Viral hepatitis
Reading File
Finding Sources
Searching PubMed
"viral hepatitis" AND treatment
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Reading File
I now have comprehensive material from multiple authoritative textbooks. Let me compile the full, detailed answer on viral hepatitis.
Viral Hepatitis
A comprehensive overview based on Robbins & Kumar Basic Pathology, Goldman-Cecil Medicine, and Sleisenger & Fordtran's GI and Liver Disease.
Overview
The term "viral hepatitis" refers to liver inflammation caused by hepatotropic viruses - those with a specific tropism for hepatocytes. Five major agents are recognized: HAV, HBV, HCV, HDV, and HEV. Other viruses (EBV, CMV, HSV, SARS-CoV-2, adenovirus) can also cause hepatitis but are not primarily hepatotropic. Liver injury in all forms is immune-mediated rather than directly cytopathic - CD8+ cytotoxic T cells, pro-inflammatory cytokines, NK cells, and antibody-dependent cellular cytotoxicity all contribute to hepatocellular damage.
- Robbins & Kumar Basic Pathology, p. 598
Comparative Summary Table
| Feature | HAV | HBV | HCV | HDV | HEV |
|---|---|---|---|---|---|
| Genome | ssRNA | Partially dsDNA | ssRNA | Circular defective ssRNA | ssRNA |
| Family | Hepatovirus (Picornaviridae) | Hepadnaviridae | Flaviviridae | Deltaviridae (subviral) | Hepeviridae |
| Transmission | Fecal-oral | Parenteral, sexual, perinatal | Parenteral (IVDU, needlestick) | Parenteral (requires HBV) | Fecal-oral |
| Incubation | 2-6 weeks | 2-26 weeks (mean 8 wk) | 4-26 weeks (mean 9 wk) | Same as HBV | 4-5 weeks |
| Chronic disease | Never | 5-10% (adults); >90% (perinatal) | >80% | 10% (coinfection); 90-100% (superinfection) | Rarely (immunocompromised) |
| Carrier state | No | Yes | Yes | Yes (with HBV) | No |
| Vaccine | Yes (since 1995) | Yes | No | Prevented by HBV vaccine | Approved in China; investigational elsewhere |
Individual Viruses
Hepatitis A (HAV)
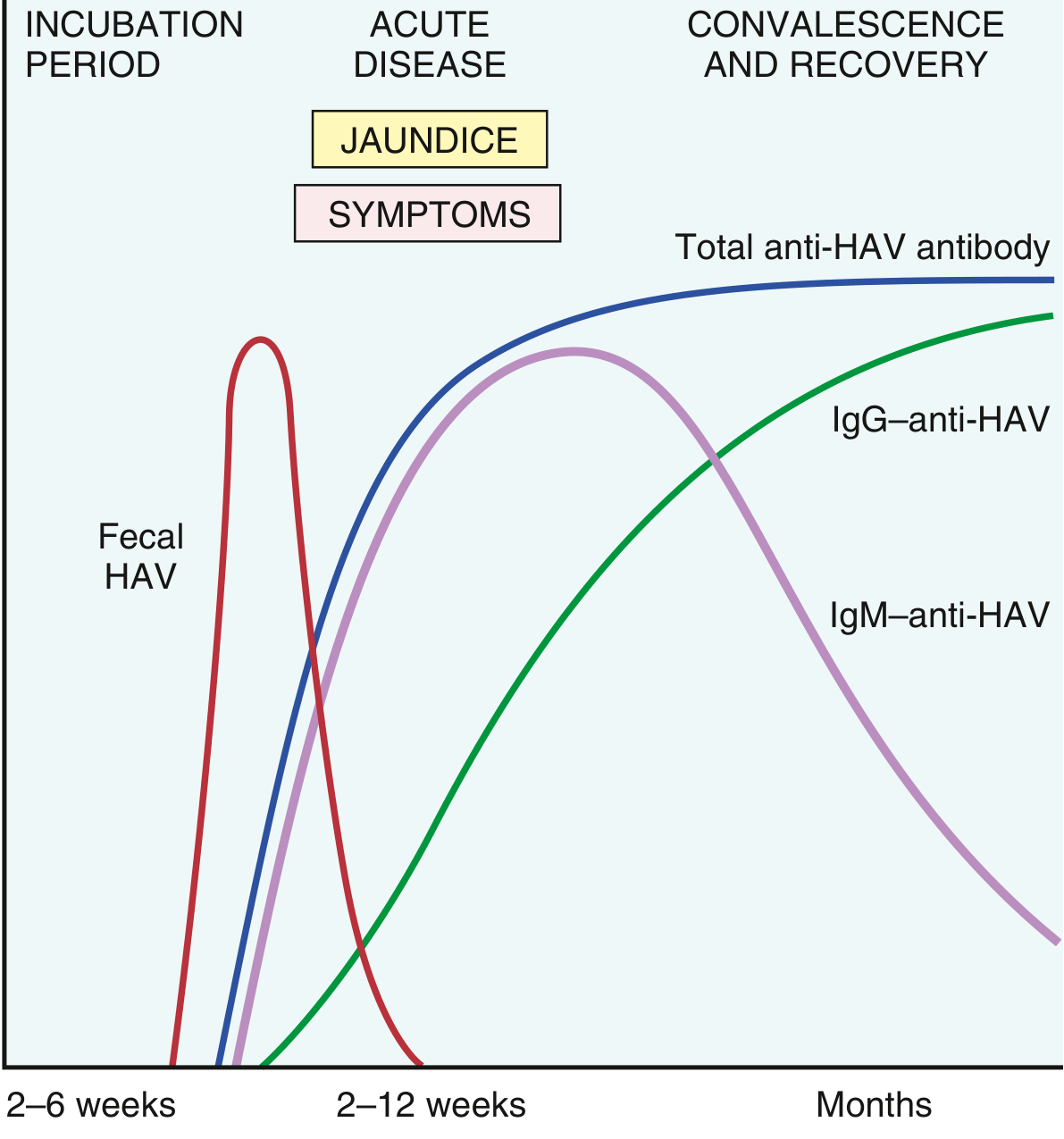
HAV is a non-enveloped, positive-strand RNA picornavirus. Transmission is fecal-oral, typically via contaminated water, food, shellfish, or infected food-industry workers. It sheds in stool for 2-3 weeks before and 1 week after jaundice onset - the period of peak infectivity.
Key features:
- Incubation: 2-6 weeks
- Self-limited; never causes chronic hepatitis
- Fulminant hepatitis in ~0.1% of cases
- Does not establish a carrier state
- HAV itself is not cytopathic; CD8+ T cells drive hepatocellular injury
- Viremia is transient, so bloodborne transmission is very rare
Serologic diagnosis:
-
IgM anti-HAV: appears at symptom onset - marker of acute infection
-
Fecal viral shedding ends as IgM titer rises
-
IgG anti-HAV: persists for years, confers lifelong immunity
-
HAV vaccine (live attenuated) has reduced US cases by >95% since 1995 (~2,800 cases/year now)
-
Robbins & Kumar Basic Pathology, p. 598-599
Hepatitis B (HBV)
HBV is the world's most consequential hepatitis virus. Two billion people have been infected; 250 million have chronic infection; 75% of carriers live in Asia and the Western Pacific rim.
Structure: Enveloped, partially double-stranded DNA virus (hepadnavirus). The virion (Dane particle) has:
- HBsAg (surface antigen) - on the outer envelope
- HBcAg (core antigen) - on the nucleocapsid (not found in serum)
- HBeAg - a secreted antigen derived from pre-core protein; correlates with active viral replication and infectivity
HBV replication involves reverse transcriptase (unique among DNA viruses), so antiviral drugs targeting RT (tenofovir, entecavir) are effective.
Clinical outcomes of HBV:
- Acute hepatitis with recovery and viral clearance
- Nonprogressive chronic hepatitis
- Progressive chronic disease → cirrhosis → hepatocellular carcinoma (HCC)
- Fulminant hepatitis with massive liver necrosis
- Asymptomatic "healthy" carrier state
Chronicity rates:
- Adult-acquired infection: 5-10% progress to chronic
- Perinatally acquired (endemic areas): >90% develop chronic infection and carrier state
Extrahepatic manifestations (immune complex-mediated):
- Membranous or membranoproliferative glomerulonephritis
- Polyarteritis nodosa (hepatitis B surface antigen-containing immune complexes)
- Serum sickness-like prodrome (urticaria, arthralgias, fever)
Serology and markers:
| Marker | Significance |
|---|---|
| HBsAg | Present in acute and chronic infection; persistence >6 months = chronic |
| Anti-HBs | Appears after recovery or vaccination; confers immunity |
| IgM anti-HBc | Acute infection (including window period when HBsAg has cleared but anti-HBs has not yet appeared) |
| IgG anti-HBc | Past or chronic infection |
| HBeAg | Active viral replication; high infectivity |
| Anti-HBe | Decreasing replication; seroconversion is favorable |
| HBV DNA (PCR) | Quantifies viral load; guides therapy |
Treatment:
- Tenofovir disoproxil fumarate (TDF) or tenofovir alafenamide (TAF) - first-line nucleotide analogues
- Entecavir - first-line nucleoside analogue
- Pegylated interferon-alpha - finite-duration therapy; suitable for selected patients
- Goal: sustained suppression of HBV DNA, HBeAg seroconversion, and ideally HBsAg loss
Hepatitis C (HCV)
HCV is the leading cause of chronic liver disease and liver transplantation in the Western world.
Structure: Enveloped, single-stranded RNA flavivirus. Its genome encodes a single polyprotein processed into 10 functional proteins including:
- NS3/4A protease - required for polyprotein processing (target of drugs like glecaprevir, voxilaprevir)
- NS5A - essential for viral assembly (target of ledipasvir, velpatasvir)
- NS5B RNA polymerase - replicates the viral genome (target of sofosbuvir)
Because the RNA polymerase has very low fidelity, HCV mutates rapidly, generating 7 major genotypes and multiple quasispecies within each infected patient. This rapid mutation previously complicated treatment, though modern pan-genotypic regimens overcome this.
Risk factors for HCV:
- Intravenous drug use (IVDU) - most common route in high-income countries
- Needlestick injury (risk ~1.8% per stick vs. 0.3% for HIV)
- Perinatal transmission (~5-6% of infants born to HCV+ mothers)
- Blood transfusion (risk now essentially zero in developed countries due to screening)
- Sexual transmission is inefficient but possible
Clinical course:
- Incubation: 4-26 weeks (mean 9 weeks)
- 85% of acute infections are asymptomatic - most patients unaware they are infected
- HCV RNA detectable in blood within 1-3 weeks of exposure
- Severe acute hepatitis is rare
- >80% develop chronic infection - major distinguishing feature from HBV
- Of those with chronic HCV: ~20% develop cirrhosis over 20-30 years
- Cirrhosis is a major risk for HCC; HCV accounts for ~1/3 of liver cancers in the US
Characteristic feature of chronic HCV: episodic elevations of serum aminotransferases separated by periods of normal levels - patients may appear to improve but fibrosis still progresses.
Treatment (Direct-Acting Antivirals - DAAs):
- Sofosbuvir/ledipasvir (Harvoni) - for genotype 1
- Sofosbuvir/velpatasvir (Epclusa) - pan-genotypic
- Glecaprevir/pibrentasvir (Mavyret) - pan-genotypic, 8 weeks for non-cirrhotic
- Sustained virologic response (SVR) - undetectable HCV RNA 12 weeks after treatment completion - is equivalent to cure; achieved in >95% of patients
Hepatitis D (HDV)
HDV is a defective viroid - it can only infect individuals already infected with HBV because it uses HBsAg as its own envelope protein. HDV contains circular, defective single-stranded RNA and is classified in Deltaviridae.
Two patterns of HDV infection:
- Coinfection (simultaneous HDV + HBV acquisition): usually self-limited, low risk of chronicity (~10%), but higher risk of fulminant hepatitis than HBV alone
- Superinfection (HDV acquired by chronic HBV carrier): severe, rapidly progressive; 90-100% develop chronic HDV hepatitis; may cause acute-on-chronic liver failure
Prevention: HBV vaccination also prevents HDV.
Treatment: Pegylated interferon alpha (modest efficacy). Bulevirtide (a novel entry inhibitor) has received conditional approval in Europe for chronic HDV.
Hepatitis E (HEV)
HEV is a non-enveloped, single-stranded RNA virus in the Hepeviridae family. Like HAV, it is transmitted fecal-orally.
Key features:
- Incubation: 4-5 weeks
- Usually self-limited; does not typically cause chronic hepatitis (except in immunocompromised hosts)
- Pregnant women are uniquely vulnerable - fulminant hepatic failure occurs in up to 20-25% of pregnant women infected in the 3rd trimester, especially with HEV genotype 1 (high mortality rate in endemic regions)
- HEV genotype 3/4 (zoonotic) can cause chronic infection in solid organ transplant recipients and HIV patients
- Waterborne epidemics in developing countries (South Asia, Sub-Saharan Africa, Mexico)
- Diagnosis: serum IgM/IgG antibodies; PCR for HEV RNA
- No vaccine approved outside China; ribavirin used for chronic HEV in immunocompromised patients
Pathology: Acute vs. Chronic Hepatitis
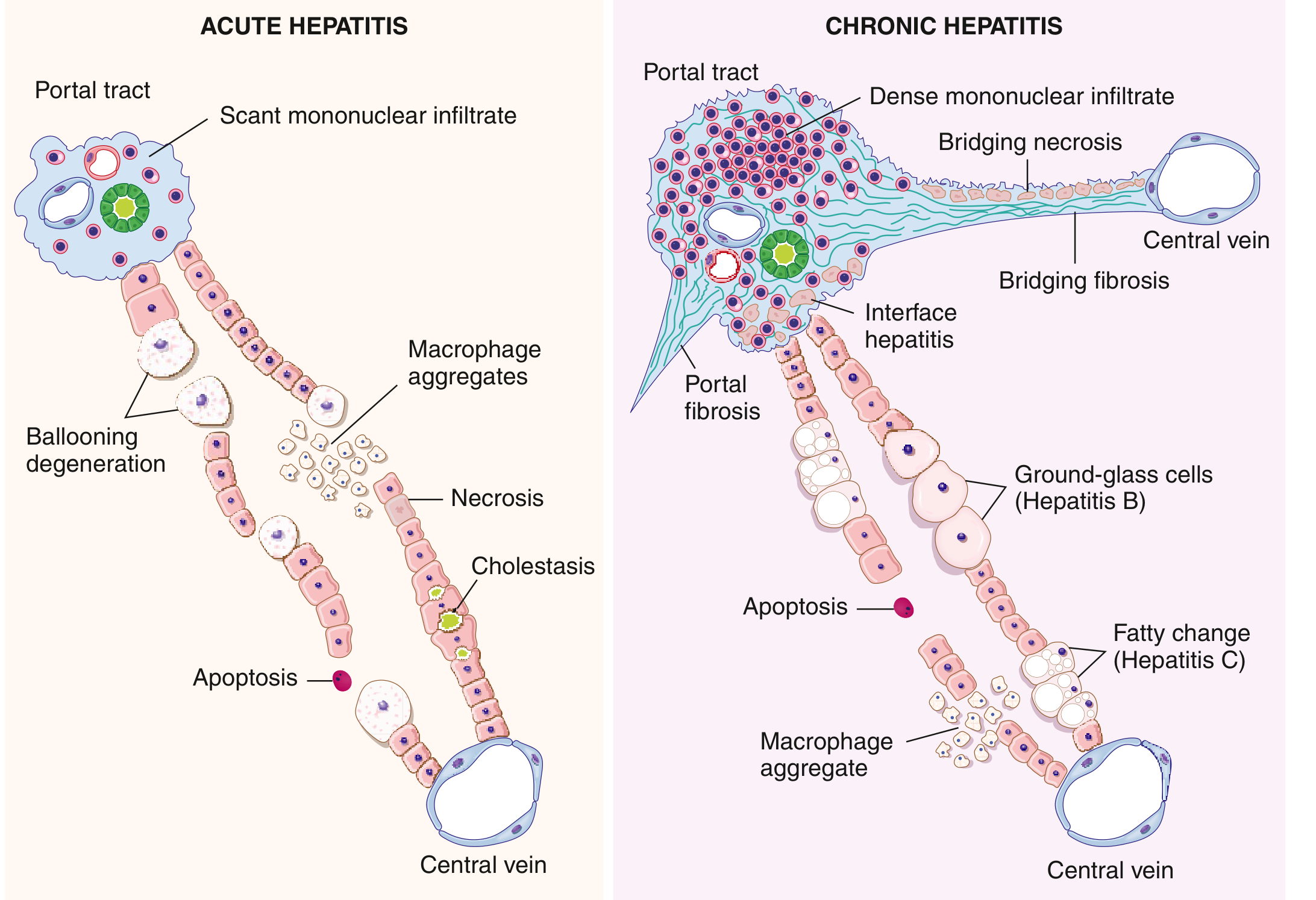
Acute Viral Hepatitis (Microscopy)
- Portal and lobular lymphocytic infiltrate (variably with plasma cells and eosinophils)
- Ballooning degeneration of hepatocytes
- Apoptosis (acidophil/Councilman bodies - shrunken, densely eosinophilic hepatocytes)
- Necrosis: may be focal, confluent, or bridging (portal-to-central) in severe cases
- Cholestasis (bile plugs in canaliculi)
- Panlobular or panacinar necrosis = fulminant hepatitis (massive liver failure)
- Macrophage aggregates at sites of necrotic hepatocytes
Chronic Viral Hepatitis (Microscopy)
-
Dense portal lymphoplasmacytic infiltration - the defining feature
-
Interface hepatitis (piecemeal necrosis): inflammatory cells cross the limiting plate and damage periportal hepatocytes
-
Portal and periportal fibrosis → bridging fibrosis (porto-portal and porto-central) → cirrhosis
-
Specific features by virus:
- Hepatitis B: "ground-glass" hepatocytes (HBsAg-laden ER visible on H&E) and "sanded nuclei" (HBcAg)
- Hepatitis C: fatty change (steatosis), lymphoid aggregates in portal tracts, bile duct damage
-
Robbins & Kumar Basic Pathology, p. 604-606
Clinicopathologic Syndromes
1. Asymptomatic Infection
Most common outcome with HCV (85% of acute infections); also common with HBV in adults
2. Acute Symptomatic Hepatitis
Phases:
- Prodromal (pre-icteric): malaise, fatigue, anorexia, nausea, vomiting, right upper quadrant discomfort, low-grade fever (1-2 weeks)
- Icteric (jaundice) phase: dark urine (bilirubinuria), pale stools, jaundice, tender hepatomegaly; transaminases (ALT > AST) may be 10-40x normal
- Recovery phase: symptoms resolve, liver enzymes normalize
3. Fulminant Hepatitis (Acute Liver Failure)
- Massive hepatic necrosis with encephalopathy within 8 weeks of onset
- Rare but life-threatening; may require emergency liver transplantation
- HAV: ~0.1%; HBV: ~1%; HDV coinfection: higher risk
- HEV in pregnancy: up to 20-25% fulminant failure rate
4. Chronic Hepatitis
- Defined as hepatic inflammation persisting beyond 6 months
- May be asymptomatic or present with fatigue, RUQ discomfort, stigmata of chronic liver disease
- Graded (degree of inflammation) and staged (degree of fibrosis) on biopsy
5. Carrier State
- Individuals who harbor the virus without significant liver disease
- HBV: >90% of perinatally infected individuals become carriers in endemic regions
- Important reservoirs of transmission
Diagnosis Summary
| Condition | Key Tests |
|---|---|
| Acute HAV | IgM anti-HAV |
| Immunity/past HAV | IgG anti-HAV |
| Acute HBV | HBsAg + IgM anti-HBc |
| Window period HBV | IgM anti-HBc (HBsAg has cleared, anti-HBs not yet appeared) |
| Chronic HBV | HBsAg >6 months, IgG anti-HBc, HBV DNA |
| Past HBV / immunity | Anti-HBs + anti-HBc |
| Vaccination immunity | Anti-HBs alone |
| Acute/chronic HCV | Anti-HCV ELISA + confirmatory HCV RNA PCR |
| Chronic HCV activity | HCV RNA quantification |
| HDV | Anti-HDV IgM/IgG; HDV RNA |
| Acute HEV | IgM anti-HEV; HEV RNA (PCR) |
Prevention
| Virus | Prevention |
|---|---|
| HAV | Inactivated vaccine (2-dose series); good sanitation |
| HBV | Recombinant HBsAg vaccine (3-dose series); neonatal vaccination in endemic areas; HBIG for post-exposure prophylaxis |
| HCV | No vaccine; harm reduction (clean needles, IVDU programs); blood screening |
| HDV | HBV vaccination prevents HDV |
| HEV | Sanitation; vaccine available in China (Hecolin); ribavirin in chronic immunocompromised cases |
Complications
All forms of chronic viral hepatitis share a common pathway to:
- Cirrhosis - irreversible fibrotic replacement of liver parenchyma
- Portal hypertension - varices, ascites, splenomegaly
- Hepatocellular carcinoma (HCC) - particularly with chronic HBV (can occur even without cirrhosis) and HCV (almost always via cirrhosis)
- Hepatic encephalopathy - in decompensated cirrhosis
- Extrahepatic manifestations: cryoglobulinemia (HCV), vasculitis, glomerulonephritis
A 2026 umbrella review of 15 meta-analyses (PMID 41794163) found that underlying viral hepatitis influences immunotherapy outcomes in advanced HCC - an important emerging clinical consideration.
Sources:
- Robbins & Kumar Basic Pathology, pp. 598-607
- Goldman-Cecil Medicine International Edition, Chapter 134 (Acute Viral Hepatitis)
- Sleisenger and Fordtran's Gastrointestinal and Liver Disease
- Petrelli F, et al. Viral hepatitis and immunotherapy outcome in advanced HCC. Crit Rev Oncol Hematol, 2026 May. PMID 41794163
This is a shared conversation. Sign in to Orris to start your own chat.