Prostate size increase with cystitis and renal concretions
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Searching Images
benign prostatic hyperplasia bladder outlet obstruction complications
Reading File
Excellent — I now have all the content I need for a comprehensive answer. Let me compile everything.
Benign Prostatic Hyperplasia: Prostate Enlargement, Cystitis, and Renal Concretions
Overview
Benign prostatic hyperplasia (BPH) is the most common benign prostatic disease in men over 50 years of age. Its frequency rises progressively with age, reaching 90% by the eighth decade. The three phenomena you've described — prostate size increase, cystitis (bladder infection/inflammation), and renal/bladder concretions (calculi) — are mechanistically linked through a single pathway: bladder outlet obstruction (BOO).
1. Prostate Size Increase (BPH)
Pathogenesis — BPH results from stromal and glandular proliferation in the transition zone (periurethral zone) of the prostate. The key mediator is dihydrotestosterone (DHT), which is 10× more potent than testosterone. It is synthesized locally from circulating testosterone by 5α-reductase type 2 and binds nuclear androgen receptors to promote growth and survival of epithelial and stromal cells. BPH does not occur in men castrated before puberty. With aging, declining testosterone combined with relatively unchanged estrogen levels (via peripheral aromatization) may further drive growth synergistically with DHT. — Robbins & Kumar Basic Pathology
Morphology — The enlarged prostate in BPH typically weighs 60–100 g (3–5× normal). The transition zone compresses the urethra to a slit-like orifice. Hyperplastic nodules contain variable proportions of proliferating glands lined by tall columnar cells with a basal cell layer, and fibromuscular stroma; glandular lumina often contain corpora amylacea (laminated proteinaceous secretory material). — Robbins & Kumar Basic Pathology
Normal size: ~20 mL in young men, increasing to 24–38 mL between ages 50–80. BPH is defined by volume >30 mL, though the degree of symptoms is highly variable. — Goldman-Cecil Medicine
2. The Obstructive Cascade: From Enlarged Prostate to Cystitis
The enlarged prostate compresses the prostatic urethra, raising resistance to urinary outflow. This produces:
- Bladder hypertrophy (detrusor muscle works harder against obstruction)
- Trabeculation → diverticula formation
- Incomplete bladder emptying → residual urine
The reservoir of residual urine is the critical link to infection. It provides a stagnant culture medium for bacteria, making cystitis (and ascending pyelonephritis) a direct complication of BPH.
"The increased resistance to urinary outflow leads to bladder hypertrophy and distention, accompanied by incomplete emptying of the bladder and presence of residual urine. The reservoir of residual urine provides a culture medium for bacteria, a common source of infection." — Robbins & Kumar Basic Pathology
In men, complicated UTI with BPH (cystitis) requires investigation including renal ultrasound, as it is a recognized complicating factor. — Swanson's Family Medicine Review
Patients experience:
- Urinary frequency, urgency, nocturia
- Hesitancy, weak stream, overflow dribbling
- Dysuria (painful micturition)
- Increased risk of bacterial cystitis and pyelonephritis
3. Bladder and Renal Concretions (Calculi)
Bladder stones — BPH is a well-established risk factor. In a large autopsy study, the prevalence of bladder stones was 8 times higher in men with histologic BPH (3.4%) vs. controls (0.4%). The mechanism is again stagnant residual urine: urinary stasis promotes precipitation of mineral salts (predominantly calcium phosphate and uric acid in this context), forming vesical calculi (bladder stones). — Campbell-Walsh-Wein Urology
"In clinical practice, the risk for bladder stone development is small, and screening is only indicated if clinical circumstances warrant it (e.g., hematuria, stuttering of urination)." — Campbell-Walsh-Wein Urology
Renal concretions — BPH-related obstruction does not directly increase ureteral or kidney stone risk in autopsy studies. However, recurrent UTIs secondary to BPH can predispose to struvite (infection) stones (magnesium ammonium phosphate) caused by urease-producing organisms (e.g., Proteus, Klebsiella). Separately, repeated episodes of nephrolithiasis can cause urinary tract obstruction and infection, creating a cycle that leads to loss of renal function and nephrocalcinosis. — Harrison's Principles of Internal Medicine 22E; Campbell-Walsh-Wein Urology
4. Full Complication Cascade Summary
BPH (transition zone hyperplasia, DHT-driven)
↓
Bladder outlet obstruction (BOO)
↓
Incomplete bladder emptying → Residual urine
↓
┌────────────────┬──────────────────────────────┐
│ │ │
Cystitis Bladder stones (vesical calculi) → Hematuria
(recurrent UTI) (urinary stasis → mineral precipitation)
│
↓ Ascending infection
Pyelonephritis / Struvite renal calculi
↓
Hydronephrosis → Renal failure (if untreated)
5. Clinical Workup & Management
| Step | Details |
|---|---|
| History & exam | IPSS/AUA-SI symptom score; digital rectal exam |
| Basic labs | Urinalysis + urine culture (rule out infection); serum PSA (if life expectancy >10 yrs) |
| Imaging | Renal/bladder ultrasound (residual urine volume, hydronephrosis, bladder stones) |
| Additional | Cystoscopy, urodynamics, postvoid residual — when indicated |
Medical therapy (first-line):
- α-blockers (tamsulosin, alfuzosin, etc.) — relax prostatic smooth muscle and bladder neck; effect within days
- 5α-reductase inhibitors (finasteride, dutasteride) — reduce prostate size by 20–25%, prevent BPH progression; effect takes 4–6 months
- PDE-5 inhibitors (tadalafil daily) — approved for BPH+LUTS, especially useful with concomitant erectile dysfunction
- Combination α-blocker + 5-ARI (MTOPS and CombAT trials) reduces risk of acute urinary retention and need for surgery
Surgical therapy (failure/intolerance of medical therapy):
- TURP (gold standard)
- HIFU, laser therapy, transurethral electrovaporization, radiofrequency ablation
— Schwartz's Principles of Surgery; Goldman-Cecil Medicine; Robbins & Kumar Basic Pathology
Gross Pathology Image
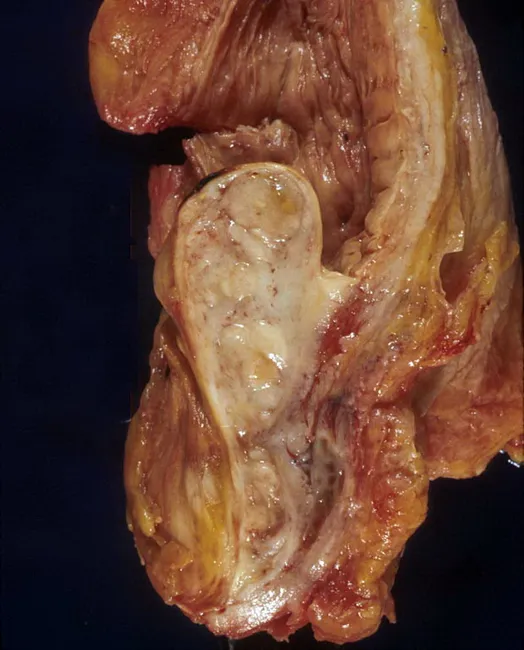
Gross pathology of BPH with median lobe enlargement projecting into the bladder neck, creating ball-valve type obstruction — the anatomic basis for urinary stasis, cystitis, and vesical calculi.
Key Teaching Point: The triad of prostatic enlargement + cystitis + concretions represents a progressive obstruction syndrome. Stagnant residual urine is the common denominator: it serves as both a bacterial culture medium (→ cystitis) and a mineral precipitation environment (→ bladder stones). Renal calculi in this setting are most often struvite (infection stones) secondary to recurrent UTIs, not a direct effect of BPH obstruction per se.
This is a shared conversation. Sign in to Orris to start your own chat.