[08/05, 1:15 am] SHAIK ASHFAQ BASHA: Hello to alll Anatomy important questions Uterus - clinical corollation and clinical cases in vishwam singh Ischio rectal fossa Ovarian fossa [08/05, 1:15 am] SHAIK ASHFAQ BASHA: Study uterus Hbc clinicals on prostate and uterus Perineal pouches body Ischiorectal fossa and today's hema ovary notes
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Here's your complete anatomy notes covering all the important topics:
🫀 ANATOMY IMPORTANT QUESTIONS — COMPLETE NOTES
1. UTERUS — Anatomy, Clinical Correlations & Cases
(Gray's Anatomy for Students + Robbins Pathology)
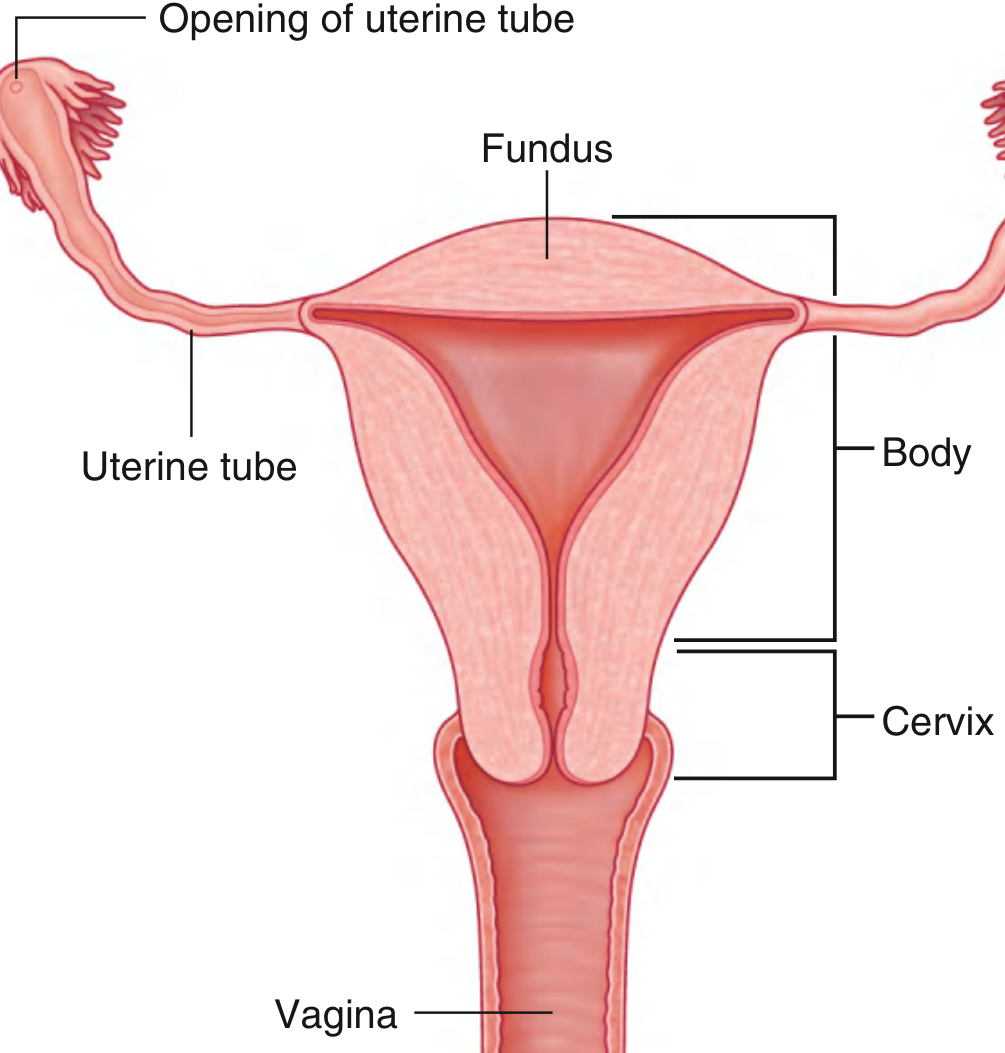
Structure
- Thick-walled muscular organ in the midline, between bladder (anterior) and rectum (posterior)
- Parts: Fundus (above uterine tubes), Body, Cervix, and it joins the Vagina inferiorly
- The cavity of the body = narrow slit laterally; inverted triangle shape anteriorly
- Superior corners → continuous with uterine tube lumina; inferior corner → continuous with cervical canal
- During pregnancy, the uterus expands dramatically superiorly into the abdominal cavity
Ligaments (Supports of Uterus)
| Ligament | Attachment | Importance |
|---|---|---|
| Transverse cervical (Cardinal) | Cervix & vaginal vault → lateral pelvic wall | MOST IMPORTANT support |
| Pubocervical | Cervix → anterior pelvic wall | |
| Uterosacral | Cervix → posterior pelvic wall | |
| Broad ligament | Peritoneal fold enclosing uterus, tubes, ovaries |
- Also supported by: perineal membrane, levator ani, perineal body
Cervix & Vaginal Fornices
- The cervix is a dome-shaped structure visible on speculum examination
- Vaginal fornices surround it (anterior, posterior, lateral)
- Posterior fornix is closely related to the recto-uterine pouch (Pouch of Douglas)
⚕️ Clinical Correlations & Cases
1. Hysterectomy
- Surgical removal of uterus (body + fundus + cervix ± ovaries & tubes)
- Full: Total Abdominal Hysterectomy + Bilateral Salpingo-Oophorectomy (TAH + BSO)
- Indications: uterine/cervical/ovarian cancer, endometriosis, excessive bleeding, postpartum hemorrhage
- Done via transverse suprapubic incision
- ⚠️ Key danger: The ureter runs close to the uterine artery — "water under the bridge" — risk of ureteric injury during ligation of uterine arteries
2. Recto-Uterine Pouch (Pouch of Douglas)
- Lies between rectum and uterus — lowest part of the abdominopelvic cavity in supine position
- Site of collection of pus, blood, or peritoneal fluid
- Cannot be palpated transabdominally — examined by transvaginal or transrectal digital palpation
- If abscess → drained via posterior vaginal wall (culdocentesis / posterior colpotomy)
3. Uterine Prolapse
- Weakness of cardinal (transverse cervical) ligaments + pelvic diaphragm → uterus descends
- Classified as 1st, 2nd, 3rd degree (procidentia = complete prolapse)
4. Implantation abnormalities
- Normal implantation = body of uterus
- Ectopic pregnancy = implantation in uterine tube (ampulla most common) → risk of rupture → hemoperitoneum collecting in Pouch of Douglas
2. ISCHIO-ANAL (ISCHIO-RECTAL) FOSSA
(Gray's Anatomy for Students)
Shape & Location
- Inverted wedge-shaped gutters on either side of the anal aperture, in the anal triangle
- Walls:
- Lateral wall: ischium + obturator internus muscle + sacrotuberous ligament
- Medial wall: levator ani muscle
- Medial & lateral walls converge superiorly where levator ani attaches to fascia of obturator internus
Contents
- Fat (fills the fossa — allows movement of pelvic diaphragm and expansion of anal canal during defecation)
- Pudendal nerve + internal pudendal vessels — pass through the pudendal canal (Alcock's canal) in the lateral wall
- Inferior rectal nerves and vessels cross the fossa to reach external anal sphincter
Anterior Recesses
- The ischio-anal fossae extend anteriorly as recesses into the urogenital triangle, superior to the deep perineal pouch
- These recesses = three-sided pyramid shape, apex pointing anteriorly toward pubis
⚕️ Clinical Correlation — Ischio-anal Abscess
- Anal mucosa can be torn by hard feces → infection of anal sinuses/crypts
- Infection can spread:
- Between sphincters → intersphincteric fistula
- Superiorly → pelvic cavity
- Laterally → ischio-anal fossa abscess (most common perianal abscess)
- The fat-filled fossa is a good medium for bacterial proliferation → painful perianal swelling
- If untreated → horseshoe abscess (crosses midline via posterior communication)
- Treatment: Surgical drainage
3. OVARIAN FOSSA
(Color Atlas of Human Anatomy Vol 2 + Campbell Walsh Urology)
Definition
- A depression of the peritoneum on the lateral wall of the pelvis
Boundaries
| Boundary | Structure |
|---|---|
| Anterior | External iliac artery |
| Posterior | Internal iliac artery (and ureter) |
| Floor | Obturator vessels + obturator nerve (beneath peritoneum) |
| Posterior boundary | External iliac vessels |
Position of Ovary
- In a nulliparous adult woman: ovary lies in the ovarian fossa
- In multiparous women: ovary is usually somewhat lower
- The ureter is closely related — separated from ovary only by parietal peritoneum
Support of Ovary
- Mesovarium — peritoneal fold anchoring it to the posterior broad ligament
- Suspensory ligament of ovary (infundibulopelvic ligament) — contains ovarian vessels, attaches to superior pole
- Ligament of ovary — from inferior pole to tubal angle of uterus
⚕️ Clinical Note
- Ovarian cancer (80–90% of ovarian tumors) arises from the epithelial surface of the ovary
- The ovary is NOT covered by peritoneum (covered by germinal epithelium = modified peritoneum) — explains peritoneal spread
- Because of proximity of ureter to the ovarian fossa, ureteric injury is a risk during oophorectomy
4. PERINEAL POUCHES & PERINEAL BODY
(Gray's Anatomy for Students)
Perineal Membrane
- Thick fibrous sheet filling the urogenital triangle
- Has a free posterior border anchored in midline to the perineal body
- Attached laterally to pubic arch
- Functions: supports external genitalia + pelvic viscera (below the urogenital hiatus)
Deep Perineal Pouch
- Immediately superior to the perineal membrane
- Contains:
- External urethral sphincter (skeletal muscle)
- Deep transverse perineal muscle
- Neurovascular tissues
- In women: urethra AND vagina pass through the deep perineal pouch and perineal membrane
Superficial Perineal Pouch
- Inferior to the perineal membrane
- Contains:
- Erectile structures: crura of clitoris/penis (attached to pubic arch), bulbs of vestibule (women) / corpus spongiosum (men)
- Skeletal muscles: ischiocavernosus, bulbospongiosus, superficial transverse perineal
- In women: bulbs of vestibule flank the vaginal opening; glans clitoris at midline anteriorly
Perineal Body
- A fibromuscular node in the midline, at the junction of the urogenital and anal triangles
- Convergence point for multiple muscles:
- External anal sphincter
- Bulbospongiosus
- Superficial and deep transverse perinei
- Levator ani (pubovaginalis)
- Clinical importance: Torn during difficult childbirth → episiotomy to prevent uncontrolled tear
5. PROSTATE — Pathology & HBC Clinicals
(Robbins & Kumar Basic Pathology)
Zones of Prostate
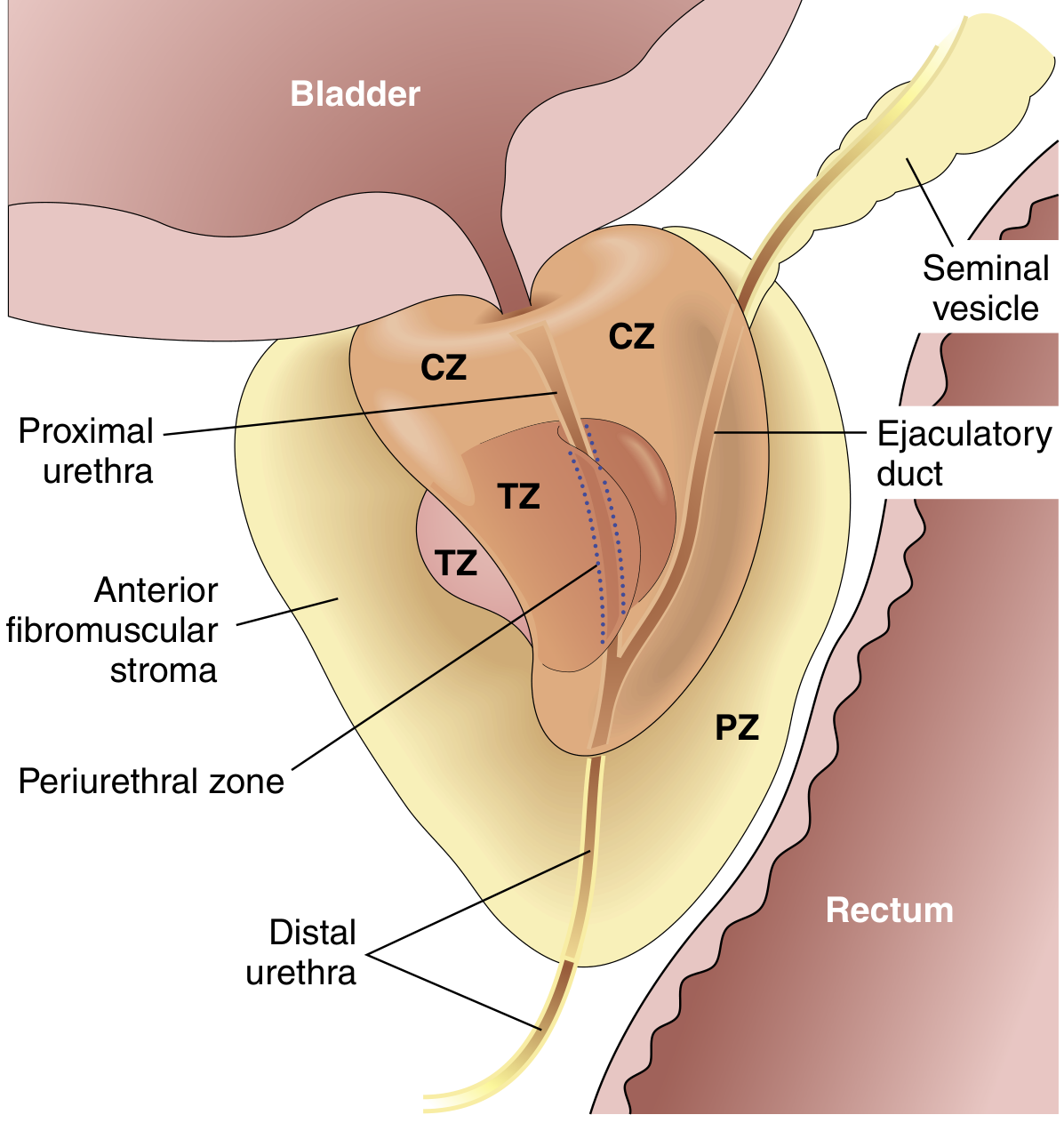
| Zone | Pathology |
|---|---|
| Transition zone (inner) | BPH (Benign Prostatic Hyperplasia) |
| Peripheral zone (outer) | Carcinoma (70–80%) — palpable on DRE |
| Central zone | Less commonly involved |
Normal prostate: two cell layers — flat basal cell layer + overlying columnar secretory cell layer
A. Prostatitis
| Type | Key Features |
|---|---|
| Acute bacterial | Fever, chills, dysuria, perineal pain, bladder outlet obstruction; ⚠️ DRE contraindicated (risk of bacteremia); Dx by urine culture |
| Chronic bacterial | Recurrent UTIs; low back pain, dysuria; leukocytosis in prostatic secretions + positive culture |
| Chronic abacterial (Pelvic Pain Syndrome) | Most common; >10 WBC/HPF in secretions but culture negative; diagnosis of exclusion |
| Granulomatous prostatitis | Most common cause in USA = BCG instillation for bladder cancer |
B. Benign Prostatic Hyperplasia (BPH)
- Most common benign prostatic disease in men >50 years; rises to 90% by 8th decade
- Zone: Transition zone (inner glands) → compresses urethra to slit-like orifice
- Pathogenesis: DHT (from testosterone via 5α-reductase type 2) drives stromal + glandular proliferation
- DHT is 10× more potent than testosterone
- Estrogen (levels relatively ↑ with age) acts synergistically
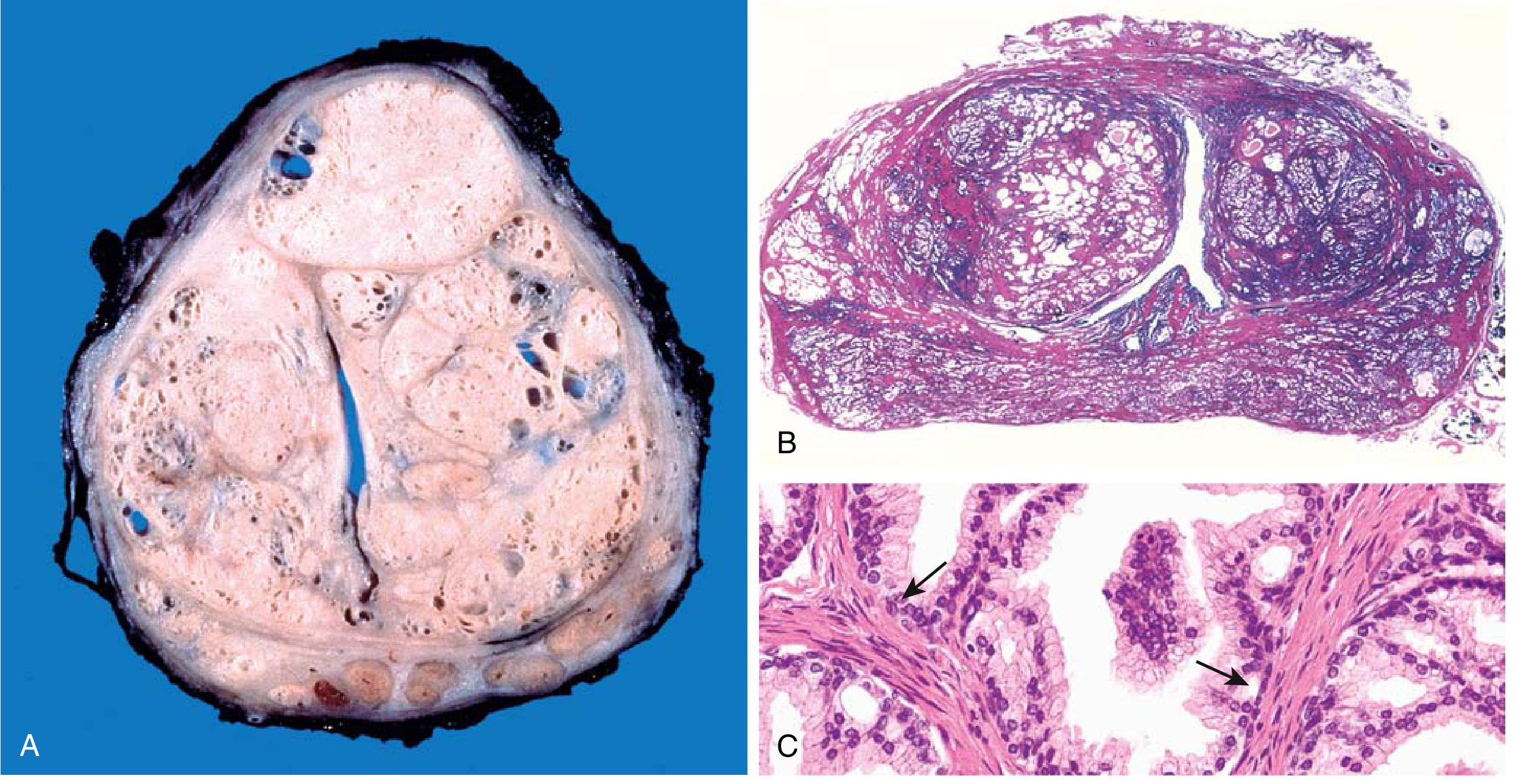
Morphology:
- Prostate weight: 60–100 g (normal ~20 g)
- Microscopy: hyperplastic glands lined by tall columnar epithelium + peripheral basal cell layer (key: basal cells PRESENT — distinguishes from carcinoma)
- Corpora amylacea = laminated proteinaceous material in lumina
Clinical Features:
- Urinary frequency, nocturia, difficulty starting/stopping stream, overflow dribbling, dysuria
- Residual urine → bacterial infections (cystitis, pyelonephritis)
- Can → hydronephrosis if complete obstruction
Treatment:
| Medical | Surgical |
|---|---|
| α1-blockers (relax smooth muscle) | TURP (Transurethral Resection of Prostate) |
| 5α-reductase inhibitors (↓ DHT) | HIFU, laser, electrovaporization, RF ablation |
C. Carcinoma of the Prostate
- Most common cancer in men — 21% of male cancer cases; 2nd leading cause of cancer death in men
- Largely a disease of aging: 20% in 50s → ~70% in 70–80 years (autopsy studies)
- Zone: Peripheral zone → palpable on Digital Rectal Examination (DRE)
- African American men have >2× the death rate (partly due to unequal access to screening)
Pathogenesis:
- Androgens, heredity, environmental factors, acquired somatic mutations
Key Histology:
- Malignant glands lack basal cell layer (vs BPH — basal cells present)
- Gleason grading system (grades 1–5; sum = Gleason score)
Screening: PSA (Prostate Specific Antigen) — elevated in cancer, BPH, and prostatitis
Clinical HBC Scenarios:
- Old man + nocturia + weak stream + elevated PSA → BPH vs Prostate Ca → need TRUS-guided biopsy
- DRE: BPH = smooth, rubbery enlargement; Carcinoma = hard, irregular, nodular
- Acute bacterial prostatitis: Never do DRE → order urine culture instead
- Bone pain in elderly man + elevated PSA → osteoblastic metastases to spine (prostate ca → blastic lesions)
Quick Memory Tricks
| Topic | Mnemonic |
|---|---|
| Uterine supports | "PCUT" — Pubocervical, Cardinal, Uterosacral, Transverse (cardinal = most important) |
| Prostate zones | "BPH is Central (transition), Cancer is Peripheral" |
| Ischio-anal fossa abscess | "Fat + Fistula + Fossa" |
| Ovarian fossa floor | Obturator nerve & vessels |
| DRE contraindicated | Acute bacterial prostatitis (→ bacteremia risk) |
Sources: Gray's Anatomy for Students; Robbins & Kumar Basic Pathology; Color Atlas of Human Anatomy Vol 2 (Thieme); Campbell Walsh Urology
This is a shared conversation. Sign in to Orris to start your own chat.