Pregnancy test in menstrual cycle
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Here is a thorough explanation of pregnancy tests in the context of the menstrual cycle, drawing from multiple authoritative medical textbooks.
Pregnancy Test in the Menstrual Cycle
The Menstrual Cycle - Foundation
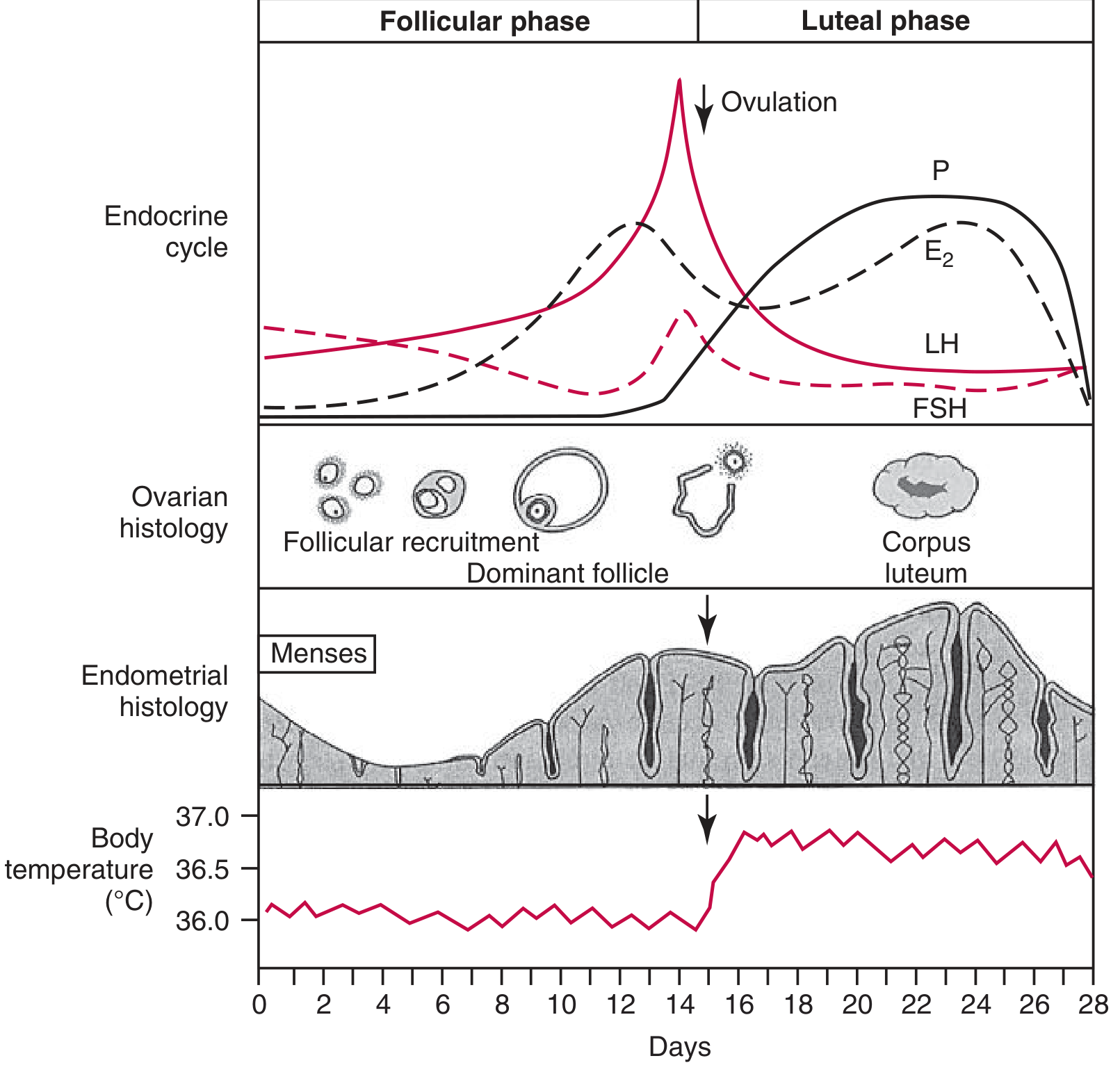
To understand when and why a pregnancy test works, you need to know what is happening hormonally across the cycle. A normal 28-day cycle has two phases:
Menstrual cycle overview - Tietz Textbook of Laboratory Medicine, 7th Edition
| Phase | Days (28-day cycle) | Key hormones |
|---|---|---|
| Follicular phase | Days 1-14 | FSH rises then falls; estradiol (E2) rises; LH surge just before ovulation |
| Ovulation | ~Day 14 | LH surge triggers release of the oocyte |
| Luteal phase | Days 15-28 | Corpus luteum secretes progesterone (P) and estrogen; if no pregnancy, corpus luteum degenerates -> menstruation |
Key points from the Tietz Textbook:
- The LH surge is a reliable predictor of ovulation, with onset occurring 16-58 hours before ovulation for 90% of women
- Cycle length variation (26-34 days) is mostly due to variation in the follicular phase, not the luteal phase
- If conception occurs, hCG from the implanting blastocyst rescues the corpus luteum, sustaining progesterone production and preventing menstruation
The Basis of the Pregnancy Test: hCG
All pregnancy tests detect beta-human chorionic gonadotropin (beta-hCG), a glycoprotein hormone secreted by trophoblast cells of the placenta after implantation.
Structure: hCG is a heterodimer with alpha and beta subunits linked by disulfide bonds. Tests target the beta subunit specifically because the alpha subunit is shared with LH, FSH, and TSH. - Henry's Clinical Diagnosis and Management by Laboratory Methods
Role of hCG in the cycle:
- hCG prevents premature degeneration (luteolysis) of the corpus luteum
- It sustains progesterone production from the corpus luteum through the first trimester
- This is why periods stop in pregnancy - the progesterone-driven endometrium is maintained
Timeline: When Does hCG Become Detectable?
The timing relative to the menstrual cycle is critical for understanding when a test will be positive:
| Event | Timing |
|---|---|
| Fertilization | ~Day 14 (ovulation) |
| Implantation | ~Days 20-23 |
| hCG detectable in serum (>5 IU/L) | 8-11 days after conception (Days 23-25 of cycle = 3rd week of pregnancy from LMP) |
| hCG detectable in urine | 1-3 days after serum detection |
| ~50% of pregnant women reach 25 IU/L | First day of missed period (Day 28-29) |
| Peak hCG concentration | ~8-10 weeks gestation (~100,000-200,000 mIU/mL) |
| hCG decline | End of 2nd trimester: 90% reduction from peak |
- Roberts and Hedges' Clinical Procedures in Emergency Medicine; Tietz Textbook of Laboratory Medicine
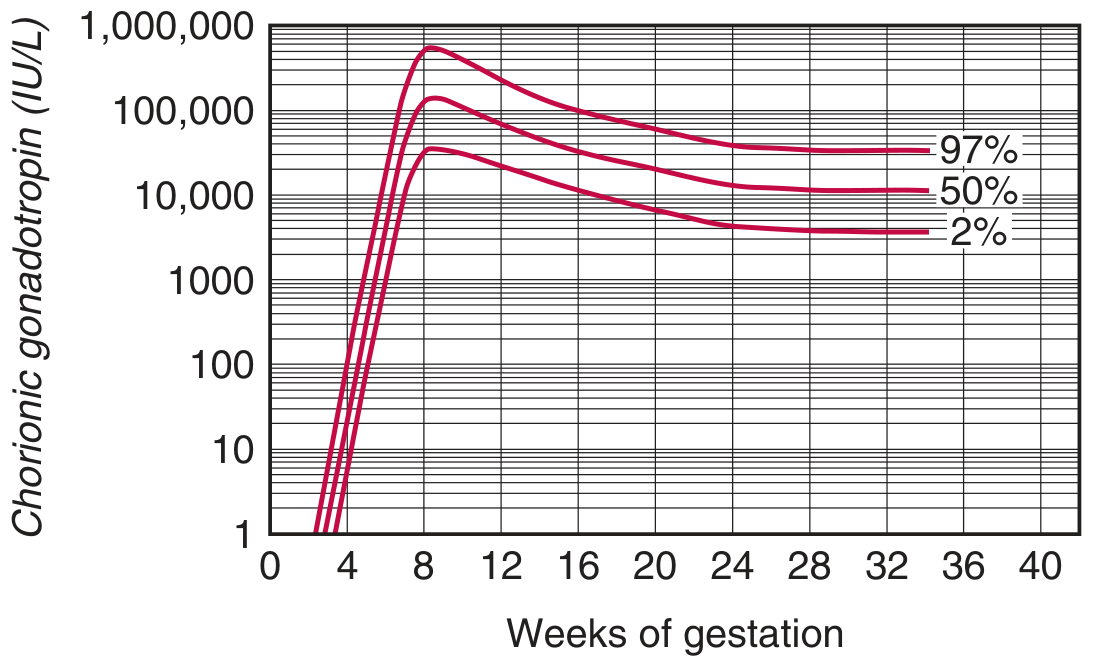
hCG rises steeply from implantation to ~8-10 weeks, then declines. - Tietz Textbook of Laboratory Medicine
Doubling time: In a healthy intrauterine pregnancy, beta-hCG doubles approximately every 2.5 days in the first 4 weeks. The doubling rate slows to every 3 days thereafter. A level that fails to increase by 66% every 48 hours has a ~75% probability of being a nonviable pregnancy. - Roberts and Hedges' Clinical Procedures in Emergency
Types of Pregnancy Tests
1. Qualitative Tests (Yes/No Result)
Urine hCG (home/POC test):
- Uses immunochromatography (lateral flow)
- Detection threshold typically 25 IU/L
- OTC home tests may detect as low as 0.5-25 IU/L (they use larger sample volumes)
- First-morning urine is preferred because it is concentrated
- Waived under CLIA '88 - can be done at home or point-of-care
- Result: colored test line = positive
Serum qualitative hCG (lab-based):
- Slightly more sensitive than urine - detects pregnancy earlier because serum hCG concentration is higher than urine
- Classified as moderately complex under CLIA - requires centrifugation, must be done in a lab
- Tietz Textbook of Laboratory Medicine, 7th Edition
2. Quantitative Tests (Serum beta-hCG Level)
- Measures exact hCG concentration (IU/L or mIU/mL)
- Detection threshold ~5 IU/L
- Used to:
- Diagnose and date early pregnancy
- Monitor pregnancy viability (serial doubling)
- Diagnose ectopic pregnancy (combined with ultrasound)
- Monitor trophoblastic disease (gestational trophoblastic tumors, choriocarcinoma)
Best Time to Perform a Pregnancy Test
| Timing | Reliability |
|---|---|
| Before missed period (early luteal phase) | May be negative even if pregnant (hCG below threshold) |
| Day of missed period | ~50% sensitivity; hCG ~25 IU/L in half of pregnant women |
| 1 week after missed period | High sensitivity; most reliable |
| Any time with missed period + symptoms | Indicated urgently (e.g., to rule out ectopic pregnancy) |
Key clinical point: Urine tests can detect pregnancy around the day of missed menses. Testing earlier (days 21-27) risks false-negative results because hCG may still be below the test threshold. - Tietz Textbook of Laboratory Medicine
False Positives and False Negatives
False positives:
- Heterophile antibodies or human anti-mouse antibodies (HAMA) in serum
- Molar pregnancy or choriocarcinoma (very high hCG)
- Delayed reading of the test result (test band darkens over time)
- Rare: tuboovarian abscess (one case report of positive urine / normal serum beta-hCG)
False negatives:
- Testing too early (hCG below threshold)
- Dilute urine (not first-morning specimen)
- Hook effect - extremely high hCG (e.g., complete mole) can saturate antibodies and produce false negative on some assays
- hCG beta-core fragment in urine (predominant after 5th week) can competitively inhibit the test
- Tietz Textbook of Laboratory Medicine; Roberts and Hedges' Clinical Procedures in Emergency
Whole Blood as an Alternative Specimen
In emergency settings, when urine is unavailable (e.g., hypotensive patient with suspected ectopic pregnancy), whole blood can be placed directly into standard urine dipstick devices and has been validated as a reliable alternative. This can be lifesaving for timely recognition of ectopic pregnancy. - Roberts and Hedges' Clinical Procedures in Emergency Medicine
Summary Diagram
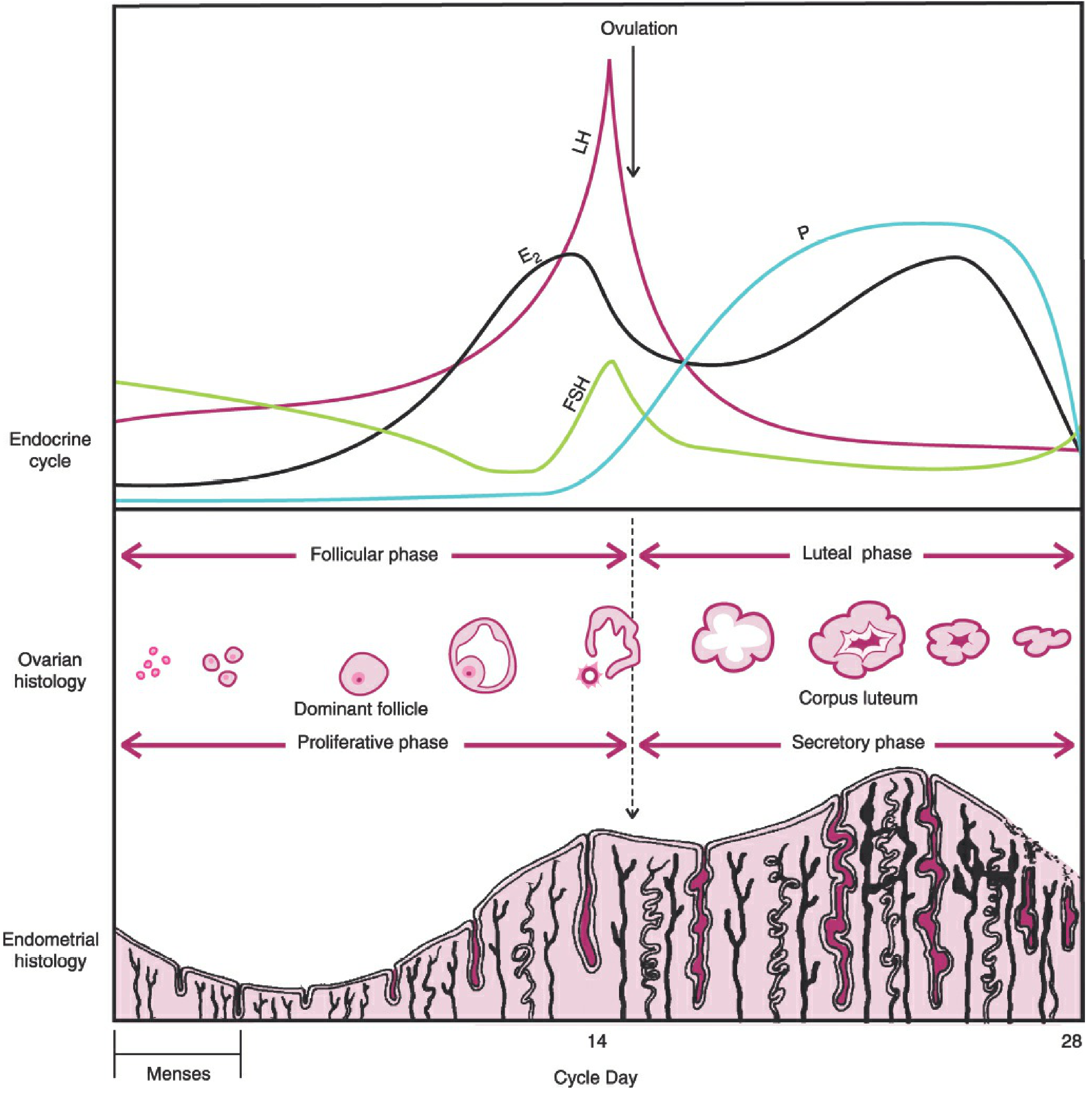
The menstrual cycle - Berek & Novak's Gynecology
In brief: Pregnancy tests detect beta-hCG, which appears in blood ~8-11 days after conception (implantation), and in urine 1-3 days later. The test is most reliable at or after the first missed period. Serial quantitative beta-hCG levels (doubling every 48-72h) confirm a healthy intrauterine pregnancy; failure to double suggests ectopic pregnancy or miscarriage.
Pregnancy test in menstrual cycle very short notes
Pregnancy Test in Menstrual Cycle - Short Notes
What is Detected?
- All pregnancy tests detect beta-hCG (beta-human chorionic gonadotropin)
- Secreted by trophoblast cells after implantation of the blastocyst
hCG & The Menstrual Cycle
| Event | Day (28-day cycle) |
|---|---|
| Ovulation | Day 14 |
| Implantation | Days 20-23 |
| hCG detectable in serum | Days 23-25 (8-11 days post-conception) |
| hCG detectable in urine | 1-3 days after serum |
| Test reliable (missed period) | Day 28+ |
Role of hCG in Cycle
- Prevents luteolysis (corpus luteum degeneration)
- Maintains progesterone production → endometrium preserved → no menstruation
Types of Tests
| Test | Specimen | Threshold | Use |
|---|---|---|---|
| Qualitative (dipstick) | Urine / blood | ~25 IU/L | Home / POC |
| Qualitative (lab) | Serum | ~25 IU/L | Lab only |
| Quantitative | Serum | ~5 IU/L | Dating, ectopic, viability |
Best Time to Test
- Day of missed period - ~50% sensitive
- 1 week after missed period - most reliable
- Use first-morning urine (concentrated = more hCG)
hCG Doubling Rule
- Doubles every ~2.5 days in first 4 weeks (viable IUP)
- Fails to rise 66% in 48h → likely nonviable / ectopic
- Peak: 100,000-200,000 mIU/mL at 10-14 weeks
False Results
| False Positive | False Negative |
|---|---|
| Heterophile antibodies | Testing too early |
| Molar pregnancy / choriocarcinoma | Dilute urine |
| Delayed test reading | Hook effect (very high hCG) |
Key point: Pregnancy test turns positive around the missed period because hCG rises geometrically after implantation (~Day 20-23) and crosses the detection threshold (~25 IU/L) by Day 28.
Endocrine visual pathways short notes
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Visual Pathways - Short Notes (Endocrine Focus)
The Visual Pathway - Anatomy
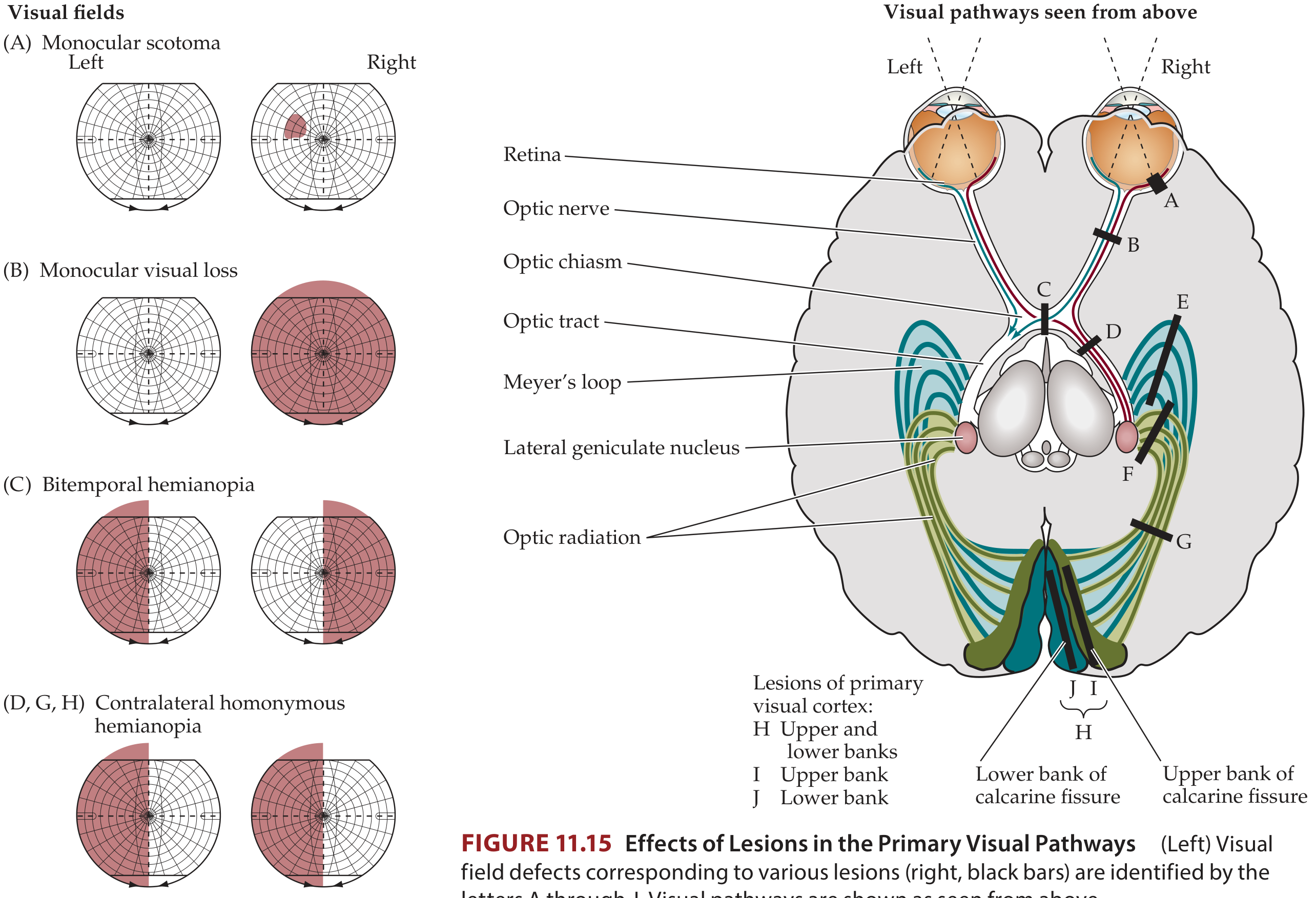
Route: Retina → Optic nerve → Optic chiasm → Optic tract → Lateral Geniculate Nucleus (LGN) → Optic radiations → Primary visual cortex (occipital lobe)
Key decussation at the chiasm:
- Nasal retinal fibers (temporal visual field) → cross to contralateral optic tract
- Temporal retinal fibers (nasal visual field) → stay ipsilateral

Endocrine Relevance - The Optic Chiasm & Pituitary
The optic chiasm sits directly above the pituitary gland (sella turcica). This is why pituitary and hypothalamic lesions classically cause visual field defects.
Lesion Map & Visual Field Defects
| Site of Lesion | Visual Field Defect | Common Endocrine Cause |
|---|---|---|
| Optic nerve | Monocular blindness / scotoma (one eye only) | Optic glioma, meningioma |
| Optic chiasm (central) | Bitemporal hemianopia (both outer fields lost) | Pituitary adenoma, craniopharyngioma, meningioma |
| Anterior chiasm | Junctional scotoma (optic neuropathy in 1 eye + superior-temporal cut in other) | Tuberculum sellae meningioma |
| Optic tract | Contralateral homonymous hemianopia (incongruous) | Tumors, infarct |
| Meyer's loop (temporal optic radiation) | Superior quadrantic homonymous hemianopia ("pie in the sky") | Temporal lobe lesions |
| Parietal optic radiation | Inferior quadrantic homonymous hemianopia | Parietal lobe lesions |
| Visual cortex (occipital) | Dense congruous homonymous hemianopia ± macular sparing | Posterior cerebral artery occlusion |
| Both occipital lobes | Cortical blindness | Bilateral PCA occlusion |
The Key Endocrine-Visual Connection: Pituitary Adenoma
- Pituitary adenoma grows upward out of the sella turcica
- Compresses the crossing nasal fibers at the chiasm
- Results: Bitemporal hemianopia (both temporal fields lost)
- Often insidious - patient may not notice until late
- Always test each eye separately to detect it
Crossed fibers are more vulnerable to compression than uncrossed fibers - explains why temporal fields go first. - Harrison's Principles of Internal Medicine, 22e
Quick Memory Rule
| Pre-chiasmal lesion | Monocular defect (one eye) |
|---|---|
| Chiasmal lesion | Bitemporal (heteronymous) hemianopia |
| Post-chiasmal lesion | Homonymous hemianopia (same side both eyes) |
| More posterior → more congruous the defect |
Endocrine Causes of Chiasmal Compression
- Pituitary adenoma (most common)
- Craniopharyngioma
- Hypothalamic glioma
- Meningioma (tuberculum sellae / diaphragma sellae)
- Rathke's cleft cyst
- Aneurysm (internal carotid / anterior communicating artery)
- Neuroanatomy through Clinical Cases 3rd Edition; Harrison's Principles of Internal Medicine 22e; Gray's Anatomy for Students
Visual pathway endocrine esay words
Visual Pathway & Endocrine - Easy Words
What is the Visual Pathway?
Think of it like a road that carries "what you see" from your eyes to your brain.
The Road: Step by Step
Eyes (Retina)
↓
Optic Nerve (like a cable from each eye)
↓
Optic Chiasm (X-shaped crossing point)
↓
Optic Tract (road to brain)
↓
LGN - Lateral Geniculate Nucleus (relay station in thalamus)
↓
Optic Radiations (fan of fibres)
↓
Visual Cortex - Occipital lobe (back of brain = "seeing centre")
The Most Important Part - The Optic Chiasm
- The chiasm is shaped like the letter X
- Here, inner half fibres cross over to the opposite side
- Outer half fibres stay on the same side
- The chiasm sits just above the pituitary gland
This is why pituitary problems affect vision!
The Endocrine Connection (Most Important for Exams)
Pituitary Adenoma (most common cause)
- The pituitary gland sits in a bony cup called the sella turcica
- When a pituitary tumour grows upward, it squeezes the chiasm from below
- It hits the crossing fibres first (the inner fibres that carry outer field vision)
- Result: You lose both outer (temporal) visual fields
- This is called Bitemporal Hemianopia
Normal vision: You see left + right + centre
Bitemporal hemianopia: You see only the centre
(like wearing blinkers / horse blinders)
Lesion Table in Simple Words
| Where is the problem? | What vision is lost? | Easy way to remember |
|---|---|---|
| One optic nerve | One eye goes blind | "Cable cut on one side" |
| Optic chiasm | Outer fields of BOTH eyes | "Pituitary pressing from below" |
| After the chiasm (optic tract) | Same-side field in BOTH eyes | "Right side damage = left field gone in both eyes" |
| Temporal lobe radiation | Upper quarter of opposite field | "Pie in the sky" |
| Parietal lobe radiation | Lower quarter of opposite field | "Pie on the floor" |
| Back of brain (cortex) | Half field gone, but centre often saved | "Macular sparing" |
| Both sides of cortex | Complete blindness | Cortical blindness |
Key Endocrine Causes of Chiasm Compression
- Pituitary adenoma - grows upward from below
- Craniopharyngioma - grows near pituitary in children
- Meningioma - tumour of brain covering near sella
- Hypothalamic glioma - grows downward
- Aneurysm - balloon in a nearby artery
The Golden Rule
| Before chiasm | One eye affected |
|---|---|
| At chiasm | Both outer fields lost (bitemporal) |
| After chiasm | Same field in both eyes lost (homonymous) |
| More towards back of brain → defect becomes more equal/matching in both eyes |
One-Line Summary
The pituitary tumour grows up, squeezes the optic chiasm, destroys the crossing fibres, and causes bitemporal hemianopia - the patient loses both outer fields of vision.
This is a shared conversation. Sign in to Orris to start your own chat.