Status epilecticus pharmacology
Reading File
Finding Sources
Searching PubMed
"status epilepticus" AND treatment
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have comprehensive information from multiple authoritative sources. Here is a full, synthesized answer:
Status Epilepticus: Pharmacology
Definition and Time-Based Classification
Status epilepticus (SE) is defined as a seizure lasting ≥5 minutes (generalized tonic-clonic) or ≥10 minutes (focal with impaired awareness), OR two or more seizures without recovery of consciousness between them. Treatment begins at the 5-minute mark because:
- Seizures are unlikely to stop spontaneously after this point
- Permanent neuronal injury becomes progressively likely
- Drug efficacy decreases over time due to receptor internalization
Phases by time:
| Phase | Timeframe | Definition |
|---|---|---|
| Early/Impending SE | 0-5 min | Active seizure, high chance of spontaneous termination |
| Established SE | 5-30 min | Requires immediate pharmacologic intervention |
| Refractory SE | >30 min after first + second-line therapy | Persists despite benzodiazepine + one second-line agent |
| Super-refractory SE | >24 h after third-line (anesthetic) therapy | Highest mortality |
Pathophysiology Underpinning Drug Targets
As seizures pass 5 minutes, two major shifts occur that explain why later treatment is harder:
- GABA-A receptor internalization - surface receptor expression falls sharply, reducing benzodiazepine efficacy
- Upregulation of NMDA and glutamate receptors - excitatory tone increases
- Blood-brain barrier compromise allows K⁺ and albumin (both hyperexcitatory) into the CNS
- After 20 minutes: hypotension, hypoxia, metabolic acidosis, hyperthermia, cardiac dysrhythmias, and pulmonary edema develop
This receptor plasticity is why benzodiazepines must be given early and in adequate doses, and why later phases require drugs with different mechanisms.
Treatment Algorithm
The treatment protocol image from Tintinalli's Emergency Medicine summarizes the approach:
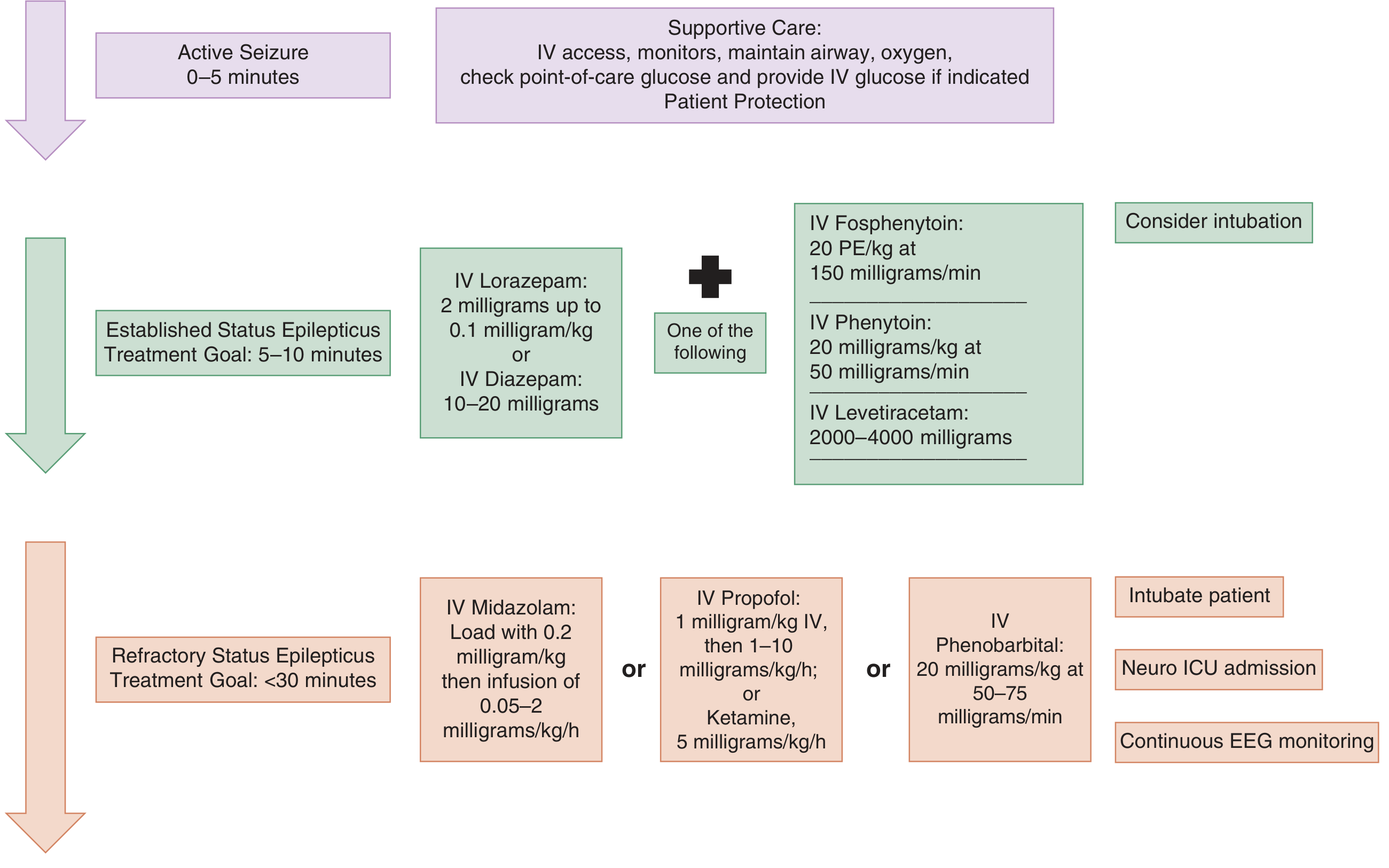
Phase 1 - First-Line: Benzodiazepines (0-10 min)
Benzodiazepines are the initial treatment of choice. They work by enhancing GABA-A receptor-mediated Cl⁻ influx, increasing the frequency of channel opening.
Drug Comparison
| Drug | Route | Dose | Onset | Key Pharmacokinetic Feature |
|---|---|---|---|---|
| Lorazepam IV | IV | 0.1 mg/kg (max 4 mg) at 2 mg/min | ~2 min | Less lipophilic (logP 2.4); minimal redistribution to peripheral fat; longer effective CNS duration |
| Diazepam IV | IV | 0.2 mg/kg (5-10 mg bolus at 5 mg/min) | 1-3 min | Highly lipophilic (logP 2.0); rapidly redistributes to peripheral fat → short CNS duration despite long plasma half-life |
| Midazolam IM | IM | 10 mg (adult); preferred if no IV access | 5-10 min | Water-soluble at low pH; IM absorption reliable; RAMPART trial: non-inferior to IV lorazepam in prehospital SE |
| Midazolam intranasal/buccal | IN/buccal | 0.2 mg/kg | 5-10 min | Useful in children, community setting |
| Diazepam rectal | Rectal | 0.2-0.5 mg/kg | Slower | Community/prehospital alternative |
| Clonazepam IV | IV | 1 mg at 0.5 mg/min | Fast | Used outside USA |
Key pharmacokinetic insight: Lorazepam is preferred over diazepam for IV use because of less extensive peripheral redistribution - effective CNS concentrations persist longer. However, clinical trials have not consistently shown superiority; the perceived pharmacokinetic advantage is the main rationale.
Benzodiazepines terminate early SE in ~70% of cases. A second dose may be given after 5 minutes of continued seizure activity.
Phase 2 - Second-Line Agents (Benzodiazepine-Refractory, 10-30 min)
These are given when benzodiazepines fail. All three approved options have roughly equal efficacy (~50% seizure cessation) in benzodiazepine-refractory SE (supported by the ESETT trial).
1. Fosphenytoin / Phenytoin
- Fosphenytoin: Water-soluble prodrug; rapidly converted to phenytoin in plasma. Can be given IV or IM. Rate: up to 150 mg PE/kg/min. Better tolerated than phenytoin (less cardiotoxic, less sclerosing to vasculature).
- Phenytoin: Dose 20 mg/kg IV at ≤50 mg/min (slower due to cardiac risk). Requires cardiac monitoring - risk of hypotension, bradycardia, and arrhythmia. Must not be given in glucose-containing solutions (precipitates).
- Mechanism: Blocks voltage-gated Na⁺ channels (prolongs inactivated state), reducing high-frequency neuronal firing. No CNS depression.
2. Valproic Acid (Valproate)
- Dose: 30-40 mg/kg IV at 5 mg/kg/min
- Mechanism: Multiple - Na⁺ channel blockade, enhanced GABA synthesis/metabolism, T-type Ca²⁺ channel blockade
- Advantages: Can give faster than phenytoin; no cardiac monitoring required; effective in absence SE
- Contraindications: Liver disease, thrombocytopenia, suspected mitochondrial/metabolic disease, pregnancy (teratogenic - neural tube defects)
3. Levetiracetam
- Dose: 2000-4000 mg IV (or 30-60 mg/kg) over 10 minutes
- Mechanism: Binds SV2A (synaptic vesicle glycoprotein 2A) - reduces neurotransmitter release from presynaptic vesicles. Also modulates GABA and glycine inhibitory transmission.
- Advantages: No hepatic metabolism, few drug interactions, no cardiac toxicity, can be given rapidly
- Increasingly preferred due to favorable safety profile
4. Phenobarbital (IV)
- Dose: 10-20 mg/kg IV at 50-75 mg/min
- Mechanism: Enhances GABA-A activity (prolongs duration of Cl⁻ channel opening), also directly activates Cl⁻ channels at high doses
- Highly effective but limited by severe sedation, respiratory depression, and hypotension
- Often avoided as second-line; still used when other agents fail
5. Lacosamide (IV)
- Mechanism: Enhances slow inactivation of Na⁺ channels (distinct from phenytoin which targets fast inactivation)
- Generally well tolerated but ECG monitoring required (risk of PR interval prolongation and arrhythmia)
- Emerging evidence supports use as second-line
Phase 3 - Refractory SE: IV Anesthetic Agents (>30 min)
When two adequate treatment attempts fail, the patient requires ICU admission, endotracheal intubation, and continuous IV anesthetic infusions with EEG monitoring.
| Drug | Loading Dose | Infusion | Notes |
|---|---|---|---|
| Midazolam | 0.2 mg/kg IV | 0.05-2 mg/kg/h | First choice in many centers; tachyphylaxis can develop |
| Propofol | 1 mg/kg IV | 1-10 mg/kg/h | Rapid onset/offset; risk of propofol infusion syndrome (PRIS) with prolonged high-dose use (metabolic acidosis, rhabdomyolysis, cardiac failure) |
| Pentobarbital | 5-15 mg/kg IV | 0.5-3 mg/kg/h | Potent; achieves burst suppression; risk of hypotension, ileus |
| Thiopental | 3-5 mg/kg IV | 3-5 mg/kg/h | Similar to pentobarbital; not available in all countries |
| Ketamine | 1-5 mg/kg IV | 2.2-5 mg/kg/h | NMDA receptor antagonist; hemodynamically supportive; increasingly used in super-refractory SE - 2024 meta-analysis (PMID 38881333) supports efficacy in pediatric SE; avoids respiratory depression |
Key principle: Paralytic agents should NOT be used for long-term control - they mask ongoing seizure activity visible only on EEG. Continuous EEG monitoring is mandatory in all intubated patients with SE.
Phase 4 - Super-Refractory SE (>24 h on anesthetics)
Options include:
- Inhaled volatile anesthetics (isoflurane, desflurane) - GABA potentiation
- Ketamine (if not already used)
- Immunotherapy (steroids, IVIG, plasmapheresis) - if autoimmune encephalitis suspected (notably now the most common cause in one large study, per Goldman-Cecil Medicine)
- Non-pharmacologic: Vagal nerve stimulation, electroconvulsive therapy (evidence limited), ketogenic diet
- Therapeutic hypothermia - not beneficial based on current evidence
Summary Drug Table
| Phase | Drug | Mechanism | Key Dose | Key Risk |
|---|---|---|---|---|
| 1st line | Lorazepam IV | GABA-A agonist (Cl⁻ channel frequency ↑) | 0.1 mg/kg IV | Respiratory depression, sedation |
| 1st line | Midazolam IM | GABA-A agonist | 10 mg IM | Less if used IM |
| 1st line | Diazepam IV | GABA-A agonist | 0.2 mg/kg IV | Short CNS duration (redistribution) |
| 2nd line | Fosphenytoin | Na⁺ channel blockade | 20 mg PE/kg IV | Less cardiotoxic than phenytoin |
| 2nd line | Levetiracetam | SV2A binding; ↓ vesicular release | 2000-4000 mg IV | Behavioral (irritability) |
| 2nd line | Valproate | Na⁺ block + GABA enhancement + Ca²⁺ block | 30-40 mg/kg IV | Hepatotoxicity; contraindicated in pregnancy/liver disease |
| 2nd line | Phenobarbital | GABA-A (duration of Cl⁻ channel opening ↑) | 10-20 mg/kg IV | Respiratory depression, hypotension |
| 2nd line | Lacosamide | Slow Na⁺ channel inactivation | 200-400 mg IV | PR prolongation, arrhythmia |
| 3rd line | Midazolam infusion | GABA-A agonist | 0.05-2 mg/kg/h | Tachyphylaxis |
| 3rd line | Propofol infusion | GABA-A potentiation + Na⁺/Ca²⁺ block | 1-10 mg/kg/h | Propofol infusion syndrome |
| 3rd line | Pentobarbital | GABA-A (also direct channel activation) | 0.5-3 mg/kg/h | Hypotension, ileus |
| 3rd/4th | Ketamine | NMDA receptor antagonist | 2.2-5 mg/kg/h | Raises ICP (caution in ↑ICP) |
Supportive Measures (All Phases)
- Secure airway, oxygen, large-bore IV; avoid glucose-containing fluids if giving phenytoin
- Cardiac monitoring (especially with phenytoin, fosphenytoin, lacosamide)
- Correct metabolic triggers: hypoglycemia, hyponatremia, hypocalcemia, hypomagnesemia
- Thiamine 100 mg IV before glucose in alcoholic or malnourished patients
- Target seizure control within 30 minutes of presentation
Sources: Katzung's Basic and Clinical Pharmacology 16e; Tintinalli's Emergency Medicine; Rosen's Emergency Medicine; Goldman-Cecil Medicine; Miller's Anesthesia 10e; Bradley and Daroff's Neurology in Clinical Practice. Recent guidelines review: Vignatelli et al., Epilepsia 2024 (PMID 38606469); Refractory SE anesthetics review: Au et al., JAMA Neurol 2024 (PMID 38466294).
This is a shared conversation. Sign in to Orris to start your own chat.