Tb
Reading File
Asking for Preferences
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Loading Image
Loading Image
I now have comprehensive material. Here is a detailed, well-structured answer on the diagnosis and investigations of TB.
Tuberculosis (TB) - Diagnosis & Investigations
1. Clinical Suspicion - When to Investigate
Clinical suspicion is the first step. Key symptoms include:
- Cough - persistent, productive, often with mucus or blood (note: 10-25% of bacteriologically confirmed TB patients do not report cough)
- Systemic symptoms - fever, night sweats, weight loss
- Hemoptysis - seen with more extensive disease
- Lymphadenopathy - especially in HIV-positive patients
Risk factors that heighten suspicion include: HIV infection, recent exposure to a known case, immunosuppression, residence in high-incidence areas, and certain occupational exposures. Using a broader symptom screen (any one of: cough of any duration, fever, night sweats, or weight loss) in high-risk groups gives a negative predictive value of ~97.7% for TB.
- Murray & Nadel's Textbook of Respiratory Medicine, p. 1187-1188
2. Chest Radiograph
The CXR is usually the first investigation and is highly informative, though not diagnostic on its own.
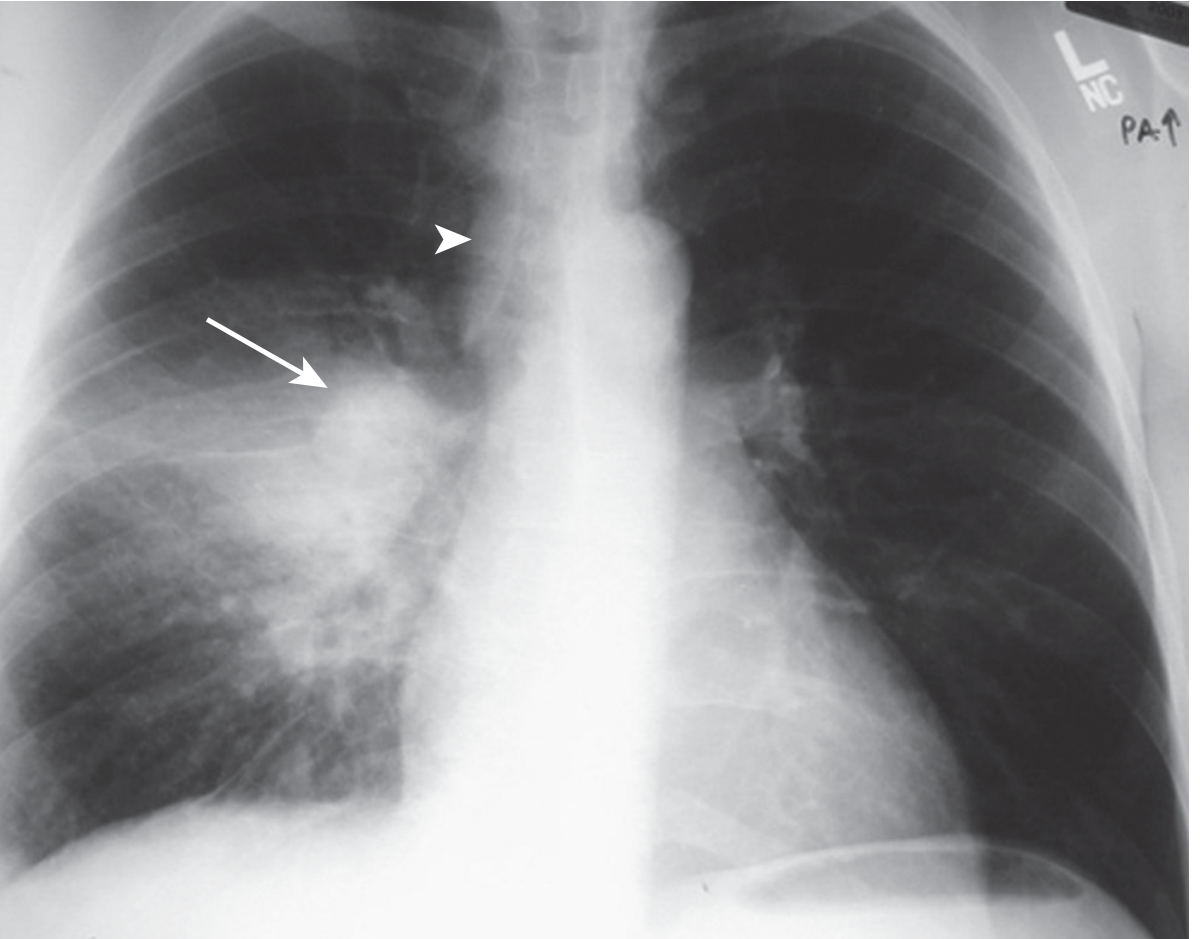
Primary TB:
- Middle or lower lung zone consolidation with ipsilateral hilar/paratracheal lymphadenopathy
- Atelectasis from airway compression
- May show pleural effusion
Primary TB (right lower lobe consolidation + right hilar lymphadenopathy):
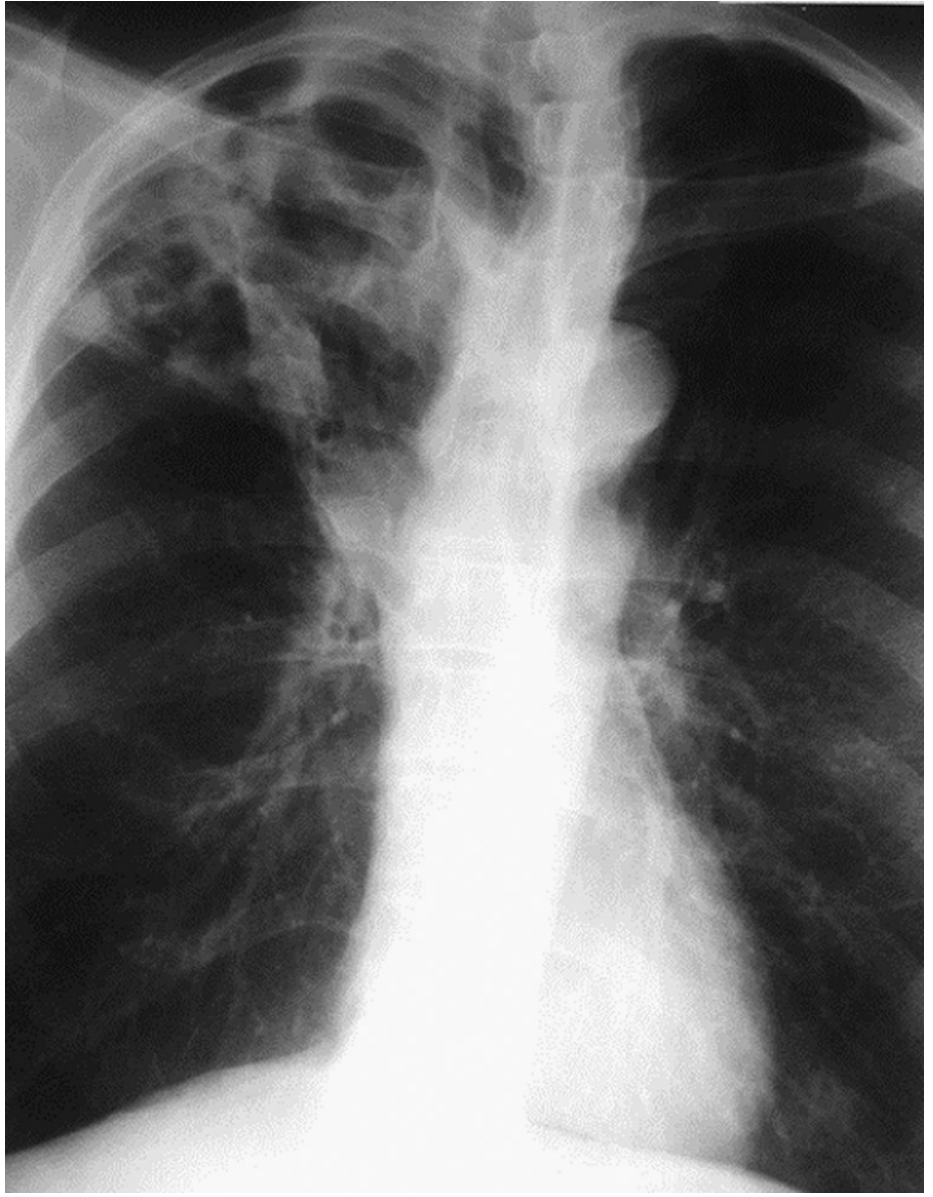
Reactivation (Post-primary) TB:
- Upper lobe involvement (apical and posterior segments of right upper lobe; apical-posterior segment of left upper lobe)
- Cavitation is common
- Fibrotic scarring with lung shrinkage and calcification on healing
- Bronchogenic spread can cause lower lobe opacities
- Miliary pattern if hematogenous dissemination occurs
Cavitary TB (right upper lobe):
In HIV:
- Early HIV - typical upper lobe pattern
- Advanced HIV (low CD4) - atypical pattern: lower zone / diffuse opacities, intrathoracic adenopathy, less cavitation
Limitation: CXR cannot determine activity from a single film alone, and cannot give a definitive diagnosis. Microbiologic evaluation is always needed.
- Murray & Nadel's Textbook of Respiratory Medicine, p. 1188-1189
3. Microbiological Tests
A. AFB Smear Microscopy (Ziehl-Neelsen / fluorescence stain)
- Collect at least 2 sputum specimens (US: 3 specimens are routine)
- Specimens include: early morning sputum, spot sputum, induced sputum, BAL (if unable to produce)
- Sensitivity: up to 90% with 3 specimens; however, often lower in paucibacillary disease
- AFB smear cannot distinguish M. tuberculosis from non-tuberculous mycobacteria (NTM)
- Remains the most widely available test globally
B. Mycobacterial Culture
-
More sensitive than smear (~100% when adequate sputum is provided)
-
Results take 2-8 weeks (liquid culture faster than solid media)
-
Definitive identification of M. tuberculosis complex
-
Also allows drug susceptibility testing (DST)
-
Requires specialized lab infrastructure; often unavailable in resource-limited settings
-
Textbook of Family Medicine, 9e, p. 763
C. Nucleic Acid Amplification Testing (NAAT) - Xpert MTB/RIF
This is the most significant advance in rapid TB diagnosis:
-
Xpert MTB/RIF (GeneXpert): Self-contained, automated, results in ~90 minutes
-
Simultaneously detects M. tuberculosis complex AND rifampicin resistance (as a proxy for MDR-TB)
-
Distinguishes M. tuberculosis from NTM (unlike smear)
-
Interpretation:
- AFB smear-positive + NAAT-positive = rapid confirmation of TB
- AFB smear-negative + NAAT-positive = presumptive evidence in intermediate/high-probability cases
- NAAT-negative does NOT exclude active TB (insufficient sensitivity to replace culture)
-
WHO recommendation: Preferred initial test for all adults/children with suspected TB where feasible, especially for HIV-positive patients and those at risk of MDR-TB
-
US recommendation: Use as adjunct to smear + culture
-
Murray & Nadel's Textbook of Respiratory Medicine, p. 1189-1193
D. Line Probe Assays (LPAs)
- Molecular test detecting resistance to isoniazid, rifampin, fluoroquinolones, and injectables
- Useful for rapid MDR-TB and XDR-TB screening
- Applied to culture isolates or directly to smear-positive specimens
4. Tests for TB Infection (Latent TB)
These tests measure the host immune response and cannot distinguish latent from active TB. They are used for screening/infection detection.
A. Tuberculin Skin Test (TST / Mantoux)
- Intradermal injection of PPD (purified protein derivative)
- Read at 48-72 hours; induration measured in mm
- Cutoffs:
- ≥5 mm: HIV-infected, close contacts, immunosuppressed, CXR with fibrotic changes
- ≥10 mm: Recent immigrants, IV drug users, high-risk occupational groups, children <4 yrs
- ≥15 mm: No known risk factors
- Limitations:
- False-negative: immunosuppression, overwhelming TB, very early infection
- False-positive: prior BCG vaccination, NTM infection
- Low specificity due to cross-reactivity with conserved mycobacterial proteins
- Operator-dependent; batch variations
B. Interferon-Gamma Release Assays (IGRAs)
- Measure T-cell IFN-γ release in response to TB-specific antigens ESAT-6 and CFP-10 (RD1-encoded, absent from BCG and most NTMs)
- Types:
- QuantiFERON-TB Gold Plus (QFT-Plus): Whole-blood ELISA; measures both CD4+ and CD8+ T-cell responses
- T-SPOT.TB (Oxford Immunotec): ELISPOT assay
- Advantages over TST: Higher specificity; not affected by BCG vaccination; no booster effect; single visit
- Limitations: False-negatives in immunosuppressed; higher cost; need lab processing
C. New Antigen-Based Skin Tests (TBSTs)
-
Use ESAT-6 and CFP-10 antigens (same as IGRAs) but in skin-test format
-
WHO assessment: accuracy similar to IGRAs and greater than TST
-
Useful also for HIV-positive individuals, children, and BCG-vaccinated persons
-
Harrison's Principles of Internal Medicine 22E (2025), p. 1437
5. Non-Sputum-Based Tests
Urine LAM (Lipoarabinomannan) Antigen Test
-
Detects LAM - a mycobacterial cell-wall component - in urine
-
Particularly useful when sputum cannot be produced
-
Best performance in: HIV-positive patients with low CD4 counts (<200 cells/µL)
- Pooled sensitivity 42-62% (higher in hospitalized, symptomatic, low-CD4 patients)
- Pooled specificity ~91%
-
WHO recommendation: Recommended for all HIV-positive inpatients with TB symptoms, regardless of CD4 count; and for outpatients with CD4 <100 cells/µL
-
Not currently available in the US
-
Murray & Nadel's Textbook of Respiratory Medicine, p. 1193
6. Additional Investigations
| Investigation | Role |
|---|---|
| CT Chest | Better than CXR for cavitation, adenopathy, miliary disease, pleural disease; helpful when CXR is ambiguous |
| Bronchoscopy + BAL | When sputum cannot be obtained; allows smear, culture, NAAT of BAL fluid |
| Pleural fluid analysis | For TB pleuritis: exudate, lymphocyte-predominant; ADA elevated; pleural biopsy (granulomas + culture) has higher yield than fluid alone |
| Tissue biopsy | For extrapulmonary TB (lymph node, bone, pleura) - histology shows caseating granulomas; AFB stain + culture |
| PCR on non-sputum specimens | High specificity when positive; useful for pleural biopsy material; sensitivity too low (~30%) to exclude diagnosis |
| FNA (lymph node) | Useful in scrofula / extrapulmonary TB |
7. Summary Algorithm
Clinical suspicion (symptoms + risk factors)
↓
Chest X-ray
↓
Sputum × 2-3 for: AFB smear + mycobacterial culture + NAAT (Xpert MTB/RIF)
↓
[If smear-negative + high suspicion] → CT chest, bronchoscopy/BAL, induced sputum
↓
[Infection screening (no active disease suspected)] → TST or IGRA
↓
[HIV-positive / cannot produce sputum] → Urine LAM + Xpert
↓
Definitive diagnosis = positive culture OR positive NAAT (with clinical correlation)
Key points to remember:
- Smear alone cannot confirm TB species - NAAT distinguishes M. tuberculosis from NTM
- A single negative NAAT does not rule out active TB - culture remains the gold standard
- TST and IGRAs detect infection, not active disease
- Radiographs are suggestive but never diagnostic; microbiologic confirmation is always needed
- In HIV, expect atypical presentations and use urine LAM + Xpert as initial tests
Sources: Harrison's Principles of Internal Medicine 22E (2025), p. 1437-1438 | Murray & Nadel's Textbook of Respiratory Medicine, p. 1187-1193
This is a shared conversation. Sign in to Orris to start your own chat.