Mechanism of contraction of cardiac muscle and relaxation of cardiac muscles from Guyton.
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Finding Sources
Reading File
Loading Image
I now have all the content needed from Guyton. Let me compile the full detailed answer.
Mechanism of Contraction and Relaxation of Cardiac Muscle
(Guyton and Hall Textbook of Medical Physiology)
1. Cardiac Muscle Physiology - Overview
The heart is composed of three major types of cardiac muscle: atrial muscle, ventricular muscle, and specialized excitatory/conductive fibers. Atrial and ventricular muscle contract similarly to skeletal muscle, but the duration of contraction is much longer. Cardiac muscle is striated, and contains actin and myosin filaments that slide during contraction in the same manner as skeletal muscle. However, the mechanism of excitation-contraction coupling is distinctly different.
2. Action Potential in Cardiac Muscle
Figure 9.4 - Rhythmical action potentials from Purkinje fiber and ventricular muscle:
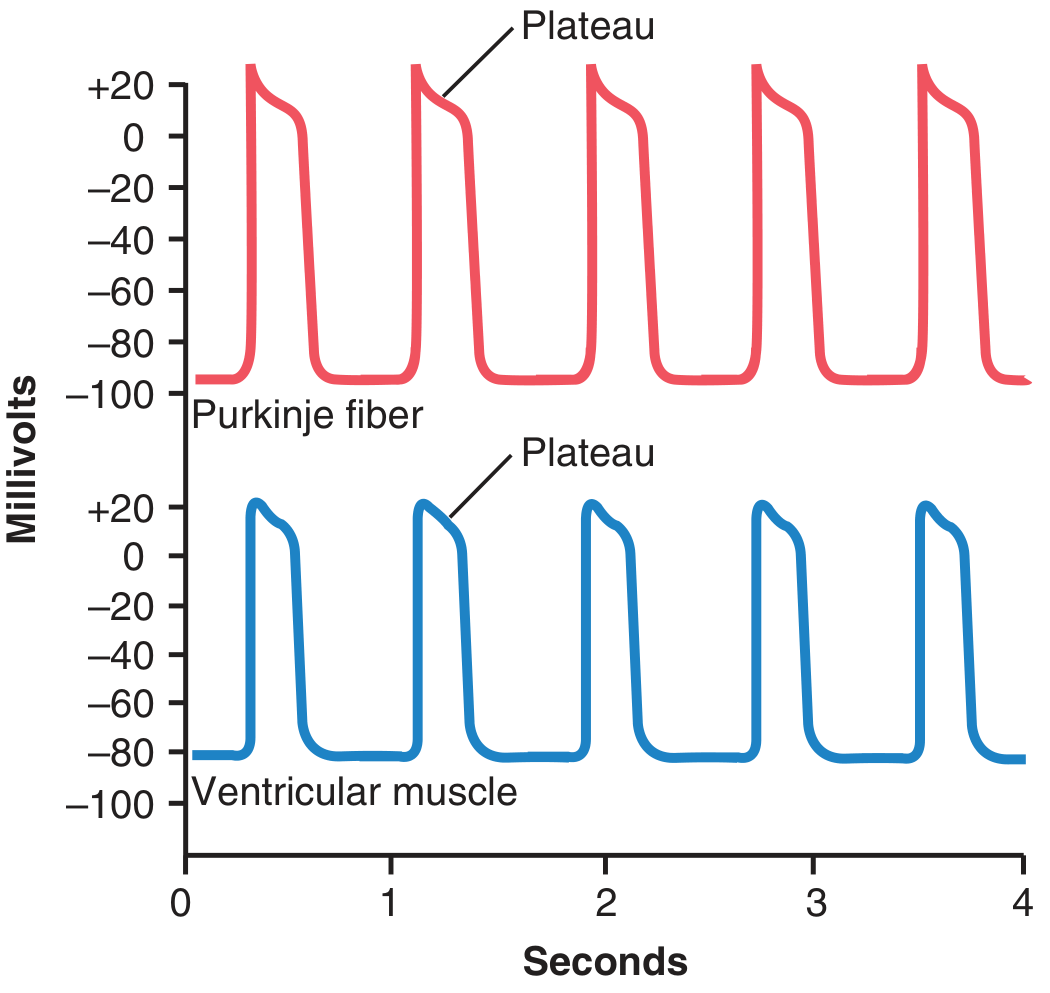
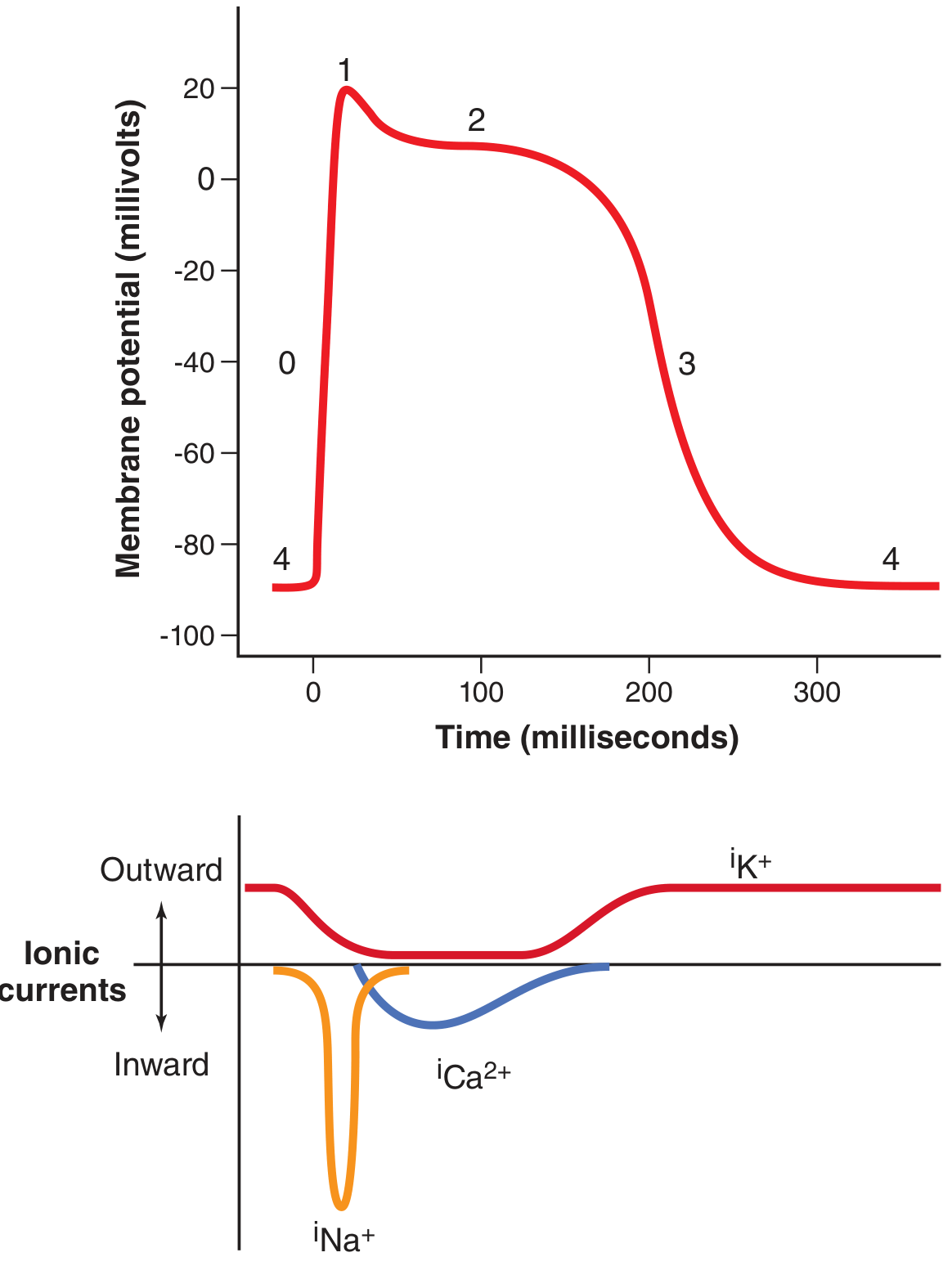
Figure 9.5 - Phases of the ventricular action potential and ionic currents:
The ventricular action potential averages ~105 mV, rising from a resting potential of about -85 mV to +20 mV. It has a characteristic plateau phase (Phase 2) lasting ~0.2-0.3 seconds, which is the critical feature linking the action potential to prolonged contraction.
Phases of the Action Potential:
- Phase 0 - Rapid depolarization: Opening of fast Na+ channels (same as skeletal muscle)
- Phase 1 - Early partial repolarization
- Phase 2 (Plateau) - Maintained depolarization due to two factors:
- Opening of L-type calcium channels (slow calcium channels), which allow sustained influx of Ca²+ and Na+ for several tenths of a second
- A ~5-fold decrease in K+ permeability, which prevents early repolarization by reducing K+ efflux
- Phase 3 - Rapid repolarization: Slow calcium channels close; K+ efflux increases
- Phase 4 - Resting membrane potential (~-85 mV)
3. Excitation-Contraction Coupling - Mechanism of Contraction
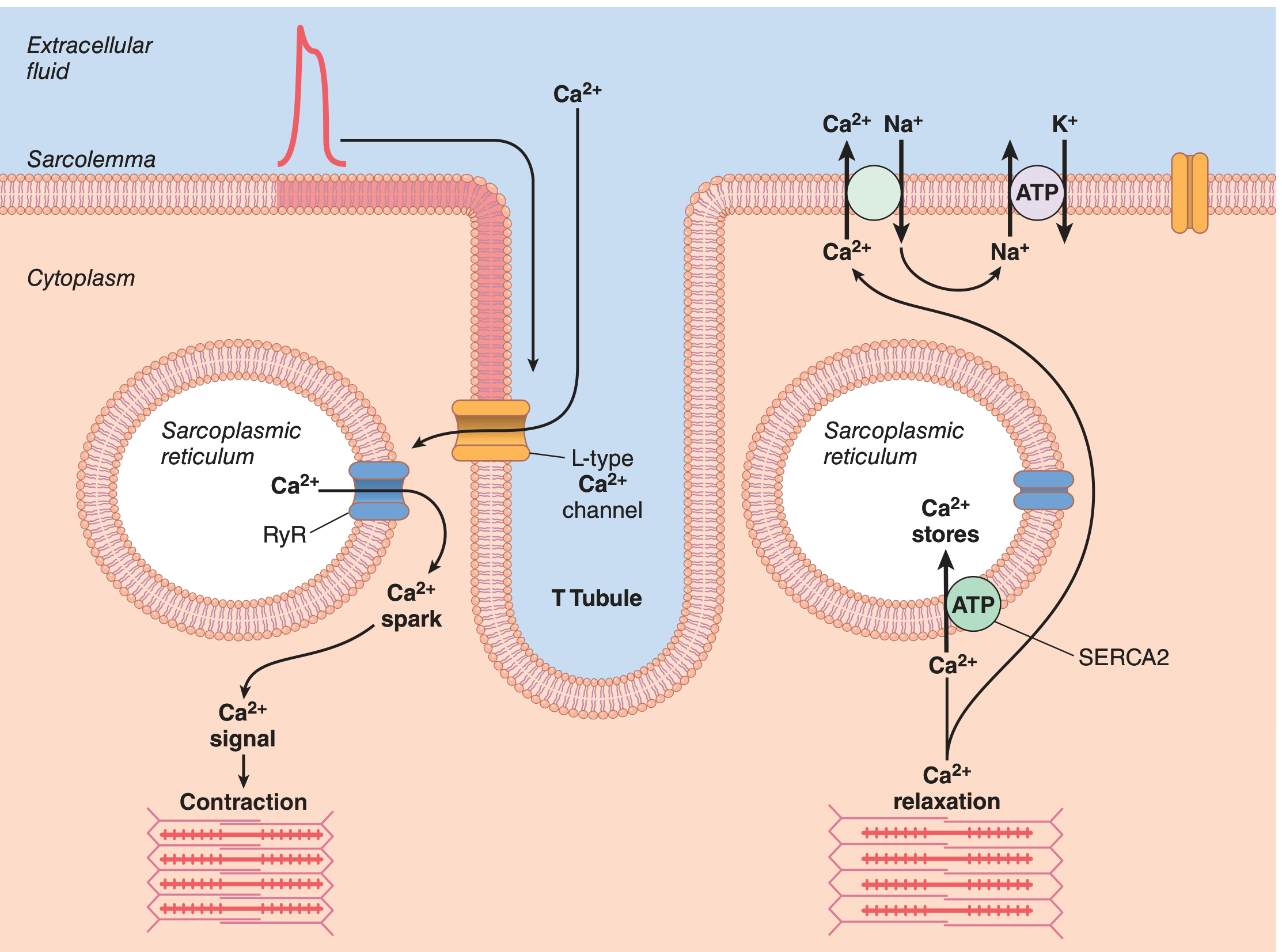
Figure 9.7 - The complete mechanism of excitation-contraction coupling and relaxation:
Step-by-Step Mechanism:
Step 1: Action potential spreads into T tubules
When an action potential passes over the cardiac muscle membrane, it spreads into the interior of the cell along the membranes of the transverse (T) tubules. The T tubules in cardiac muscle are 5 times wider in diameter (and 25 times greater in volume) than those in skeletal muscle. Inside the T tubules, electronegatively charged mucopolysaccharides bind abundant stores of Ca²+, keeping them available for rapid diffusion inward.
Step 2: Calcium-induced calcium release (CICR)
The T tubule action potential does two things simultaneously:
- Opens voltage-gated L-type Ca²+ channels in the T tubule membrane → Ca²+ flows from the T tubule (and extracellular fluid) into the sarcoplasm
- This entering Ca²+ activates ryanodine receptor (RyR) channels on the sarcoplasmic reticulum → triggers a much larger release of Ca²+ from SR stores (the "Ca²+ spark")
This is the critical difference from skeletal muscle: in skeletal muscle, contraction is caused almost entirely by Ca²+ from the SR. In cardiac muscle, Ca²+ from the T tubule/extracellular space is an essential trigger (CICR). Without it, the SR alone cannot provide enough Ca²+ for full contraction.
Step 3: Ca²+ interacts with troponin - cross-bridge cycling
The sarcoplasmic Ca²+ diffuses into the myofibrils and binds to troponin C on the actin filaments. This removes the inhibitory effect of the troponin-tropomyosin complex, exposing the active sites on actin. Myosin heads then form cross-bridges with actin, undergo power strokes using ATP hydrolysis, and the filaments slide past each other - generating force and shortening the muscle. This is the same cross-bridge cycling mechanism as in skeletal muscle.
Dependence on extracellular Ca²+: Because the T tubules open directly into the extracellular space, cardiac muscle contraction depends greatly on extracellular Ca²+ concentration. A heart placed in a calcium-free solution stops beating quickly. This is entirely unlike skeletal muscle, which is largely unaffected by moderate changes in extracellular Ca²+.
4. Mechanism of Relaxation
Relaxation occurs when Ca²+ is removed from the sarcoplasm at the end of the plateau phase. Three mechanisms accomplish this:
| Mechanism | Detail |
|---|---|
| SERCA2 pump (primary) | Ca²+-ATPase pump on the SR membrane actively pumps Ca²+ back into the SR stores, requiring ATP |
| Na+/Ca²+ exchanger (NCX) | Extrudes Ca²+ from the cell across the sarcolemma in exchange for Na+ entry (3 Na+ in: 1 Ca²+ out) |
| Na+/K+-ATPase | Pumps out the Na²+ that entered via NCX, maintaining the Na+ gradient that drives NCX |
When Ca²+ falls in the sarcoplasm:
- Ca²+ dissociates from troponin C
- Troponin-tropomyosin complex returns to its inhibitory position
- Active sites on actin are blocked
- Cross-bridges detach and contraction ceases
The left ventricle also demonstrates elastic recoil/untwisting during diastole. The subepicardial and subendocardial muscle fiber layers, arranged in a double helix, store elastic energy during systole's twisting (wringing) motion. At the end of systole the ventricle resembles a loaded spring and recoils (untwists) during diastole, which actively aids rapid ventricular filling.
5. Duration of Contraction
Cardiac muscle begins to contract a few milliseconds after the action potential begins and continues contracting until a few milliseconds after the action potential ends. Therefore:
- Atrial muscle: contraction lasts ~0.2 seconds
- Ventricular muscle: contraction lasts ~0.3 seconds
This is ~15 times longer than a skeletal muscle twitch, and is directly due to the prolonged plateau of the action potential.
6. Refractory Period
The long plateau also creates a long refractory period (0.25-0.30 sec for ventricles; 0.15 sec for atria). This essentially equals the duration of contraction, which prevents tetanic summation in the heart - a critical physiological safety feature that allows the heart to relax between beats for filling.
- Guyton and Hall Textbook of Medical Physiology, Chapter 9 (Cardiac Muscle; The Heart as a Pump), pp. 123-126
This is a shared conversation. Sign in to Orris to start your own chat.