Use of calcium for osteoporosis treatment
Reading File
Finding Sources
Finding Sources
Searching PubMed
calcium supplementation osteoporosis treatment
Reading File
Reading File
Reading File
Reading Article
PMID: 40087804
Loading Image
Reading File
Loading Image
I now have comprehensive, authoritative data from multiple sources. Here is a thorough synthesis:
Calcium for Osteoporosis Treatment
Background: Why Calcium Matters
Osteoporosis is characterized by progressive bone mass loss and skeletal fragility, increasing fracture risk. At the microscopic level, the trabecular architecture is severely disrupted compared to normal bone:
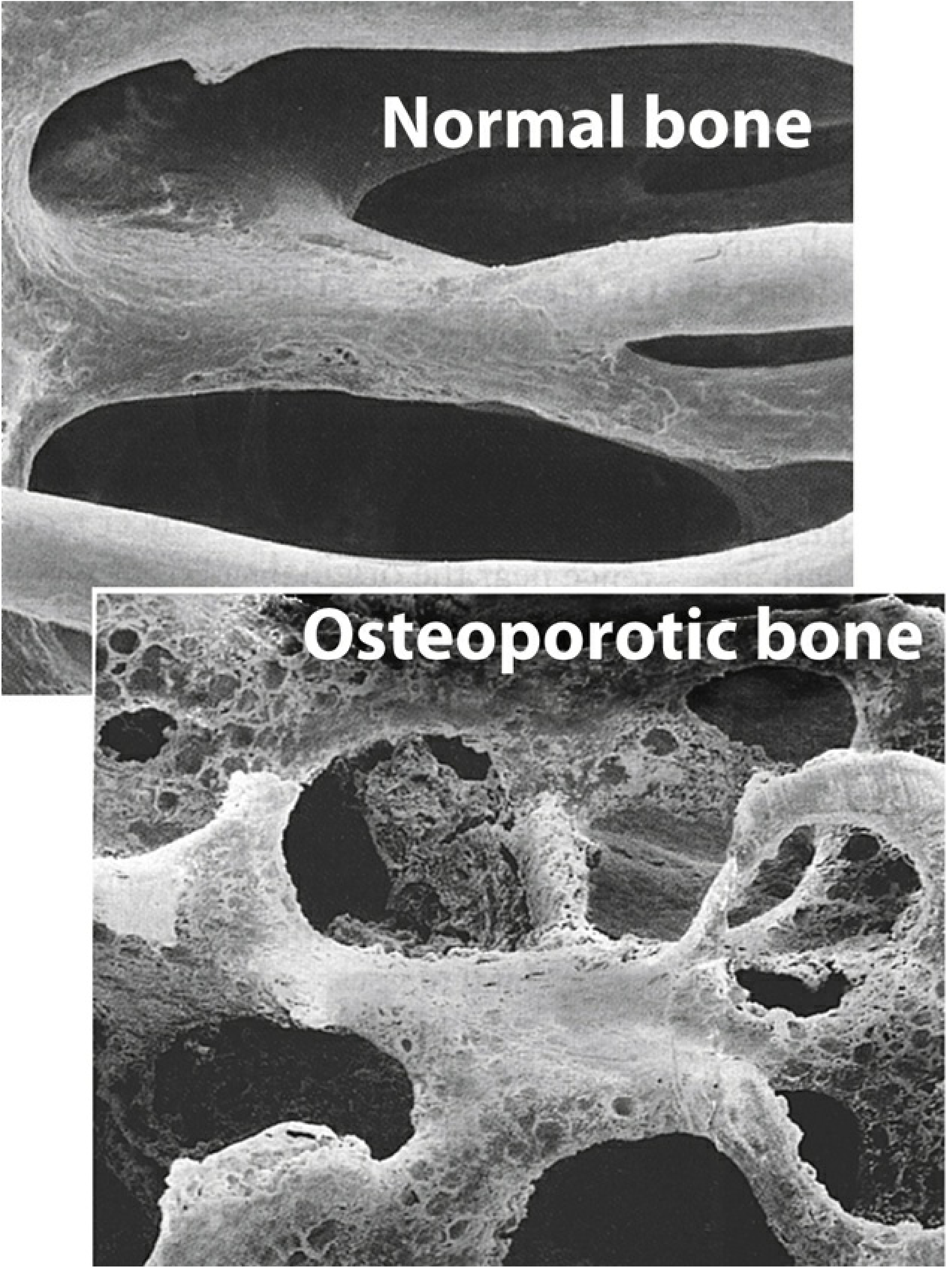
Calcium is the primary mineral constituent of bone (as hydroxyapatite crystals — calcium phosphate), making it a fundamental substrate for bone mineralization. Bone undergoes continuous remodeling, with ~10% of the skeleton replaced annually. Calcium balance directly influences whether remodeling results in net bone gain or loss.
Role of Calcium in Osteoporosis Management
1. Prevention (Foundation of Therapy)
Calcium is considered a first-line preventive measure, not a standalone curative agent. Strategies to prevent bone loss include:
- Adequate dietary calcium intake
- Vitamin D supplementation
- Weight-bearing exercise
- Smoking cessation
- Avoidance of excessive alcohol
— Lippincott Illustrated Reviews: Pharmacology
2. Calcium Supplementation — What It Does (and Doesn't Do)
| Effect | Evidence |
|---|---|
| Improves BMD | Modest increase of 1–2% |
| Reduces hip/nonvertebral fracture risk (alone) | Does NOT independently reduce fracture risk |
| Combined Ca + Vitamin D → fracture reduction | Small benefit in postmenopausal women ≥65 and men ≥65 |
| In community-dwelling adults without osteopenia/osteoporosis | No benefit in preventing fractures or falls |
"Calcium supplementation modestly improves bone mineral density by 1 to 2%, but it does not independently reduce the risk of hip and nonvertebral fractures in patients with osteoporosis." — Goldman-Cecil Medicine
Recommended Calcium Intake
- Target: 1,200–1,500 mg/day of elemental calcium (total from diet + supplements)
- Dietary sources are preferred over supplements
- Supplements used only as adjunct to achieve the daily goal
- The NOF recommends all individuals obtain at least 1,200 mg/day
— Goldman-Cecil Medicine; Swanson's Family Medicine Review
Calcium Supplement Formulations
| Supplement | Elemental Ca Content | Notes |
|---|---|---|
| Calcium carbonate | 40% | Cheapest; must be taken with meals for best absorption; poorly absorbed with PPIs/H2 blockers |
| Calcium citrate | 21% | Better tolerated; can be taken with or without food; preferred with acid-reducing agents |
— Lippincott Illustrated Reviews: Pharmacology
Vitamin D: The Essential Co-factor
Calcium supplementation alone is insufficient. Vitamin D is required for intestinal calcium absorption:
- Combined Ca (1,000 mg) + Vitamin D (400–800 IU): demonstrated small but significant reduction in hip fracture risk in postmenopausal women and men ≥65
- Target serum 25(OH)D: ≥20 ng/mL (minimum for bone health; some recommend ≥30 ng/mL)
- Activated vitamin D analogues (calcitriol, α-calcidiol) are generally avoided due to hypercalcemia risk — exception: stages 3–4 CKD with secondary hyperparathyroidism
— Goldman-Cecil Medicine; Katzung's Basic and Clinical Pharmacology
Postmenopausal osteoporosis is often accompanied by lower 1,25(OH)₂D levels and reduced intestinal calcium transport, making vitamin D co-supplementation especially important. — Katzung
Calcium's Place in the Treatment Algorithm
Calcium/vitamin D are foundational but not sufficient alone for high-risk patients. Per fracture risk stratification:
| Fracture Risk | Calcium/Vit D Role | Additional Therapy |
|---|---|---|
| Low | Primary (nonpharmacologic) | Calcium + Vitamin D + exercise |
| Moderate | Adjunct | ± Bisphosphonate |
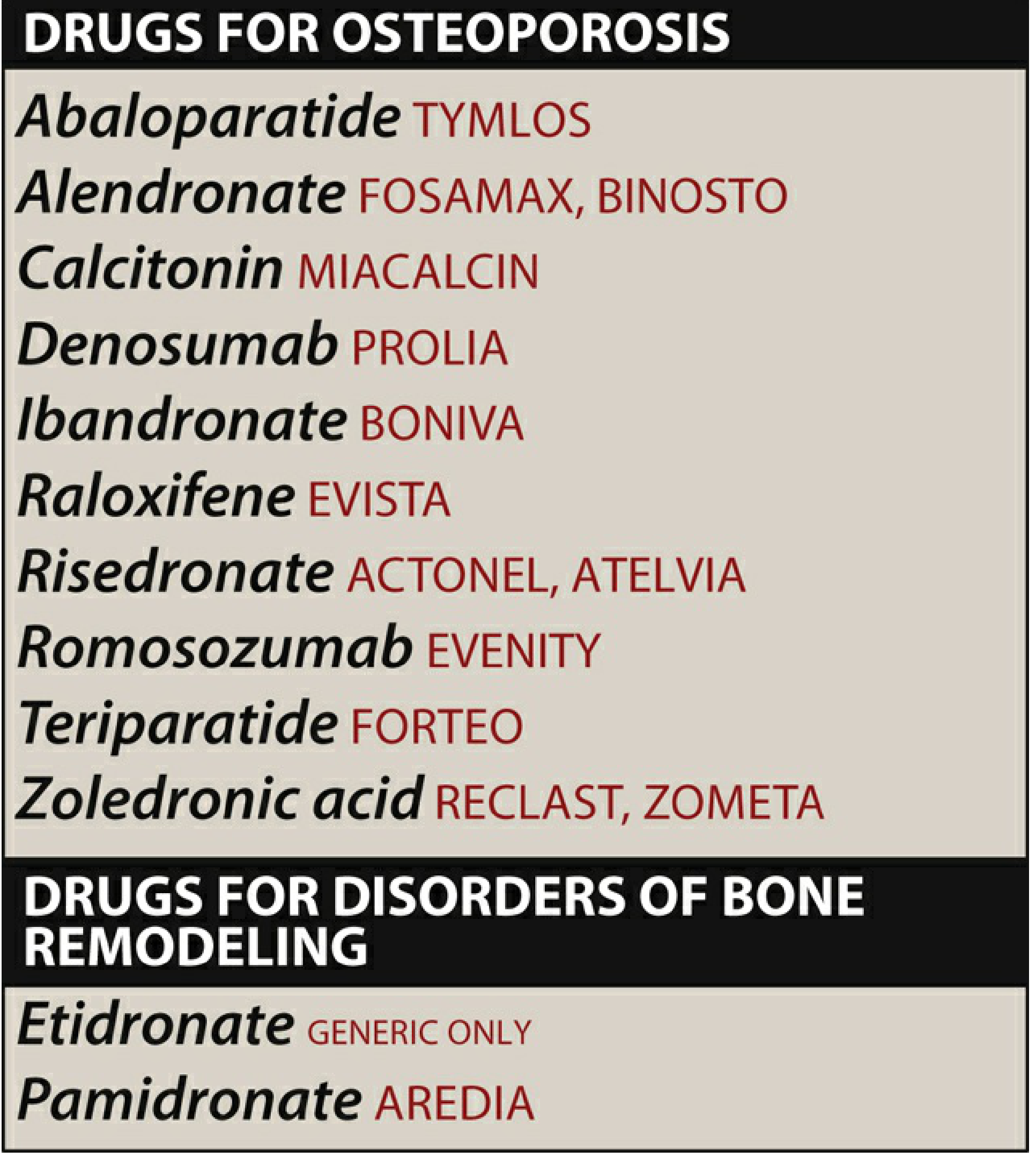
| High | Adjunct | Bisphosphonate, Denosumab, SERM |
| Very High | Adjunct | Anabolic agents (teriparatide, romosozumab) |
— Goldman-Cecil Medicine, Table 225-2
Calcium supplementation is always co-prescribed alongside pharmacologic therapy (bisphosphonates, denosumab, etc.) — it supports bone mineralization and prevents drug-induced hypocalcemia.
Adverse Effects and Drug Interactions of Calcium Supplementation
| Concern | Details |
|---|---|
| GI effects | Gas, bloating, constipation |
| Nephrolithiasis | Established increased risk with higher-dose supplementation |
| Cardiovascular events | Potential increase in nonfatal cardiac events at higher doses (controversial) |
| Drug interactions | Reduces absorption of iron, thyroid hormone, fluoroquinolones, and tetracyclines — separate by several hours |
| PPIs/H2 blockers | Impair calcium carbonate absorption → use calcium citrate instead |
— Lippincott Illustrated Reviews: Pharmacology; Goldman-Cecil Medicine
Special Populations
- Malabsorptive disorders / Bariatric surgery: calcium and vitamin D malabsorption leads to combined osteoporosis + osteomalacia; high-dose vitamin D plus calcium supplementation required
- CKD stages 3–4: activated vitamin D analogues (calcitriol) preferred; careful monitoring of serum calcium needed; denosumab (not cleared renally) may be used with vigilance
- Glucocorticoid-induced osteoporosis: calcium + vitamin D supplementation is standard adjunct along with bisphosphonates
Recent Evidence (2025 Systematic Review)
A 2025 systematic review of 37 RCTs (43,397 patients) — Migliorini et al., Eur J Med Res [PMID: 40087804] — found:
- In postmenopausal women on antiresorptive therapy, vitamin D was associated with fewer GI adverse events and lower mortality
- Calcium supplementation alone showed no statistically significant association with BMD, fracture rates, bone markers, or mortality
- This reinforces that calcium is an important adjunct, not a therapeutic anchor
Summary
Calcium is a necessary but insufficient component of osteoporosis management:
- Target: 1,200–1,500 mg/day elemental calcium, preferably from dietary sources
- Always combine with vitamin D (400–800 IU/day minimum; target 25(OH)D ≥20 ng/mL)
- Does not independently reduce fracture risk — pharmacologic therapy required for moderate-to-high-risk patients
- Choose calcium citrate over carbonate in patients on acid-suppression therapy
- Monitor for nephrolithiasis risk and potential cardiovascular effects with supplementation above dietary needs
Dietary sources of calcium, daily amounts of foods
Finding Sources
Searching the Web
dietary sources of calcium mg per serving food amounts daily intake chart
Your credits are exhausted. Your daily credits reset tomorrow, or you can purchase a top-up for more.
This is a shared conversation. Sign in to Orris to start your own chat.