
Screenshot_20260519_083503.jpg
Please let me know diagnosis and changes seen
Reading File
Finding Sources
Searching Images
right bundle branch block ECG pattern
Loading Image
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Based on the ECG image and the machine interpretation printed at the bottom of the tracing, here is a complete analysis:
ECG Interpretation
Machine-Reported Parameters (from the printout)
| Parameter | Value |
|---|---|
| Heart Rate | 77 bpm |
| P (ms) | 142 |
| QRS (ms) | 141 |
| QT/QTc (ms) | 420 / 477 |
| RV1/SV1 (mV) | 0.13 / 0.28 |
| RV5/SV1mV | 0.93 / 0.39 |
Machine Diagnoses (printed on ECG)
- Sinus Rhythm
- Long QTc (477 ms)
- Marked Right Axis Deviation (RAD)
- Complete Right Bundle Branch Block (RBBB)
The report flags: "Report needs clinician review" and "Abnormal ECG"
Key ECG Findings & Explanation
1. Sinus Rhythm
- Normal P waves preceding each QRS complex at ~77 bpm — the underlying rhythm is normal sinus.
2. Complete Right Bundle Branch Block (RBBB)
The QRS duration is 141 ms (>120 ms = complete BBB). Criteria for RBBB:
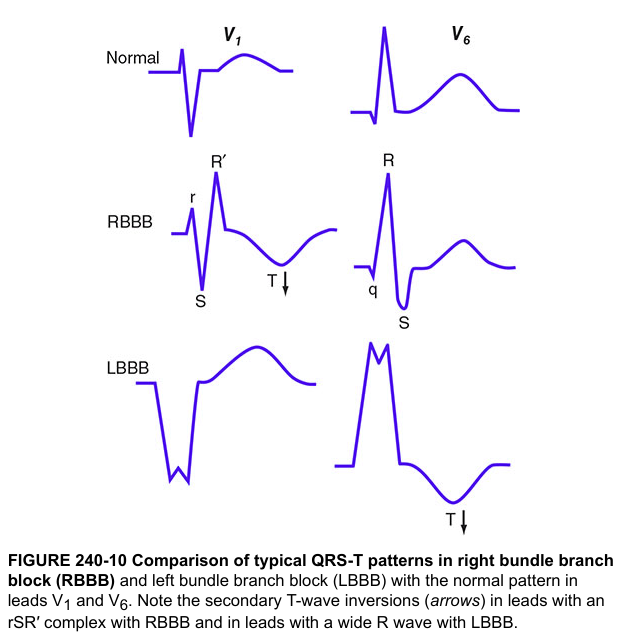
- rSR' ("rabbit ear" or M-shaped) pattern in V1–V3 — the hallmark of RBBB (visible on the tracing)
- Wide, slurred S waves in leads I, V5, V6 — representing delayed right ventricular depolarization
- Secondary T-wave inversions in V1–V3 — a normal consequence of the conduction delay, not representing ischemia
Mechanism: The right bundle branch fails to conduct, so the RV depolarizes late via cell-to-cell spread from the LV. This produces a terminal rightward and anterior vector — seen as the terminal R' in V1 and the wide S in lateral leads.
3. Marked Right Axis Deviation (RAD)
- The QRS axis is markedly rightward (machine confirms this)
- In the context of RBBB, marked RAD strongly suggests co-existing Left Posterior Fascicular Block (LPFB)
- RBBB + LPFB = Bifascicular Block — a significant finding indicating disease involving two of the three fascicles of the His-Purkinje system
- Must be distinguished from other causes of RAD: right ventricular hypertrophy, pulmonary embolism, and lateral wall MI (Goldman-Cecil Medicine)
4. Prolonged QTc (477 ms)
- Normal QTc is <440 ms (men), <460 ms (women)
- QTc of 477 ms is prolonged, raising risk of ventricular arrhythmia (Torsades de Pointes)
- In the context of RBBB and RAD, the QT measurement may be influenced by the wide QRS itself, but the machine correction still flags it as abnormal
Diagnosis Summary
Sinus rhythm with Complete Right Bundle Branch Block (RBBB) + Marked Right Axis Deviation, consistent with Bifascicular Block (RBBB + Left Posterior Fascicular Block), with prolonged QTc
Clinical Significance & Next Steps
| Finding | Clinical Implication |
|---|---|
| Complete RBBB | May be idiopathic/degenerative, but rule out: ischemic heart disease, pulmonary embolism, RV strain, infiltrative cardiomyopathy, ASD |
| Bifascicular block (RBBB + LPFB) | Risk of progression to complete (third-degree) AV block — warrants further evaluation; if symptomatic (syncope/presyncope), permanent pacemaker may be needed |
| Prolonged QTc | Check electrolytes (K⁺, Mg²⁺, Ca²⁺), review all QT-prolonging medications |
| Combined picture | Echocardiogram and stress test (echo/nuclear) are recommended; consider cardiac MRI if infiltrative disease suspected |
The machine correctly notes this ECG requires clinician review. The combination of RBBB with marked RAD (bifascicular block) in any patient with syncope, presyncope, or dyspnea should prompt urgent cardiology referral.
Sources: Goldman-Cecil Medicine; The Harriet Lane Handbook (ventricular conduction disturbances); Harrison's Principles of Internal Medicine, 21st ed.
This is a shared conversation. Sign in to Orris to start your own chat.