I have my university exam of 1 st year of subject physiology These are the important long answer give me answer of this question "Describe the synthesis of thyroid hormones. Add a note on hypothyroidism." and remeber it's a long question
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Loading Image
I now have more than enough comprehensive information from Ganong's, Guyton's, and Costanzo's physiology textbooks to write a complete long-answer exam response. Let me compose the full answer now.
Synthesis of Thyroid Hormones and Hypothyroidism
PART 1: SYNTHESIS OF THYROID HORMONES
Introduction
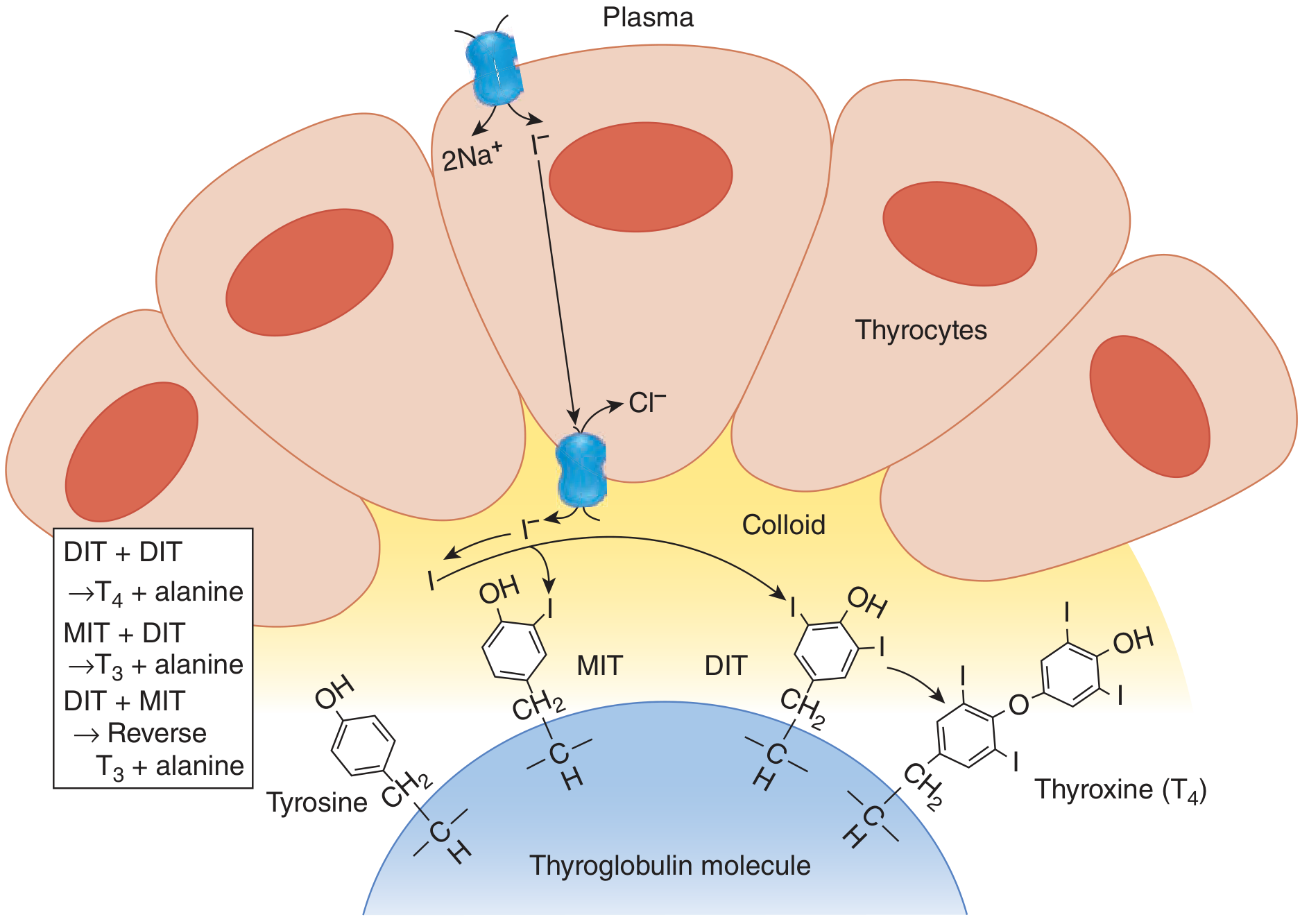
The thyroid gland is a butterfly-shaped gland located anterior to the trachea. It consists of spherical follicles, each surrounded by a single layer of epithelial cells called thyrocytes (follicular cells). The follicle is filled with colloid, which consists predominantly of the glycoprotein thyroglobulin. The thyroid hormones are thyroxine (T4) and triiodothyronine (T3), both of which are iodinated derivatives of the amino acid tyrosine.
The synthesis of thyroid hormones is a multistep process requiring iodine and occurs both inside the thyrocyte and at the apical membrane-colloid interface.
Step 1: Iodide Trapping (Iodide Uptake)
The first step in thyroid hormone synthesis is the active transport of iodide (I⁻) from the blood into the thyrocyte.
- This is accomplished by the Sodium-Iodide Symporter (NIS), located on the basolateral membrane of the thyrocyte.
- NIS co-transports 2 Na⁺ ions and 1 I⁻ ion into the cell simultaneously.
- The energy comes indirectly from the Na⁺-K⁺ ATPase pump, which maintains a low intracellular Na⁺ concentration, creating an electrochemical gradient that drives iodide uptake.
- This is an active, energy-dependent process.
- In a normal thyroid gland, the iodide concentration inside the follicular cell reaches approximately 30 times that in the plasma. During maximal stimulation by TSH, this ratio can rise to 250 times.
- This entire process is called iodide trapping.
- TSH strongly stimulates NIS activity; hypophysectomy diminishes it.
After entering the cell, iodide is transported across the apical membrane into the colloid by a chloride-iodide counter-transporter called Pendrin.
Guyton and Hall Textbook of Medical Physiology
Step 2: Synthesis and Secretion of Thyroglobulin
- The thyrocytes synthesize thyroglobulin, a large glycoprotein with a molecular weight of approximately 335,000 Da (660 kDa as a dimer).
- Each thyroglobulin molecule contains approximately 70 tyrosine residues, of which only 4-8 are normally iodinated and incorporated into thyroid hormones.
- Thyroglobulin is synthesized in the rough endoplasmic reticulum, processed in the Golgi apparatus, and secreted into the colloid by exocytosis.
Guyton and Hall Textbook of Medical Physiology
Step 3: Oxidation of Iodide and Organification
- Once iodide reaches the apical surface of the thyrocyte (colloid interface), it is oxidized to iodine (I₀ or I⁺) by the enzyme Thyroid Peroxidase (TPO), also called iodide peroxidase, in a reaction requiring H₂O₂ as a cofactor.
- This oxidized iodine is then immediately incorporated into the carbon-3 position of tyrosine residues of the thyroglobulin molecule.
- This process of incorporating iodine into tyrosine is called organification of iodide.
Ganong's Review of Medical Physiology, 26th Edition
Step 4: Formation of MIT and DIT
Iodination of tyrosine residues on thyroglobulin produces two intermediate compounds:
| Compound | Description |
|---|---|
| MIT (Monoiodotyrosine) | Tyrosine + 1 iodine atom at carbon-3 |
| DIT (Diiodotyrosine) | Tyrosine + 2 iodine atoms at carbon-3 and carbon-5 |
In the normal human thyroid, the average distribution is approximately: 3% MIT, 33% DIT, 35% T4, and 7% T3.
Step 5: Coupling Reaction (Condensation)
The MIT and DIT residues, still bound within the thyroglobulin molecule, undergo an oxidative coupling reaction, also mediated by thyroid peroxidase (TPO):
| Coupling | Product |
|---|---|
| DIT + DIT | T4 (Thyroxine / Tetraiodothyronine) + alanine |
| MIT + DIT | T3 (Triiodothyronine) + alanine |
| DIT + MIT | Reverse T3 (rT3) + alanine |
- T4 is the major product secreted (about 80 µg/day).
- T3 is the biologically more active form but secreted in smaller amounts (about 4 µg/day).
- Most T3 in the circulation (approximately 80%) is produced by peripheral deiodination of T4 in tissues such as the liver and kidney by deiodinase enzymes.
The thyroid hormones so formed remain covalently bound within the thyroglobulin molecule and are stored in the colloid. Colloid serves as a reservoir of preformed thyroid hormones - humans can subsist on an iodine-free diet for up to 2 months before circulating hormone levels fall.
Ganong's Review of Medical Physiology, 26th Edition
Step 6: Secretion of Thyroid Hormones (Reabsorption and Proteolysis)
When thyroid hormones are needed:
- Colloid is internalized by the thyrocytes via endocytosis (pinocytosis at the apical border).
- The endocytic vesicles fuse with lysosomes, forming phagolysosomes.
- Proteolytic enzymes hydrolyze the peptide bonds of thyroglobulin, releasing free T4 and T3 into the cytoplasm.
- T4 and T3 diffuse across the basolateral membrane into the capillaries and enter the circulation.
- MIT and DIT are not secreted. They are deiodinated by iodotyrosine deiodinase, and the recovered iodine is recycled within the gland. This recycled iodine provides about twice as much iodide for hormone synthesis as NIS does.
- In congenital absence of iodotyrosine deiodinase, MIT and DIT appear in urine causing iodine deficiency.
Ganong's Review of Medical Physiology, 26th Edition
Regulation of Synthesis (Hypothalamo-Pituitary-Thyroid Axis)
- TRH (Thyrotropin-Releasing Hormone) from the hypothalamus stimulates the anterior pituitary to release TSH (Thyroid-Stimulating Hormone / Thyrotropin).
- TSH acts on thyrocytes to stimulate ALL steps of thyroid hormone synthesis: iodide trapping, thyroglobulin synthesis, organification, coupling, and secretion.
- High circulating levels of free T3 and T4 exert negative feedback on both the pituitary and hypothalamus, suppressing TSH and TRH secretion.
Transport in Blood
- T4 and T3 are lipophilic and are bound to plasma proteins in circulation:
- Thyroxine-Binding Globulin (TBG) - carries ~70% of T4
- Thyroxine-Binding Prealbumin (Transthyretin)
- Albumin
- Only the free (unbound) fraction is biologically active.
- Normal total plasma T4 ≈ 8 µg/dL; total plasma T3 ≈ 0.15 µg/dL.
Ganong's Review of Medical Physiology, 26th Edition
PART 2: NOTE ON HYPOTHYROIDISM
Definition
Hypothyroidism is a clinical condition resulting from insufficient production or action of thyroid hormones (T3 and T4), leading to a generalized slowing of metabolic processes throughout the body.
Classification
| Type | Cause |
|---|---|
| Primary hypothyroidism | Defect in the thyroid gland itself |
| Secondary hypothyroidism | Deficiency of TSH (anterior pituitary failure) |
| Tertiary hypothyroidism | Deficiency of TRH (hypothalamic failure) |
Etiology (Causes)
- Autoimmune thyroid destruction - Hashimoto's Thyroiditis - most common cause in iodine-sufficient regions. Antibodies destroy thyroid tissue leading to fibrosis and failure.
- Iodine deficiency - most common cause worldwide, leads to goitre formation.
- Surgical removal of the thyroid gland (post-thyroidectomy) for hyperthyroidism or cancer.
- Radioiodine (I-131) therapy for hyperthyroidism.
- Drugs - lithium, amiodarone, antithyroid drugs (carbimazole, propylthiouracil).
- Congenital hypothyroidism - absent or hypoplastic thyroid gland; genetic enzyme defects.
- Hypothalamic or pituitary failure (secondary/tertiary).
- Target tissue resistance to thyroid hormones (rare).
Costanzo Physiology, 7th Edition
TSH Levels in Diagnosis
- Primary hypothyroidism (gland defect): TSH is elevated (increased by negative feedback due to low T3/T4).
- Secondary/Tertiary hypothyroidism (pituitary/hypothalamic defect): TSH is low or normal.
Clinical Features / Signs and Symptoms
The manifestations of hypothyroidism are the opposite of hyperthyroidism - reflecting a generalized reduction in metabolic activity.
Metabolic:
- Decreased basal metabolic rate (BMR reduced by 30-50% in myxedema)
- Weight gain without increased food intake
- Cold intolerance, decreased heat production
- Hypercholesterolaemia and hypertriglyceridaemia
Cardiovascular:
- Decreased heart rate (bradycardia)
- Decreased cardiac output
- Decreased blood volume
- Increased risk of atherosclerosis and coronary artery disease
Neuromuscular:
- Extreme muscular sluggishness and fatigue
- Slowed reflexes (hung-up reflexes - delayed relaxation phase)
- Slurred speech, slow mentation
- Mental sluggishness, lethargy, somnolence
- Sleeping 12-14 hours a day
Skin and Hair:
- Dry, coarse, scaly skin
- Hair loss (alopecia)
- Periorbital puffiness
Gastrointestinal:
- Constipation
Reproductive:
- Menstrual dysfunction (menorrhagia or amenorrhoea)
Voice:
- Deep, hoarse, froglike voice (due to myxedema of laryngeal tissues)
Myxedema
- Myxedema is the severe form of hypothyroidism in adults.
- Characterized by non-pitting edema throughout the body, especially bagginess under the eyes and facial puffiness.
- Caused by accumulation of hyaluronic acid and chondroitin sulfate bound to protein in interstitial spaces, making the fluid gel-like and immobile - hence non-pitting in nature.
- Total interstitial fluid is greatly increased.
Guyton and Hall Textbook of Medical Physiology
Goitre in Hypothyroidism
- When the defect is in the thyroid itself, low T3/T4 fails to inhibit TSH secretion.
- TSH rises continuously, chronically stimulating the thyroid gland to enlarge - producing a goitre.
- The gland enlarges but cannot produce adequate hormones (e.g., due to iodine deficiency or enzyme defects).
Hypothyroidism in Infancy and Childhood - Cretinism
- Extreme hypothyroidism during fetal life, infancy, or childhood leads to cretinism.
- Features: failure of body growth (dwarfism), intellectual disability (mental retardation), coarse facies, protruding tongue, umbilical hernia.
- Caused by: congenital absence of thyroid, genetic enzyme defects, or maternal iodine deficiency.
- A neonate without a thyroid may appear normal initially (due to maternal thyroid hormones), but symptoms appear within weeks.
- If untreated, the intellectual disability is irreversible.
- Treatment is oral T4 replacement - must be started as early as possible.
Diagnostic Tests
- Serum TSH - most sensitive test for primary hypothyroidism (elevated).
- Free T4 (fT4) - decreased.
- Free T3 (fT3) - decreased.
- BMR - reduced by 30-50% in myxedema.
- TRH stimulation test - exaggerated TSH response in primary hypothyroidism.
- Serum cholesterol - elevated.
- Anti-TPO antibodies, Anti-thyroglobulin antibodies - elevated in Hashimoto's thyroiditis.
Treatment
- Thyroid hormone replacement therapy - oral Levothyroxine (T4) is the treatment of choice.
- Exogenous T4 is converted to its active form, T3, in target tissues by deiodinases.
- T4 has a long half-life (about 7 days), so once-daily dosing maintains stable levels.
- Properly treated patients can lead normal, full lives.
Guyton and Hall Textbook of Medical Physiology; Costanzo Physiology, 7th Edition
Summary Table
| Feature | Hypothyroidism |
|---|---|
| T3/T4 levels | Decreased |
| TSH (primary) | Increased |
| TSH (secondary/tertiary) | Decreased |
| BMR | Decreased |
| Heart rate | Decreased |
| Weight | Increased |
| Temperature tolerance | Cold intolerance |
| Reflexes | Sluggish (delayed relaxation) |
| Skin | Dry, coarse, non-pitting edema |
| Special form in adults | Myxedema |
| Special form in children | Cretinism |
| Most common cause | Hashimoto's thyroiditis / iodine deficiency |
| Treatment | Levothyroxine (T4) oral |
Sources: Ganong's Review of Medical Physiology (26th Ed.), Guyton and Hall Textbook of Medical Physiology, Costanzo Physiology (7th Ed.)
What is the full form of TSH
TSH stands for Thyroid-Stimulating Hormone.
It is also called Thyrotropin. TSH is secreted by the anterior pituitary gland and its primary function is to stimulate the thyroid gland to produce and release T3 (Triiodothyronine) and T4 (Thyroxine).
This is a shared conversation. Sign in to Orris to start your own chat.