Hiv patient in my opd how to take history
Reading File
Finding Sources
Finding Sources
Searching the Web
HIV patient history taking OPD clinical approach
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
I now have enough information from Harrison's and other authoritative sources to give a comprehensive, well-structured answer. Let me compose it now.
Taking History from an HIV Patient in OPD
Here is a systematic approach to history-taking for an HIV patient presenting in your outpatient clinic.
1. Presenting Complaint & History of Present Illness
Start with why the patient has come today. Key questions:
- What symptoms are they experiencing now? (fever, weight loss, night sweats, cough, diarrhea, oral lesions, rash, headache, visual changes)
- Duration and progression of symptoms
- Any recent hospitalization or illness
2. HIV-Specific History
Diagnosis and Timeline
- When was HIV diagnosed? How? (screening vs. symptomatic presentation)
- What stage are they at - do they know their current CD4 count and viral load?
- Have they ever been diagnosed with AIDS or an AIDS-defining illness? (see box below)
Antiretroviral Therapy (ART)
- Are they on ART currently? Which regimen?
- When was ART started? Any recent changes?
- Adherence - are they taking medication as prescribed? Any missed doses?
- Any drug toxicities or side effects experienced?
- Any history of treatment failure or resistance testing done?
3. Risk History (Elicit Sensitively and Non-Judgmentally)
This is important to understand mode of acquisition and ongoing transmission risk:
- Sexual history - number of partners, condom use, men who have sex with men (MSM), anal/vaginal/oral intercourse
- IV drug use - needle sharing, current or past
- Blood transfusion history - when, where
- Vertical transmission (in children/young patients) - maternal HIV status
- Partner's HIV status - if known
"Risk factors for HIV infection such as unprotected sexual activity and injection drug abuse should be specifically queried." - Murray & Nadel's Textbook of Respiratory Medicine
4. Opportunistic Infection (OI) Screening
Ask directly about symptoms of common OIs based on CD4 level:
| CD4 Range | Common OIs to Ask About |
|---|---|
| <500 | Candidiasis (oral/vaginal), TB, herpes zoster |
| <200 | PCP pneumonia, Toxoplasma encephalitis, Cryptococcal meningitis |
| <100 | CMV retinitis, MAC, Cryptosporidiosis |
| <50 | CMV disease, disseminated MAC, CNS lymphoma |
Ask about:
- Fever, sweats, weight loss (constitutional symptoms)
- Cough, breathlessness (PCP, TB, bacterial pneumonia)
- Diarrhea, abdominal pain (Cryptosporidium, MAC, CMV colitis)
- Headache, neck stiffness, confusion (Cryptococcal meningitis, Toxoplasma, TB meningitis)
- Visual changes, floaters (CMV retinitis)
- Oral white plaques (candidiasis), dysphagia (oesophageal candidiasis)
- Skin lesions (Kaposi's sarcoma, molluscum, herpes)
- Cognitive/mood changes (HIV encephalopathy)
5. Past Medical and Surgical History
- Prior STIs: gonorrhoea, chlamydia, syphilis, herpes (STIs increase HIV transmission risk significantly - syphilis 7-fold, herpes up to 25-fold)
- TB history or exposure - TST/IGRA result
- Hepatitis B or C co-infection
- Recurrent bacterial infections (pneumonia, sinusitis)
- Prior surgeries, blood products received
6. Drug History
- Full ART medication list - generic names, doses, timing
- Prophylaxis medications (Co-trimoxazole/TMP-SMX, fluconazole, azithromycin)
- Any other medications, herbal supplements (drug interactions are important with ART)
- Contraception (hormonal contraceptives interact with some ART)
- Allergies (especially sulfa drugs - relevant for Co-trimoxazole prophylaxis)
7. Social and Family History
- Living situation - does anyone know about the diagnosis? Support network
- Occupation - exposure risks, functional status
- Alcohol and substance use (affects adherence, liver disease)
- Diet and nutritional status
- Travel history - endemic fungal infections (histoplasmosis, coccidioidomycosis), TB exposure
8. Psychiatric and Neurological History
- Depression, anxiety, suicidal ideation (very common, affects adherence)
- Cognitive complaints - memory, concentration
- History of trauma or abuse (relevant in some populations)
"Excessive risk-taking behaviors increasing likelihood of viral exposure...higher risk for developing psychiatric symptoms in response to being HIV-positive." - Kaplan & Sadock's Comprehensive Textbook of Psychiatry
9. Immunization History
Ask if the patient has received:
- Pneumococcal vaccine
- Annual influenza and COVID-19 vaccines
- Hepatitis A and B vaccines (if seronegative)
- HPV vaccine (if indicated)
10. Review of Systems (Systematic Screen)
Go through every system quickly to catch subclinical disease:
- General: weight, appetite, fever, fatigue
- HEENT: vision changes, oral lesions, lymphadenopathy
- Respiratory: cough, dyspnoea, haemoptysis
- GI: nausea, diarrhoea, dysphagia, jaundice
- Neuro: headache, weakness, confusion, peripheral numbness/tingling
- Skin: rash, ulcers, nodules, new lesions
- Genitourinary: dysuria, discharge, ulcers
Harrison's: Initial Evaluation Checklist
After history, the initial evaluation should include (Harrison's, 22e, p. 1659):
- CD4+ T lymphocyte count
- Plasma HIV RNA (viral load)
- HIV resistance testing
- HLA-B*5701 screening (before abacavir)
- RPR/VDRL (syphilis)
- Anti-Toxoplasma antibody titer
- Hepatitis A, B, C serologies
- PPD or IFN-gamma release assay (TB)
- Fasting glucose and lipid profile
- LFTs (AST, ALT, ALP, bilirubin)
- Urinalysis, CBC, comprehensive metabolic panel
- Mini-Mental Status Examination
Key Principle: Non-Judgmental Communication
Throughout the history, maintain a patient-centred, non-judgmental approach. Normalize sensitive questions ("I ask all my patients about sexual history as part of routine care"). Use open-ended questions first, then move to specifics. Ensure confidentiality. Counsel on transmission prevention and offer partner notification support.
Sources: Harrison's Principles of Internal Medicine 22e (2025), Tintinalli's Emergency Medicine, Murray & Nadel's Textbook of Respiratory Medicine, Kaplan & Sadock's Comprehensive Textbook of Psychiatry
My patient had a weakness, headache and dizziness how to diagnose it
Reading File
Finding Sources
Finding Sources
Finding Sources
Searching the Web
headache dizziness weakness diagnostic approach clinical differential diagnosis
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Loading Image
I have a rich diagnostic flowchart and comprehensive textbook content. I now have everything needed for a thorough, well-structured answer.
Diagnosing a Patient with Weakness, Headache, and Dizziness
This is a broad symptomatic triad with a wide differential. The key is a structured approach - starting with history to categorize the symptoms, then focused examination, then targeted investigations.
Step 1: Characterize Each Symptom
A. Characterize the Dizziness First
The single most important step. Ask the patient to describe dizziness without using the word "dizzy":
| Type | Description by Patient | Likely Category |
|---|---|---|
| Vertigo | "The room is spinning" | Inner ear / CNS (brainstem, cerebellum) |
| Presyncope | "I feel like I'm about to faint / graying out" | Cardiac, vasovagal, orthostatic |
| Disequilibrium | "I feel unsteady on my feet" | Neurosensory system disturbance |
| Non-specific | "I feel floaty / lightheaded" | Often psychogenic / anxiety |
"The initial step in evaluation is a thorough history. The physician should clarify the category of dizziness... categorizing the type of dizziness can limit the differential diagnosis." - Textbook of Family Medicine 9e
Ask:
- Does the room spin, or do you feel faint?
- Is dizziness triggered by head movement (turning in bed, looking up)?
- How long does each episode last? (seconds = BPPV; hours = Meniere's; continuous = stroke)
- Does it occur on standing? (orthostatic hypotension)
B. Characterize the Headache
Ask the SOCRATES questions:
- Site - unilateral, bilateral, occipital, frontal?
- Onset - sudden ("thunderclap") vs. gradual
- Character - throbbing, pressure, band-like, stabbing
- Radiation - neck stiffness, behind eyes
- Associated symptoms - nausea, vomiting, photophobia, aura, visual changes
- Time - episodic vs. constant; duration
- Exacerbating/relieving factors - posture, exertion, lying down
- Severity - worst headache of life?
Red Flags (SNOOP4):
- Sudden onset "thunderclap" headache = subarachnoid haemorrhage until proven otherwise
- Progressive worsening headache + fever + neck stiffness = meningitis
- Headache + focal neurological deficit + weakness = stroke/tumour
- New headache in age >50 years
- Headache worse on lying down (raised ICP)
- Headache after head trauma
C. Characterize the Weakness
- Is it generalized or focal?
- Upper limb vs. lower limb, one side (hemiparesis) vs. both sides?
- Sudden onset (stroke) vs. gradual (anaemia, hypothyroidism, malignancy)
- Associated with fatigue, exertion (cardiac, anaemia)
- Muscle aches, joint pain (polymyalgia, inflammatory)
- Weight loss, night sweats (malignancy, TB, HIV)
Step 2: Key Red Flag Check (Must-Not-Miss Diagnoses)
Before assuming benign causes, actively screen for:
| Red Flag | Think |
|---|---|
| Sudden severe headache + weakness + dizziness | Stroke (CVA/TIA), subarachnoid haemorrhage |
| Headache + fever + neck stiffness | Meningitis/encephalitis |
| Positional dizziness + occipital headache | Cerebellar lesion, posterior fossa tumour |
| Weakness + postural dizziness + hyperpigmentation | Adrenal insufficiency |
| Headache + visual changes + pituitary symptoms | Pituitary apoplexy |
| Headache + papilloedema on fundoscopy | Raised intracranial pressure |
| Gradual weakness + pallor + dizziness | Severe anaemia |
"The constellation of symptoms in acute adrenal insufficiency - weakness, malaise, fatigue, nausea, dizziness - is a common diagnostic mimic and must be considered." - Rosen's Emergency Medicine
Step 3: Focused Physical Examination
Vital Signs
- BP both arms (difference >20 mmHg = subclavian steal)
- Orthostatic BP and pulse: drop >20 mmHg systolic on standing = orthostatic hypotension
- Heart rate, temperature, SpO2
Neurological Exam (most important)
- Cranial nerve assessment - facial weakness, diplopia, dysarthria, dysphagia
- Nystagmus evaluation - type and direction (bidirectional or failure to fatigue = central)
- Motor power - all 4 limbs
- Cerebellar tests - finger-nose, heel-shin, Romberg, tandem gait
- Gait assessment
- Fundoscopy - papilloedema
Cardiovascular
- Auscultation for murmurs, arrhythmia
- Carotid bruits (TIA risk)
ENT
- Otoscopy (infection, cholesteatoma)
- Rinne and Weber tests (sensorineural vs. conductive hearing loss)
General
- Pallor (anaemia), jaundice, lymphadenopathy, thyroid palpation
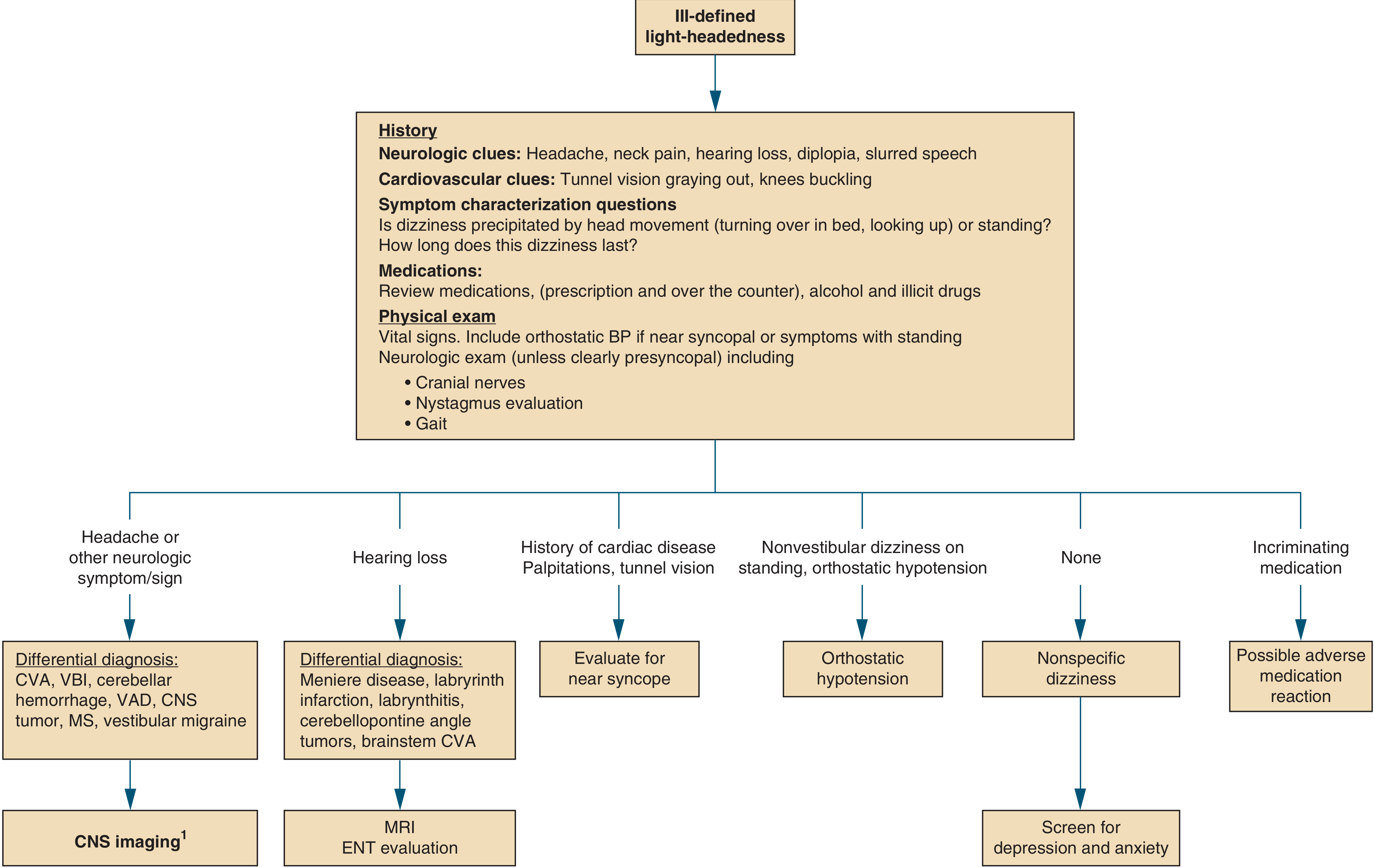
Step 4: Diagnostic Flowchart
The following chart from Symptom to Diagnosis: An Evidence-Based Guide guides the workup based on what the history and exam reveal:
Step 5: Investigations
Order based on clinical suspicion, but a standard workup includes:
First-line (all patients):
- CBC - anaemia, infection (↑ WBC = infection)
- Blood glucose - hypoglycaemia is a common cause of all three symptoms
- Renal function (BMP/electrolytes) - hyponatraemia, uraemia
- Thyroid function tests (TFTs) - hypothyroidism causes weakness, headache, dizziness
- ESR/CRP - inflammation, temporal arteritis (if >50 years old)
- ECG - arrhythmia, heart block
If neurological signs present:
- Urgent CT head (to exclude haemorrhage, tumour, mass lesion)
- MRI brain with contrast (better for posterior fossa, brainstem, MS, infarct)
- If stroke suspected: CT angiography or MR angiography
If vestibular causes suspected:
- Audiometry / ENT referral
- Dix-Hallpike maneuver (for BPPV - nystagmus on positional testing)
If systemic/metabolic causes:
- Serum cortisol (adrenal insufficiency)
- Vitamin B12 and folate levels
- LFTs
- Chest X-ray
- Iron studies (iron deficiency anaemia)
If infection suspected:
- Blood cultures, LP (if meningitis cannot be excluded - do CT head first)
Step 6: Common Differential Diagnoses Summary
| Diagnosis | Key Distinguishing Features |
|---|---|
| Tension headache | Band-like headache, bilateral, no nausea/aura; dizziness mild |
| Migraine | Unilateral, throbbing, nausea, photophobia, aura; may have vertigo (vestibular migraine) |
| BPPV | Brief episodes <1 min, triggered by head position change; Dix-Hallpike positive |
| Meniere's disease | Episodic vertigo (hours), fluctuating hearing loss, tinnitus, ear fullness |
| Stroke/TIA | Sudden onset, focal signs, risk factors (HTN, DM, AF, smoking) |
| Anaemia | Pallor, fatigue, exertional dizziness, palpitations, low Hb |
| Orthostatic hypotension | Dizziness on standing, BP drops >20 mmHg; drug-related or dehydration |
| Hypothyroidism | Gradual weakness, cold intolerance, weight gain, slow pulse, raised TSH |
| Hypertension | BP elevated; headache usually occipital, morning onset |
| Anxiety/panic disorder | Chronic non-specific dizziness, floating sensation, no neurological signs |
| CO poisoning | All three symptoms, indoor exposure, multiple family members affected |
| Adrenal insufficiency | Weakness + dizziness + hypotension + hyponatraemia + hyperpigmentation |
| Meningitis | Fever + headache + neck stiffness + photophobia - emergency |
Key Principle
The triad of weakness + headache + dizziness is non-specific. Your job is to:
- Rule out dangerous causes first (stroke, SAH, meningitis, CO poisoning)
- Then characterize the dizziness type to narrow the differential
- Look for patterns that point to a systemic vs. neurological vs. vestibular origin
Sources: Symptom to Diagnosis: An Evidence-Based Guide 4th Ed, Textbook of Family Medicine 9e, Rosen's Emergency Medicine, K.J. Lee's Essential Otolaryngology
This is a shared conversation. Sign in to Orris to start your own chat.