Calcium metabolism Covering urinary calcium excretion Gi regulation of calcium absorption Total adjusted calcium Calcium sensing receptors Renal handling of calcium Role of PTH in calcium metabolism Hypercalcaemia Hypocalcemia Explain all this to me in simplified manner
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Finding Sources
Finding Sources
I now have very comprehensive content from Harrison's 22E and other authoritative sources. Let me compile the full detailed answer.
Calcium Metabolism - Complete Guide
Sources: Harrison's Principles of Internal Medicine 22E (2025), Textbook of Family Medicine 9e, Goldman-Cecil Medicine
The Big Picture: Why Does Calcium Matter?
Calcium is the most abundant mineral in the body. The body holds 1-2 kg of calcium, with >99% stored in bone. The remaining ~1% circulates in blood and body fluids, yet this tiny fraction is tightly regulated because calcium controls:
- Neuromuscular excitability (nerve firing, muscle contraction)
- Cardiac rhythm
- Hormone secretion
- Intracellular signaling
Normal total serum calcium: 2.2-2.6 mmol/L (8.5-10.5 mg/dL)
The Calcium Homeostasis Diagram
This diagram shows the daily flows keeping calcium balanced:

From Harrison's 22E - Calcium flux per day across intestine, kidney, and bone. The ECF pool (1-2 g) is tiny but tightly controlled.
1. Blood Calcium: The Three Fractions
Total blood calcium has three forms:
| Fraction | % of Total | Notes |
|---|---|---|
| Ionized (free) | ~50% | The biologically active form; 1.1-1.3 mmol/L |
| Protein-bound | ~40% | Mostly to albumin; inactive |
| Complexed | ~10% | Bound to phosphate, citrate, sulfate |
Only ionized calcium matters clinically - it's what the body "feels" and regulates.
2. Total Adjusted (Corrected) Calcium
Because ~40% of calcium is bound to albumin, a low albumin gives a falsely low total calcium reading, even though the physiologically active ionized calcium is normal.
Correction formula:
Corrected Ca (mg/dL) = Measured Ca + 0.8 × (4.0 - serum albumin g/dL)
- For every 1 g/dL drop in albumin below 4.0, add 0.8 mg/dL to the measured total calcium
- Similarly, a deficit in immunoglobulins is corrected at 0.5 mg/dL per 1 g/dL deficit
Important caveat: This correction is only a rough approximation. In acute illness, always measure ionized calcium directly with a calcium-selective electrode. Acidosis raises ionized calcium (less protein binding); alkalosis lowers it.
3. GI Regulation of Calcium Absorption
The gut absorbs dietary calcium by two mechanisms working side by side:
A) Passive (Paracellular) Absorption
- Happens throughout the intestine, down a concentration gradient
- Accounts for ~5% of daily intake
- Not regulated - just depends on how much calcium is in the gut lumen
B) Active (Transcellular) Absorption - the regulated route
- Occurs mainly in the duodenum and proximal jejunum
- Calcium enters intestinal cells through the TRPV6 channel on the luminal side
- Transported across the cell bound to calbindin protein
- Pumped out the basolateral side into blood
- This active pathway is switched on by 1,25(OH)₂D (calcitriol) - the active form of Vitamin D
- Normally accounts for 20-70% of dietary calcium absorption
Vitamin D Activation Pathway
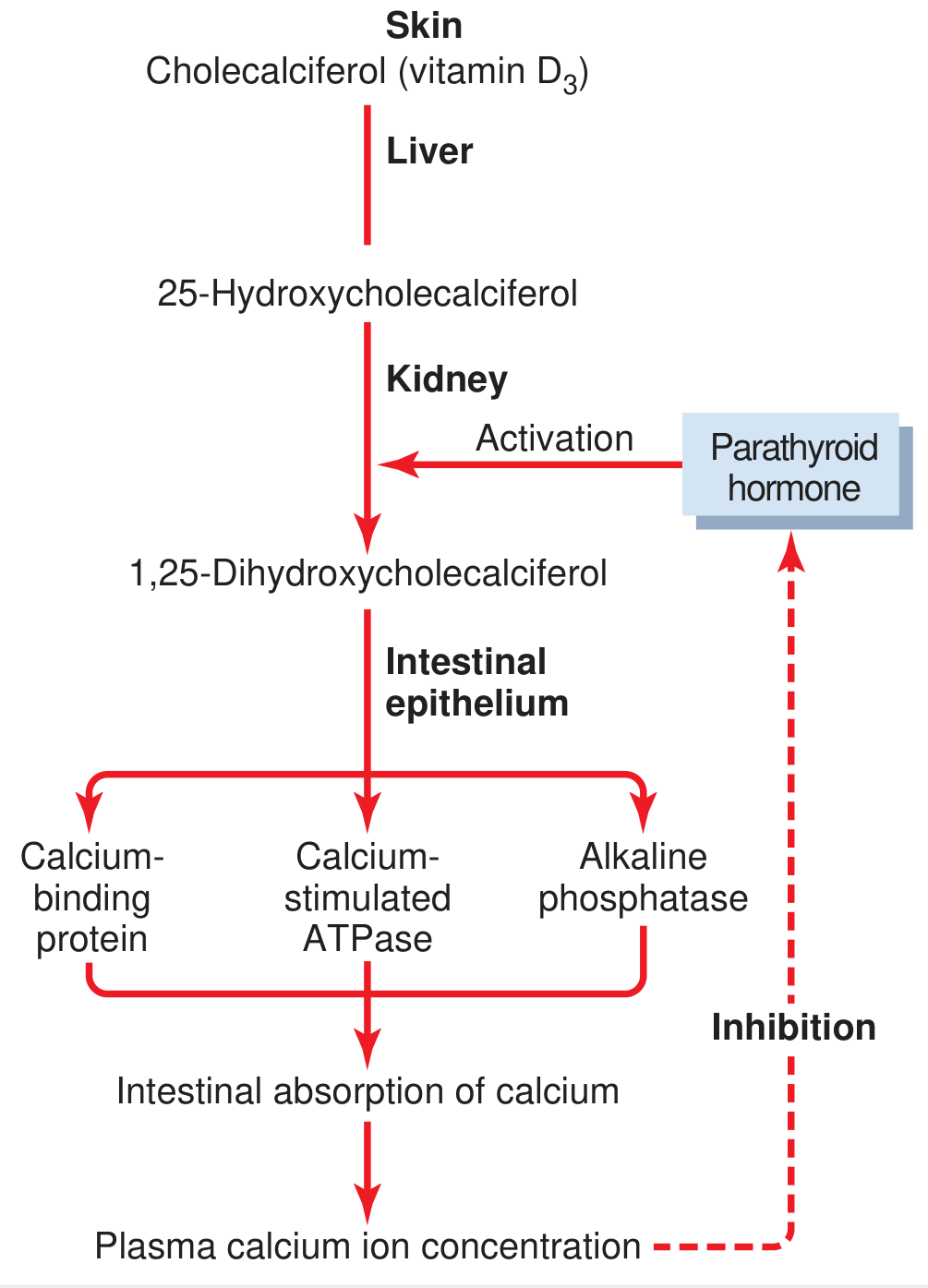
Skin → Cholecalciferol (D3) → Liver → 25-OH-D → Kidney (activated by PTH) → 1,25(OH)₂D (calcitriol) → Intestine: induces calcium-binding protein, Ca-ATPase, and alkaline phosphatase → Increased calcium absorption.
Factors Reducing Calcium Absorption
- Achlorhydria (low stomach acid) - calcium carbonate needs acid to dissolve; calcium citrate is better in these patients
- Bariatric surgery
- Pancreatic/biliary insufficiency (calcium binds unabsorbed fats)
- High calcium intake suppresses 1,25(OH)₂D synthesis (negative feedback)
- Low calcium intake does the opposite - stimulates 1,25(OH)₂D
Net result: Despite wide swings in dietary intake (400-1500 mg/day), feedback regulation keeps net intestinal absorption relatively constant at ~200-400 mg/day.
4. Calcium-Sensing Receptor (CaSR)
The CaSR is the body's calcium sensor - the molecular "thermostat" for calcium homeostasis.
Where it lives:
- Parathyroid glands (primary location - controls PTH release)
- Thick ascending limb (TAL) of renal tubule (controls urinary calcium excretion)
- Thyroid C-cells, bone, intestine, and brain
How it works:
When blood Ca²⁺ rises → CaSR on parathyroid cells is activated → 3 simultaneous effects:
- Degrades PTH mRNA
- Promotes cleavage of PTH into inactive fragments
- Suppresses release of PTH granules
The result: PTH falls rapidly, reducing bone resorption, renal calcium retention, and vitamin D activation. Blood calcium drops back to normal.
In the kidney's TAL: When blood calcium is high, CaSR activation inhibits paracellular calcium reabsorption, causing more calcium to spill into the urine - an elegant, PTH-independent feedback mechanism.
Clinical relevance - CaSR mutations:
- Loss-of-function mutation (heterozygous) → Familial Hypocalciuric Hypercalcemia (FHH) - the "thermostat" is reset high; mild asymptomatic hypercalcemia with low urinary calcium - benign, no surgery needed
- Gain-of-function mutation (activating) → Autosomal Dominant Hypocalcemia - the "thermostat" is reset low; persistent hypocalcemia with low PTH
- Calcimimetics (e.g., cinacalcet) are drugs that activate the CaSR to suppress PTH in hyperparathyroidism
5. Renal Handling of Calcium
The kidneys filter roughly 8-10 g/day of calcium - a massive load. Only 100-200 mg/day (1-2%) ends up in the urine. The rest is reclaimed in four distinct nephron segments:
| Nephron Segment | % Reabsorbed | Mechanism | Regulated? |
|---|---|---|---|
| Proximal tubule | ~65% | Passive paracellular (follows NaCl and water) | No |
| Thick ascending limb (TAL) | ~20% | Passive paracellular via paracellin-1/Claudin-14 | By CaSR |
| Distal convoluted tubule (DCT) | ~10% | Active transcellular via TRPV5 channel | Yes - by PTH, 1,25D |
| Collecting duct | Small amount | Minor | Minor |
Key point: The DCT is the fine-tuning site. PTH dramatically increases calcium reabsorption here. This is why PTH raises serum calcium partly by telling the kidney to keep more calcium.
Urinary Calcium Excretion
- Normal: 100-300 mg/day in adults
- Hypercalciuria: > 300 mg/day (men), > 250 mg/day (women) - major risk factor for kidney stones
- PTH reduces urinary calcium excretion (increases reabsorption in DCT)
- High serum calcium activates renal CaSR → inhibits TAL reabsorption → increases urine calcium
- Thiazide diuretics reduce urinary calcium (used therapeutically in hypercalciuria/stone disease)
- Loop diuretics (furosemide) increase urinary calcium loss
6. Role of PTH in Calcium Metabolism
PTH (Parathyroid Hormone) is an 84-amino acid peptide secreted by the 4 parathyroid glands. It is the single most important acute regulator of calcium.
What triggers PTH release: Low ionized calcium detected by CaSR (+ low 1,25D, low Mg)
PTH's three-pronged defense against low calcium:
A) Bone - Release calcium from the skeleton
- Activates osteoclasts (bone breakdown cells) to resorb bone and release Ca²⁺ and phosphate into blood
- Acts quickly (within hours)
B) Kidney - Save calcium, dump phosphate
- Increases Ca²⁺ reabsorption in the DCT (keeps calcium)
- Decreases phosphate reabsorption in the proximal tubule (wastes phosphate in urine) - this is why PTH excess causes hypophosphatemia
- Activates 1-alpha hydroxylase → converts 25-OH-D to active 1,25(OH)₂D → more intestinal calcium absorption (indirect effect, takes hours-days)
C) Intestine (indirect via Vitamin D)
- PTH stimulates renal 1,25(OH)₂D production → 1,25(OH)₂D then increases intestinal calcium absorption
Net result of PTH action: Blood calcium rises. Phosphate falls (the phosphaturic effect).
Negative feedback loop:
Rising calcium → activates parathyroid CaSR → PTH suppressed → calcium falls back to normal
7. Hypercalcemia
Definition: Serum calcium > 10.5 mg/dL (> 2.6 mmol/L)
The Classic Mnemonic: "Bones, Stones, Moans, and Groans"
- Bones - bone pain, pathologic fractures
- Stones - renal calculi, nephrocalcinosis
- Moans - psychiatric: depression, confusion, psychosis
- Groans - GI: nausea, vomiting, constipation, anorexia
- (Plus: polyuria, polydipsia, fatigue, muscle weakness, shortened QT interval)
Causes - Divided into Two Groups:
PRIMARY causes (excess PTH):
| Cause | % of Cases |
|---|---|
| Solitary parathyroid adenoma | ~80% |
| Parathyroid hyperplasia (all 4 glands) | ~15% |
| Multiple parathyroid adenomas | 2-4% |
| Parathyroid carcinoma | <1% |
| MEN-I, MEN-IIA (familial) | Rare |
SECONDARY / other causes:
- Malignancy (most common in hospitalized patients) - either osteolytic bone mets (myeloma, breast cancer) or PTHrP secretion (PTH-related peptide - "humoral hypercalcemia of malignancy"); calcium often >14 mg/dL
- Granulomatous disease (sarcoidosis, TB) - macrophages produce excess 1,25(OH)₂D
- Thyrotoxicosis
- Vitamin D toxicity
- Immobilization
- Milk-alkali syndrome
- Thiazide diuretics
- Familial Hypocalciuric Hypercalcemia (CaSR loss-of-function)
Distinguishing Primary HPT from Malignancy:
- In primary HPT: PTH is elevated (the problem source) - asymptomatic, found incidentally
- In malignancy: PTH is suppressed (osteolysis is the driver) - usually symptomatic, calcium >14
Management of Hypercalcemia:
- IV normal saline (volume expansion) - first and most important step
- Loop diuretics (furosemide) - increase urinary calcium loss after volume repleted
- Bisphosphonates (zoledronate, pamidronate) - inhibit osteoclasts; standard for malignancy-associated hypercalcemia
- Calcitonin - rapid but short-acting; useful early
- Steroids - effective for sarcoidosis, vitamin D toxicity, myeloma
- Cinacalcet (calcimimetic) - activates CaSR; lowers PTH in primary HPT
- Surgery (parathyroidectomy) - definitive treatment for symptomatic primary HPT
8. Hypocalcemia
Definition: Serum calcium < 8.5 mg/dL (< 2.2 mmol/L), or ionized calcium < 1.1 mmol/L
Symptoms - Due to Neuromuscular Irritability:
- Chvostek's sign - tap the facial nerve just in front of the ear → facial muscle twitching
- Trousseau's sign - inflate BP cuff above systolic for 3 min → carpal spasm (most specific)
- Perioral and fingertip tingling (paresthesias)
- Muscle cramps, tetany
- Seizures (generalized)
- Anxiety, confusion, psychosis
- Prolonged QT interval on ECG → life-threatening arrhythmia
- Hyperactive deep tendon reflexes
Severity is determined by the ionized calcium level AND the rapidity of the fall. Alkalosis worsens symptoms by shifting more calcium to the protein-bound form.
Causes:
A) PTH-deficient (hypoparathyroidism):
- Post-surgical (most common) - accidental removal of parathyroids during thyroidectomy or neck dissection
- Autoimmune hypoparathyroidism
- Infiltrative (iron overload, copper, granulomas, tumors)
- Radiation
- CaSR activating mutations (reset thermostat too low)
- Severe hypomagnesemia (Mg is required for PTH secretion AND PTH receptor action)
B) PTH-resistant (pseudohypoparathyroidism / Albright syndrome):
- PTH is elevated, but end-organs don't respond to it
- Low Ca²⁺ + high phosphate + high PTH
C) Vitamin D deficiency:
- Inadequate sun exposure, malnutrition, malabsorption
- Most common worldwide cause of hypocalcemia
D) "Hungry Bone Syndrome":
- After parathyroidectomy for severe HPT - the suddenly PTH-deprived skeleton rapidly takes up calcium from blood
E) Hyperphosphatemia:
- Renal failure → phosphate retention → calcium-phosphate complexes → less free Ca²⁺
Management:
- Acute/severe symptomatic (tetany, seizures, QT prolongation): IV calcium gluconate (not bolus - can cause cardiac arrest; give slowly)
- Concurrent: Correct hyperphosphatemia, alkalosis, hypomagnesemia
- Chronic: Oral calcium supplements + vitamin D (calcitriol in hypoparathyroidism since the kidney cannot activate vitamin D without PTH)
- Thiazide diuretics - useful adjunct in hypoparathyroidism (reduce urinary calcium loss)
Summary: The Calcium Control Loop
Low blood Ca²⁺
↓
CaSR on parathyroid glands detects the drop
↓
PTH secreted ↑↑
↓
THREE simultaneous actions:
1. Bone → osteoclast activation → Ca²⁺ released from skeleton
2. Kidney → DCT reabsorbs more Ca²⁺ + wastes phosphate
3. Kidney → activates 1,25(OH)₂D → gut absorbs more Ca²⁺
↓
Blood Ca²⁺ rises → CaSR detects it → PTH suppressed → back to normal
| Hormone | Bone | Kidney | Gut | Net Effect on Ca |
|---|---|---|---|---|
| PTH ↑ | Resorption ↑ | Ca retention ↑, PO₄ loss | D3 activation → absorption ↑ | Ca ↑, PO₄ ↓ |
| 1,25(OH)₂D ↑ | Resorption ↑ | Minor Ca retention | Absorption ↑↑ | Ca ↑ |
| Calcitonin ↑ | Resorption ↓ | Ca excretion ↑ | Minimal | Ca ↓ |
Sources: Harrison's Principles of Internal Medicine 22E (2025, McGraw Hill); Textbook of Family Medicine 9e; Goldman-Cecil Medicine International Edition
This is a shared conversation. Sign in to Orris to start your own chat.