise the valve pressure (programmable valve) or add an anti-siphon device
4. Mechanical (Fracture/Migration)
- Catheter fractures or disconnects (common over years due to patient growth in children)
- Presents similarly to obstruction (subtle raised ICP signs)
- Identified on shunt series X-rays
5. Shunt Nephritis (rare)
- Chronic low-grade bacteremia from an infected VA shunt (less relevant for VP, more for VA shunts) causes immune complex deposition in glomeruli
- Treatment: remove shunt + antibiotics; hemodialysis preferred if dialysis needed (peritonitis risk with peritoneal dialysis)
Clinical Assessment of Shunt Function
History & Exam
- Headache pattern (worse on waking/bending/Valsalva)
- Vomiting, visual changes, cognitive decline
- Palpate the shunt along its subcutaneous tract - look for wound breakdown, CSF leak, disconnection
Manual Pumping Test
Locate the valve chamber by palpation, then gently compress:
| Finding | Interpretation |
|---|---|
| Difficult to compress | Distal obstruction (valve or below) |
| Compresses easily but refills slowly (>3 sec) | Proximal obstruction |
| Normal compression and refill (15-30 sec) | Likely patent |
Caveat: Up to 40% of obstructed shunts show normal refill; positive predictive value of pumping is as low as 12%. Do NOT rely on this alone. - Roberts & Hedges' Emergency Medicine
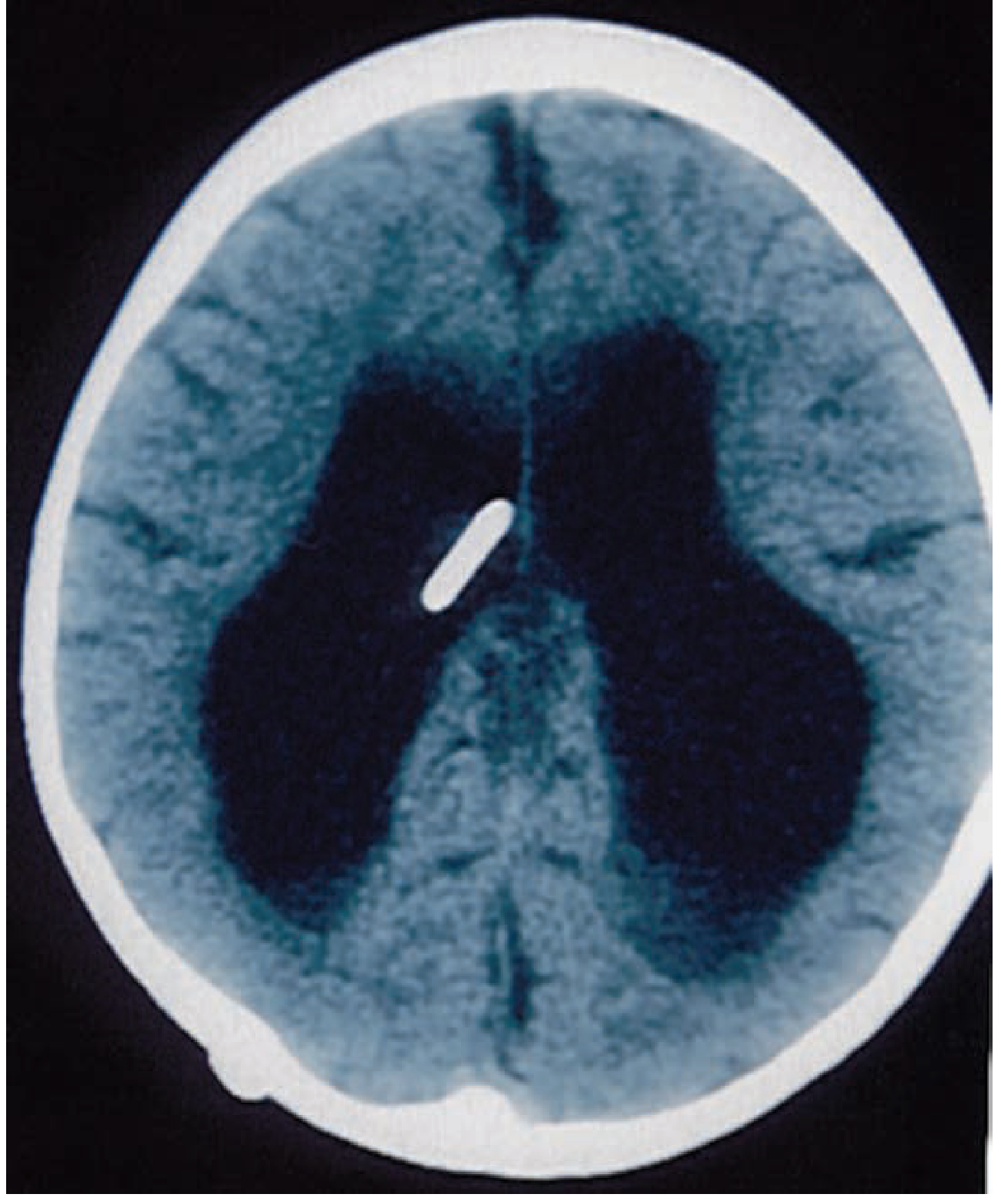
Imaging
- Non-contrast CT head - first-line; look for enlarged ventricles vs. baseline; sensitivity 83%, negative predictive value 93% for obstruction
- Always compare to the patient's previous scans (many have abnormal baseline)
- 9-15% of pediatric patients have poor brain compliance - ventricles won't enlarge even in severe shunt failure
- Shunt series X-rays - AP/lateral skull + AP chest + AP abdomen; detects kinking, fracture, disconnection, migration; sensitivity only 20% but essential when CT is abnormal to localize the failure point
- MRI - useful but can reset programmable valve settings; always consult neurosurgery before MRI in programmable valve patients
- Radionuclide shunt patency study - rarely used but can confirm flow through the system
Shunt Tap
- Performed to: confirm malfunction, rule out infection, or acutely relieve life-threatening ICP
- Should be done by neurosurgery whenever possible
- If neurosurgeon unavailable and the patient is deteriorating, an EM physician should perform it
- Technique: shave + sterile prep over the valve/reservoir; use a 25-gauge butterfly needle; measure opening pressure; send CSF for cell count, glucose, protein, culture
When to Call Neurosurgery
Immediately if:
- Suspected shunt obstruction in obstructive/congenital hydrocephalus (risk of rapid herniation)
- Deteriorating consciousness or focal neurology
- CT showing progressive ventriculomegaly vs. baseline
- Symptoms of infection + known shunt
A normal CT does NOT exclude shunt malfunction if symptoms are convincing.
Special Considerations
| Situation | Issue |
|---|---|
| MRI | May reset programmable valve pressure; get neurosurgery input first |
| Children/adolescents | Need shunt revision as they grow (catheter fracture/migration) |
| Normal pressure hydrocephalus | Ventricles may remain large even when shunt is working |
| Slit ventricle syndrome | CT shows small ventricles yet shunt is malfunctioning - positional symptoms are key |
| Pregnancy | Increased intra-abdominal pressure can impair distal drainage; monitor carefully |
Key Numbers to Remember
| Fact | Value |
|---|---|
| Shunt infection rate | 2-10% |
| Infections presenting within 2 months | ~70% |
| Shunts requiring revision within 3 years | 15-20% |
| CT sensitivity for obstruction | 83% |
| Shunt series sensitivity for obstruction | 20% |
| Overdrainage extra-axial collections | ~3.4% |
Sources: Bailey & Love's Short Practice of Surgery (28th ed.), Roberts & Hedges' Clinical Procedures in Emergency Medicine, Tintinalli's Emergency Medicine, Bradley & Daroff's Neurology in Clinical Practice, Comprehensive Clinical Nephrology (7th ed.)
This is a shared conversation. Sign in to Orris to start your own chat.