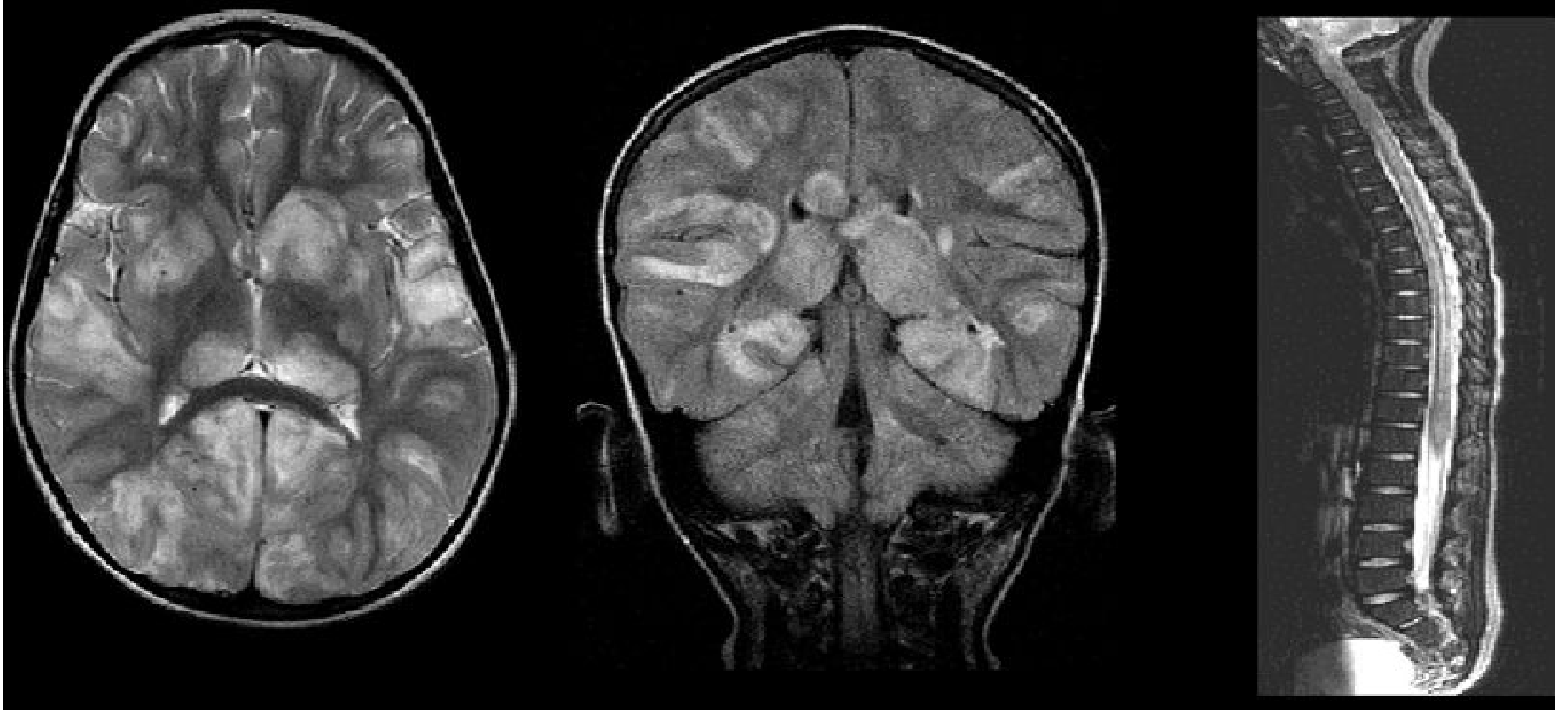
A patient with fever for one day, altered mental status like mild disorientation and slowness of speech, and weakness of the lower limbs, reduced power in lower limbs, and the MRI brain shows multiple foci of demyelination. What could be the possible differential diagnosis?
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Searching PubMed
acute disseminated encephalomyelitis ADEM differential diagnosis
Loading Image
I now have comprehensive information from multiple authoritative sources. Here is the full answer:
Differential Diagnosis: Fever + Altered Mental Status + Lower Limb Weakness + Multiple Demyelinating Foci on MRI Brain
This is a compelling neurological presentation. The combination of acute fever, encephalopathy (disorientation, slowed speech), and lower limb weakness alongside multifocal demyelination on MRI points to a specific differential cluster. The key feature distinguishing this from classic MS is the fever and encephalopathy - the textbooks are explicit that encephalopathy unexplained by systemic illness is characteristic of certain conditions but not typical MS.
1. Acute Disseminated Encephalomyelitis (ADEM) - TOP DIFFERENTIAL
This is the most likely diagnosis given the constellation of findings.
Why it fits:
- Acute onset over 1-2 days with fever
- Encephalopathy (altered consciousness or behavioral change not explained by fever alone) - Adams and Victor's notes this is defining for ADEM vs MS
- Multifocal neurological deficits including motor weakness
- Multiple demyelinating foci on MRI, typically bilateral, asymmetrical, subcortical white matter
Key details from textbooks:
- Occurs 1-3 weeks after a viral infection or vaccination (measles, mumps, rubella; also after Mycoplasma pneumoniae URTI)
- Mediated by T-cell and antibody-driven immune reaction to myelin components (molecular mimicry)
- MRI shows patchy, poorly defined T2/FLAIR hyperintense lesions in subcortical white matter, often with deep grey matter and cerebellar involvement; unlike MS, periventricular "Dawson fingers" are less typical
- CSF may show mild pleocytosis and elevated MBP
- Usually monophasic; most patients recover fully with prompt treatment
2. Viral Encephalitis (e.g., HSV, EBV, CMV, Enterovirus, West Nile, JEV)
Why it fits:
- Acute fever is a cardinal feature
- Altered mental status (confusion, slowed speech)
- Lower limb weakness possible if there is spinal cord or frontoparietal involvement
- MRI can show multifocal white matter changes, especially with herpes (HSV-1 typically temporal, but can be atypical) or flaviviruses
Key distinctions: Viral encephalitis tends to be more cortically based on MRI rather than white matter-predominant; EEG typically abnormal; CSF PCR is diagnostic.
3. Multiple Sclerosis (MS) - First Presentation / Clinically Isolated Syndrome (CIS)
Why to consider:
- Multiple demyelinating foci on MRI brain
- Lower limb weakness (corticospinal tract involvement)
- Slowed speech (possible cerebellar or brainstem lesion)
Why it fits less well here:
- Encephalopathy and fever are uncommon in MS; Bradley & Daroff's explicitly lists encephalopathy as a feature that makes one consider ADEM over MS
- MS lesions tend to be periventricular, ovoid ("Dawson fingers"), at the corpus callosum inferior margin; multifocal subcortical poorly-defined lesions favor ADEM
- No prior relapses mentioned; dissemination in time not established yet
However: If the patient is an adult and has no antecedent infection, MS cannot be excluded without follow-up imaging (McDonald criteria require dissemination in time and space).
4. Neuromyelitis Optica Spectrum Disorder (NMOSD) - AQP4-IgG or MOG-IgG associated
Why to consider:
- Multifocal demyelinating disease
- Lower limb weakness (long tract involvement)
- MRI brain lesions can be extensive (corpus callosum, periependymal, hypothalamus, area postrema)
- MOG-antibody associated disease in particular can present as ADEM-like with encephalopathy, brainstem involvement, and myelitis
Key distinctions: Typically includes optic neuritis or longitudinally extensive transverse myelitis (>3 vertebral segments); check AQP4-IgG and MOG-IgG antibodies. Brain lesions in NMOSD are larger, sometimes tumefactive, following ependymal lines - Goldman-Cecil Medicine lists NMOSD and MOG antibody disorder in the same "monophasic demyelinating syndromes" category as ADEM.
5. CNS Vasculitis / Granulomatous Angiitis of the CNS
Why to consider:
- Can cause multifocal white matter lesions mimicking demyelination
- Systemic or isolated CNS vasculitis (lupus-related, Behcet's, Granulomatosis with polyangiitis) can present with encephalopathy and focal deficits
- Bradley & Daroff's MS differential box includes granulomatous angiitis, SLE, Sjogren's, Behcet's, and polyarteritis nodosa
Key distinctions: Lesions more often ischemic (diffusion restriction); fever more indicative of underlying systemic disease; serology (ANA, ANCA, anti-dsDNA) + angiography helps.
6. Progressive Multifocal Leukoencephalopathy (PML)
Why to consider:
- JC virus-driven multifocal demyelination; MRI shows T2-bright white matter lesions (posterior subcortical)
- Can cause motor and cognitive deficits
Why it fits less in this acute presentation: PML is typically subacute/chronic and occurs in the immunocompromised (HIV, immunosuppressive therapy). Acute fever is not typical unless immune reconstitution inflammatory syndrome (IRIS) is happening. Worth considering if patient is HIV-positive or on biologics.
7. Acute Necrotizing Hemorrhagic Encephalomyelitis (Hurst Disease)
Why to consider:
- Hyperacute, fulminant variant of ADEM
- Bilateral but asymmetric large confluent edematous white matter lesions with petechial hemorrhages
- Fever, encephalopathy, rapid progression to coma
Key distinctions: MRI shows hemorrhagic components (GRE/SWI); CSF shows RBCs and elevated proteins; outcome is poor without aggressive treatment. Must be excluded urgently if presentation is deteriorating rapidly.
8. Autoimmune Encephalitis (e.g., anti-NMDAR, anti-LGI1)
Why to consider:
- Fever, altered mental status, behavioral changes
- MRI may show multifocal T2/FLAIR lesions, though often limbic
- Goldman-Cecil lists autoimmune encephalitis alongside SLE, Sjogren's, sarcoidosis as part of the MS differential
Key distinctions: Anti-NMDAR encephalitis classically in young women with psychiatric prodrome, seizures, movement disorders; MRI lesions are not predominantly demyelinating; antibody panel essential.
9. Neurosarcoidosis
Why to consider:
- Can produce multifocal CNS demyelinating-appearing lesions
- Fever and constitutional symptoms possible
- Listed in the MS differential (Bradley & Daroff's) under granulomatous diseases
Key distinctions: Look for pulmonary involvement on chest X-ray/CT, elevated ACE, uveitis, skin lesions; leptomeningeal enhancement on MRI is a clue.
Approach Summary
| Feature | ADEM | MS | Viral Encephalitis | NMOSD/MOG |
|---|---|---|---|---|
| Fever | Yes | No/rare | Yes | No/rare |
| Encephalopathy | Defining | Uncommon | Yes | Uncommon |
| Lower limb weakness | Yes | Yes | Variable | Yes (myelitis) |
| MRI multifocal demyelination | Yes (subcortical, patchy) | Yes (periventricular, Dawson fingers) | Cortical > white matter | Yes (large, ependymal) |
| Course | Monophasic | Relapsing | Acute | Relapsing |
| Antecedent infection | Often | No | Current | No |
Priority workup:
- CSF - cell count, protein, glucose, oligoclonal bands, viral PCR (HSV, EBV, CMV, enterovirus)
- Serology - AQP4-IgG, MOG-IgG, anti-NMDAR antibodies, ANA, ANCA
- MRI spinal cord with gadolinium - longitudinally extensive lesion favors NMOSD; patchy favors ADEM
- EEG - if seizures or unexplained encephalopathy
- Blood - CBC, CRP, ESR, LDH, viral serology, HIV
Sources:
- Adams and Victor's Principles of Neurology, 12th Ed. (ADEM clinical features, p. 648-656)
- Bradley and Daroff's Neurology in Clinical Practice (Box 80.2: Differential Diagnosis in MS, p. 1385-1452)
- Goldman-Cecil Medicine (Monofocal or Monophasic Demyelinating Syndromes, p. 3986)
- Grainger & Allison's Diagnostic Radiology (ADEM MRI features, p. 2024-2026)
- Robbins, Cotran & Kumar Pathologic Basis of Disease (Demyelinating Diseases overview, p. 1156-1158)
A recent 2025 review on uncommon non-MS demyelinating disorders (PMID 40591029) and advances in atypical demyelinating diseases (PMID 39893021) further support that MOG-antibody disease and NMOSD are important differentials in this type of presentation, and antibody testing is now standard in any acute demyelinating syndrome with encephalopathy.
This is a shared conversation. Sign in to Orris to start your own chat.