Peget disease
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Searching PubMed
Paget disease bone treatment bisphosphonate
Reading File
Loading Image
Loading Image
I now have comprehensive information to write a detailed, well-structured answer on Paget's Disease of Bone.
Paget's Disease of Bone (Osteitis Deformans)
Overview
Paget's disease of bone (PDB) is a chronic focal skeletal disorder in which there is an accelerated and disorganized cycle of bone resorption (by large, hyperactive osteoclasts) followed by excessive but structurally weak new bone formation. First described by Sir James Paget in 1876 as "On a Form of Chronic Inflammation of Bones (Osteitis Deformans)", it remains the second most common metabolic bone disease after osteoporosis.
Epidemiology
- Affects 2-3% of persons aged ≥55 years; prevalence rises sharply with age (up to 3-3.7% in those over 40 at autopsy)
- Predominantly a disease of Northern European descent - most prevalent in Great Britain, France, Spain, Italy, Australia, and New Zealand; rare in Asia and India
- Men slightly more affected than women (ratio ~1.4-1.7:1)
- 10-40% of patients report a positive family history
- A notable decline in both prevalence and clinical severity has been observed in recent decades, particularly in formerly high-prevalence areas
Pathogenesis
Genetic Factors
In about one-third of cases, PDB follows an autosomal dominant inheritance pattern with variable penetrance. The most important gene is:
- SQSTM1 (sequestosome 1) on chromosome 5q35, encoding the scaffold protein p62
- Over 20 mutations described, mostly in the ubiquitin-associated (UBA) domain
- The most common mutation, p.P392L, activates NF-κB signaling - the master regulator of osteoclast differentiation and bone resorption
- This mutation is a gain-of-function mutation, amplifying NF-κB activity and thus osteoclast hyperactivity
Environmental Factors
- Paramyxovirus infection (measles, respiratory syncytial virus, canine distemper) - viral nuclear inclusions have been found in pagetic osteoclasts
- Rural lifestyle exposure, possible toxin exposure
- These environmental triggers likely "unmask" genetic susceptibility
Histopathology
The classic histologic picture shows three phases:
- Osteolytic phase - giant multinucleated osteoclasts (with up to 100 nuclei, vs. normal 3-5) aggressively resorb bone
- Mixed phase - coupled, chaotic bone formation produces the hallmark "mosaic" or "jigsaw puzzle" pattern of lamellar cement lines on histology
- Sclerotic phase - bone formation predominates; bone becomes dense but structurally inferior (like "woven" rather than organized lamellar bone)
Clinical Features
Most patients are asymptomatic - the diagnosis is often incidental (elevated ALP on routine bloods, or abnormal X-ray done for another reason).
Skeletal Sites
- Most commonly affected: skull, lumbosacral spine, pelvis, and proximal femur
- Can be monostotic (single bone) or polyostotic (multiple bones)
- Disease is focal - once established in a bone it spreads locally but does not disseminate systemically
Symptoms by Site
| Site | Features |
|---|---|
| Skull | Headache, hearing loss (sensorineural + conductive), visual disturbance, "tam-o-shanter" deformity, basilar invagination → cord compression, hydrocephalus |
| Facial bones | Leontiasis ossea - characteristic lion-like facial deformity from maxillary/mandibular overgrowth |
| Spine | Back pain, spinal stenosis, nerve root compression, cord compression |
| Pelvis/Hip | Secondary osteoarthritis, protrusio acetabuli, varus femoral neck deformity |
| Long bones | Anterolateral bowing (femur, tibia - "sabre tibia"), increased warmth over bone (due to hypervascularity) |
"Leontiasis Ossea" - facial deformity from maxillary Paget disease:
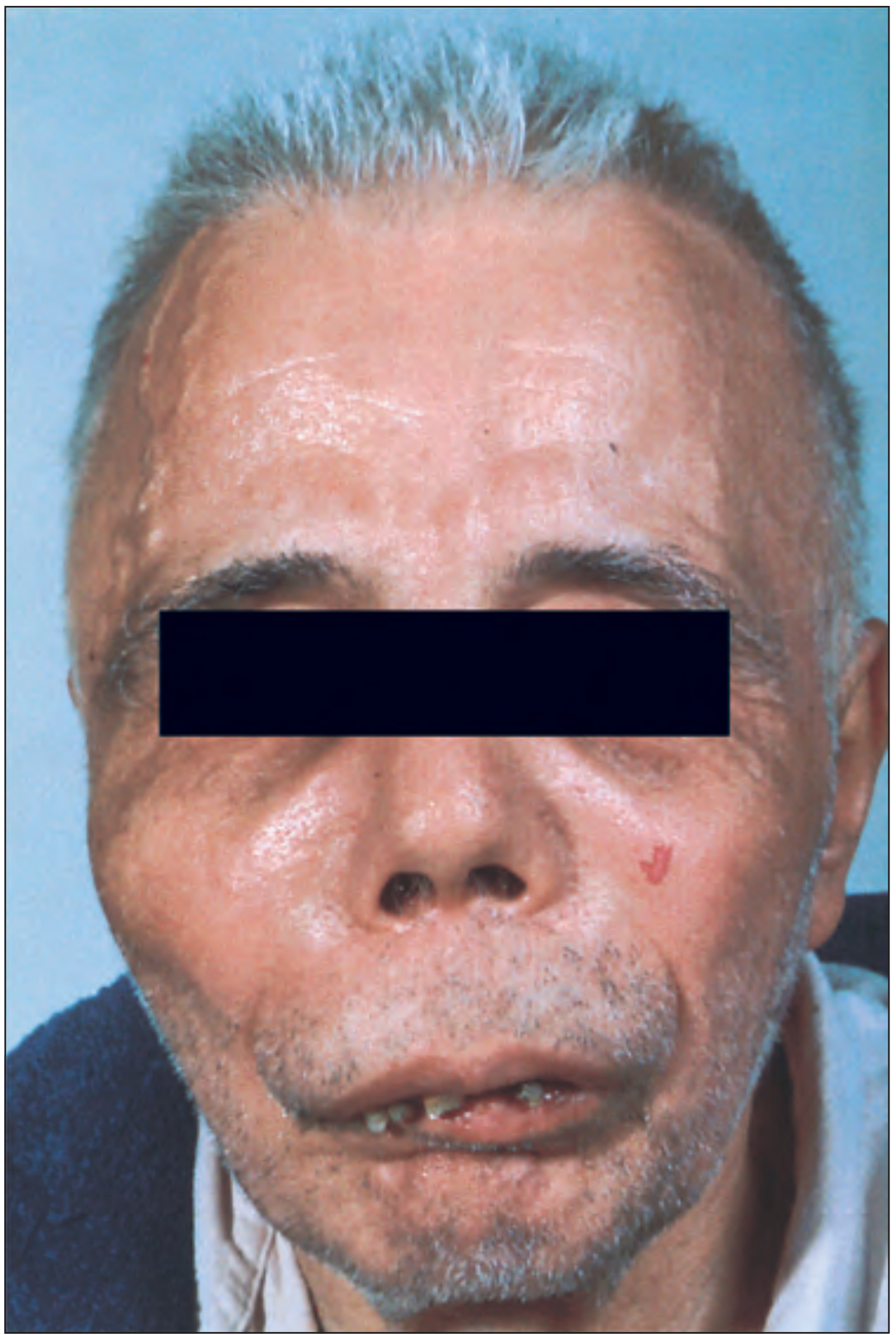
Note the hypertrophy of the right temporal artery - can be mistaken for temporal arteritis.
Paget disease of pelvis and proximal femurs (X-ray):

Note the trabecular disorganization, bone expansion, varus deformity, and secondary femoroacetabular joint space narrowing.
Complications
- Pathological fractures - "chalk-stick" fractures in weight-bearing bones
- Secondary osteoarthritis - in joints adjacent to pagetic bone
- Deafness - temporal bone involvement compresses cranial nerve VIII
- Heart failure (high-output) - due to increased vascularity of extensive pagetic bone (arteriovenous shunting)
- Osteosarcoma - rare but feared complication (~1% of long-standing cases); presents as sudden increase in pain, swelling, and markedly elevated ALP; carries a very poor prognosis
- Hypercalcemia - especially during immobilization
Diagnosis
Biochemical Markers
- Total serum alkaline phosphatase (ALP) - the most widely used marker of disease activity; reflects the rate of bone formation
- Bone-specific ALP - more specific, particularly useful when total ALP is confounded by liver disease
- Urinary markers of bone resorption (e.g., N-telopeptide, C-telopeptide) - indicate osteoclast activity
- ALP can be normal in monostotic or inactive disease
Imaging
- Bone scintigraphy (bone scan) - recommended first for assessing extent of disease; very sensitive, shows all active lesions
- Conventional radiographs - required to confirm diagnosis of lesions found on bone scan; characteristic features:
- Osteoporosis circumscripta - sharply defined osteolytic lesion in skull (early)
- Bone expansion and cortical thickening
- Coarsened, disorganized trabeculae
- "Blade of grass" / "flame-shaped" advancing lytic front in long bones
- "Cotton wool" appearance in skull (later sclerotic phase)
- "Picture frame" vertebra
- CT/MRI - used when spinal stenosis, neural compression, or sarcomatous transformation is suspected
Treatment
Indications for Treatment
Treatment is indicated for:
- Active disease with bone pain attributable to Paget disease
- Preparation for elective surgery on pagetic bone (reduces vascularity and blood loss)
- Disease at sites at risk for complications (skull base, spine, weight-bearing bones)
- Active disease adjacent to major joints (to reduce secondary OA risk)
- Hypercalcemia
Bisphosphonates (First-Line)
| Drug | Route | Notes |
|---|---|---|
| Zoledronic acid | IV (5 mg single infusion) | First choice - most potent, longest remission (often years) |
| Risedronate | Oral (30 mg/day × 2 months) | Alternative; good tolerability |
| Alendronate | Oral | Effective alternative |
| Pamidronate | IV infusion | Older agent, still used |
Bisphosphonates work by inhibiting osteoclast-mediated bone resorption (via the mevalonate pathway). Response is monitored by normalization of ALP.
Calcitonin
- Salmon calcitonin (intranasal or SC injection) is an older agent; less effective than bisphosphonates but still used in patients who cannot tolerate bisphosphonates or pre-/post-operatively
- It decreases osteoclastic activity and reduces perioperative blood loss
Analgesics
- NSAIDs and simple analgesics for pain not directly from pagetic activity (e.g., secondary OA, nerve compression)
Surgical Management
- Total hip arthroplasty (THA) - for painful secondary osteoarthritis or femoral neck fracture; technically challenging due to bone deformity and hypervascularity
- Reported 7-10 year implant survival ~86%
- Bisphosphonates and calcitonin pre-operatively reduce blood loss
- Heterotopic bone formation is a common post-op complication
- Spinal decompression - for spinal stenosis or cord compression
- Osteotomy - if severe long bone bowing prevents intramedullary stem placement during THA
Monitoring and Follow-up
- Serum ALP every 3-6 months during treatment; then every 6-12 months during remission
- Bone scan at diagnosis (to map all lesions); repeat only if new symptoms arise
- Radiographs of symptomatic or high-risk sites periodically
- Watch for sudden worsening of pain or swelling - this should prompt suspicion for osteosarcomatous transformation
Key Associations to Remember
| Feature | Details |
|---|---|
| Gene | SQSTM1/p62 (NF-κB pathway) |
| Lab marker | ↑↑ Alkaline phosphatase |
| Best imaging for extent | Bone scintigraphy |
| Best drug | Zoledronic acid IV |
| Feared complication | Osteosarcoma (~1%) |
| High-output cardiac failure | Extensive polyostotic disease |
| Skull finding (early) | Osteoporosis circumscripta |
| Facial deformity | Leontiasis ossea |
| Histology | Mosaic/jigsaw cement lines |
Sources: Rheumatology, 2-Volume Set (Elsevier 2022), p. 498-518; Goldman-Cecil Medicine International Edition; Campbell's Operative Orthopaedics 15th Ed (2026)
This is a shared conversation. Sign in to Orris to start your own chat.