Liver - anatomy, LFT, PORTAL Hypertension liver abscess, hydatid cyst
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Liver: Comprehensive Review
1. LIVER ANATOMY
Weight and Location
The adult liver weighs approximately 1.2-1.5 kg. It is located beneath the diaphragm in the right upper quadrant, protected by the lower ribs and held in place by ligamentous attachments. - Tietz Textbook of Laboratory Medicine, 7th Ed
Embryology
Liver development begins at 3-4 weeks' gestation when a hepatic foregut diverticulum buds into the ventral wall of the primitive midgut. Bipotential hepatoblasts invade the septum transversum and differentiate into hepatocytes and cholangiocytes. - Bailey & Love's Surgery, 28th Ed
Lobes and Segments
- Anatomical lobes: Right and left, divided by the falciform ligament anteriorly
- Smaller lobes: Caudate lobe (posterior-superior, drains directly into IVC - important in Budd-Chiari syndrome) and quadrate lobe (undersurface of medial left lobe)
- Riedel's lobe: An anatomic extension of the right lobe that may feel like a mobile tumour
- Couinaud segments: The liver is divided into 8 functional segments, each supplied by terminal branches of the portal vein and hepatic artery, and drained by its own bile duct and hepatic vein
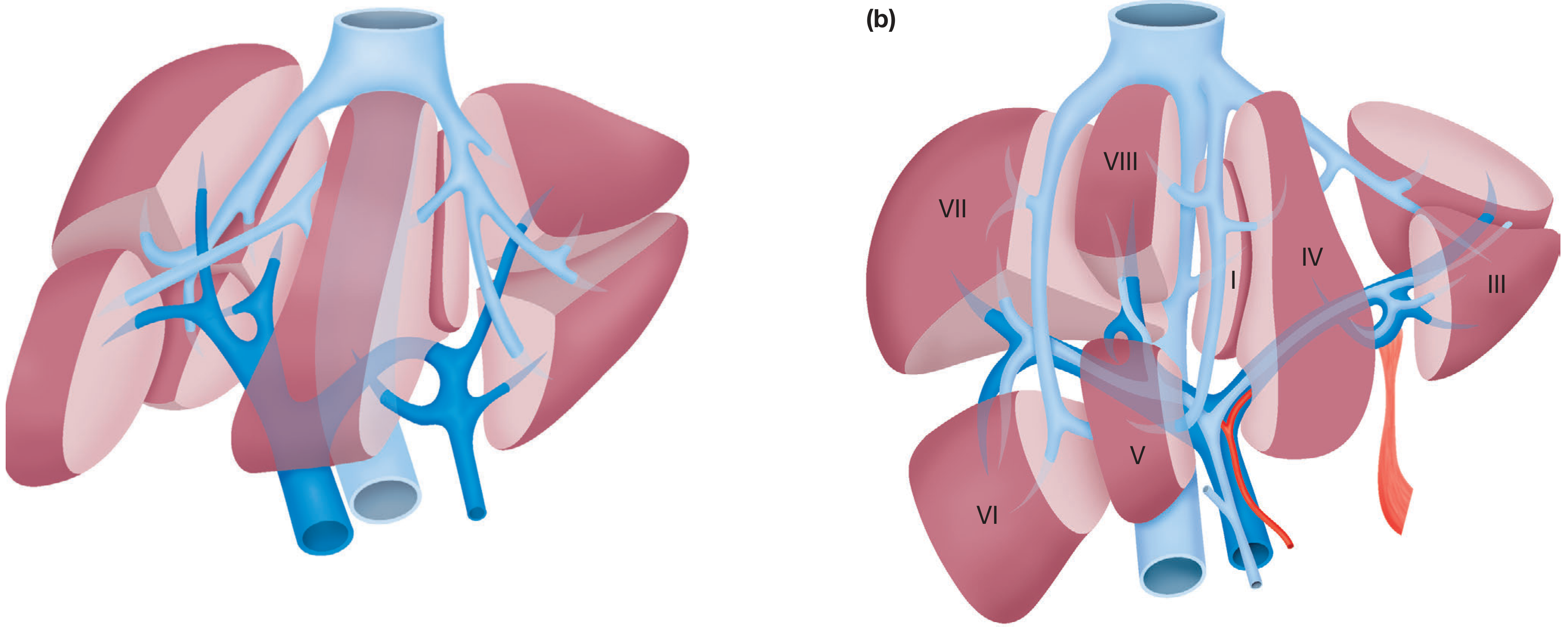
Couinaud's segmental anatomy - as seen in the patient (a) and ex vivo (b). - Bailey & Love's Surgery
Ligaments and Peritoneal Reflections
| Ligament | Origin/Note |
|---|---|
| Falciform ligament | Remnant of umbilical vein; divides right from left lobe anteriorly; portal hypertension can reopen these veins (caput medusae) |
| Left triangular ligament | Fixes left lobe to diaphragm; division exposes left IVC wall |
| Right triangular ligament | Fixes right lobe to right hemidiaphragm |
| Lesser omentum | Between stomach and liver; contains hilar structures in its right free edge |
| Glisson's capsule | Fibrous connective tissue layer under visceral peritoneum; envelops portal tracts carrying portal vein branches, hepatic artery, and bile ducts |
Blood Supply
The liver has a dual blood supply:
- Portal vein: ~80% of blood flow (70-80%), nutrient-rich blood from GI tract, spleen, pancreas, and gallbladder
- Hepatic artery (branch of coeliac trunk): ~20% of blood flow, oxygen-rich; each supplies approximately half the oxygen to the liver, making it highly resistant to infarction
- Portal vein is formed by the union of the splenic vein and superior mesenteric vein
- Venous drainage: Right and left hepatic veins exit posteriorly into the IVC near its entry into the right atrium
Biliary Drainage
Bile canaliculi → ductules → intrahepatic bile ducts → right and left hepatic ducts → common hepatic duct (exits at porta hepatis) → joined by cystic duct → common bile duct → duodenum
Nerve Supply
Vagus and phrenic nerves + sympathetic ganglia from T7-T10 spinal cord levels, running along hepatic arteries and bile ducts.
Key Functions of the Liver (Summary)
- Temperature regulation and pH balance
- Synthesis of clotting factors (I, II, V, VII, IX, X, XI)
- Glucose metabolism: glycolysis and gluconeogenesis
- Urea formation from protein catabolism
- Bilirubin formation from haem degradation
- Drug and hormone metabolism (Cytochrome P450)
- Vitamin storage: A, D, E, K, B12
- Albumin production for transport of fatty acids, steroids, waste
- Immunological function via Kupffer cells (mononuclear phagocyte system)
- Removal of gut endotoxins and foreign antigens
- Bailey & Love's Surgery, 28th Ed
2. LIVER FUNCTION TESTS (LFTs)
LFTs are a group of blood tests that help in diagnosis, assessing prognosis, and monitoring therapy of liver disease. Each test assesses a specific aspect of liver function. - Harper's Illustrated Biochemistry, 32nd Ed
Categories of LFTs
| Category | Tests | Significance |
|---|---|---|
| Parenchymal injury | ALT, AST | Hepatocellular damage |
| Biliary/cholestatic | ALP, GGT (GGTP), 5'-nucleotidase | Bile duct injury, cholestasis |
| Excretory function | Bilirubin (total, direct, indirect) | Cholestasis, hepatocellular dysfunction |
| Synthetic function | Albumin, Prothrombin time (PT/INR), coagulation factors | Liver reserve |
| Other | Ammonia, cholesterol, blood glucose | Metabolic function |
Individual Tests
1. Aminotransferases (ALT and AST)
- Activities significantly elevated days before onset of jaundice in acute viral hepatitis
- ALT is more specific for liver disease - not elevated in cardiac/skeletal muscle injury
- AST is elevated in diseases of liver, heart, lungs, kidneys, and muscle
- High ALT > AST: viral hepatitis
- AST:ALT ratio >2:1: suggests alcoholic liver disease
2. Alkaline Phosphatase (ALP)
- Elevated in obstructive jaundice and cholestatic conditions
- Also elevated in bone disease (remember: bone, liver, placenta isoforms)
3. Gamma-Glutamyl Transpeptidase (GGT)
- Elevated with bile duct injury; sensitive marker for alcohol use and cholestasis
4. Bilirubin
- Increase suggests cholestasis; obstruction of biliary tree must be excluded
- Fractionated analysis: direct (conjugated) vs indirect (unconjugated)
5. Albumin
- Reflects hepatic synthetic function; low in chronic liver disease
- Half-life ~20 days (not useful for acute liver failure)
6. Prothrombin Time (PT) / INR
- Reflects synthesis of clotting factors (II, VII, IX, X) by the liver
- Most sensitive short-term synthetic marker (factor VII has half-life ~6 hours)
- Prolonged PT = impaired synthetic function
Pattern Interpretation
| Pattern | Predominant Abnormality | Suggested Pathology |
|---|---|---|
| High ALT/AST | Parenchymal injury | Hepatitis (viral, toxic, ischaemic) |
| High ALP/GGT | Biliary enzymes | Cholestasis, cholangitis, bile duct injury |
| High bilirubin | Excretory | Biliary obstruction, haemolysis, hepatocellular |
| Low albumin + high PT | Synthetic failure | Cirrhosis, acute liver failure |
- Tietz Textbook of Laboratory Medicine, 7th Ed; Sleisenger & Fordtran's GI and Liver Disease
3. PORTAL HYPERTENSION
Definition and Normal Values
- Portal vein pressure normally = 5-7 mmHg; portal flow = 1000-1200 mL/min
- Portal hypertension = clinically significant when portal pressure gradient >10 mmHg; variceal bleeding risk increases at >12 mmHg
Classification by Site of Obstruction
| Type | Location | Key Causes |
|---|---|---|
| Pre-sinusoidal (Pre-hepatic) | Before sinusoids | Portal vein thrombosis, schistosomiasis, Felty syndrome, increased portal flow |
| Sinusoidal (Hepatic) | At sinusoids | Cirrhosis (most common cause overall), acute/chronic hepatitis, fatty liver |
| Post-sinusoidal (Post-hepatic) | After sinusoids | Budd-Chiari syndrome (hepatic vein occlusion - associated with myeloproliferative disorders in 50% of cases), congestive cardiac failure, venoocclusive disease |
Pathophysiology
Portal hypertension in cirrhosis involves two components:
- Structural (static) resistance: Progressive collagen deposition and nodule formation distort sinusoidal blood flow → increased intrahepatic resistance
- Dynamic resistance: Contraction of hepatic stellate cells (HSCs), imbalance of intrahepatic vasodilators (notably nitric oxide - deficient intrahepatic) and vasoconstrictors, injured hepatocytes
- In the splanchnic circulation paradoxically, NO is overproduced, causing splanchnic vasodilation, which increases portal blood flow and worsens portal hypertension
Portosystemic Collaterals (Sites of Varices)
When portal pressure rises, blood is diverted through collateral channels:
| Site | Clinical Significance |
|---|---|
| Gastro-oesophageal junction | Oesophageal/gastric varices (life-threatening bleeding) |
| Umbilicus | Caput medusae (reopening of umbilical veins) |
| Rectum | Anorectal varices (distinguish from haemorrhoids) |
| Retroperitoneum | Veins of Retzius |
Complications of Portal Hypertension
A. Ascites
- Results from splanchnic arterial vasodilation → effective arterial hypovolemia → activation of renin-angiotensin-aldosterone system (RAAS) + sympathetic nervous system → renal sodium and water retention
- Inflammatory mediators (PAMPs from bacterial translocation, DAMPs from injured liver) further impair circulatory function
B. Variceal Haemorrhage
- Most dangerous complication; oesophageal varices most common bleeding source
C. Hepatic Encephalopathy
- Impaired ammonia metabolism + abnormal neurotransmitters (portosystemic shunting bypasses liver)
D. Hepatorenal Syndrome
- Renal vasoconstriction secondary to splanchnic vasodilation and reduced effective circulating volume
E. Splenomegaly/Hypersplenism
- Thrombocytopenia, anaemia, leucopenia
F. Other complications: Spontaneous bacterial peritonitis (SBP), hepatopulmonary syndrome, portopulmonary hypertension, hepatic hydrothorax, dilutional hyponatraemia
- Sleisenger & Fordtran's GI and Liver Disease; Tietz Textbook of Laboratory Medicine
4. LIVER ABSCESS
Epidemiology
- Incidence: approximately 1 in 5000 hospital admissions (fairly constant rate)
- Increased risk in: elderly, diabetics, immunosuppressed
- Worldwide, bacteria remain the most common cause
Types and Causative Organisms
A. Pyogenic (Bacterial) Liver Abscess
- Usually polymicrobial; most common organisms: Klebsiella, E. coli, and the Streptococcus milleri group
- Routes of infection:
- Biliary tract pathology - most common source (35%) - cholangitis, bile duct obstruction
- Portal spread from GI tract (20%) - diverticulitis, appendicitis
- Contiguous spread from subphrenic/intra-abdominal collections
- Bacteraemia secondary to trauma
- Infected cysts, necrotic tumours post-chemotherapy
- Cryptogenic (no source identified) - 10%
B. Amoebic Liver Abscess
- Caused by Entamoeba histolytica
- Endemic in tropical/subtropical regions
- "Anchovy sauce" appearance of aspirate
- Responds well to metronidazole (medical treatment often sufficient)
Clinical Features
- Fever (most consistent finding)
- Anorexia, malaise
- Right upper quadrant discomfort/pain
- Hepatomegaly
- Occasionally jaundice
Diagnosis
- Suggested by finding of a multiloculated cystic mass on ultrasonography or CT scan
- Confirmed by aspiration (for microbiology and culture)
- CT scan shows air-fluid level and rim enhancement
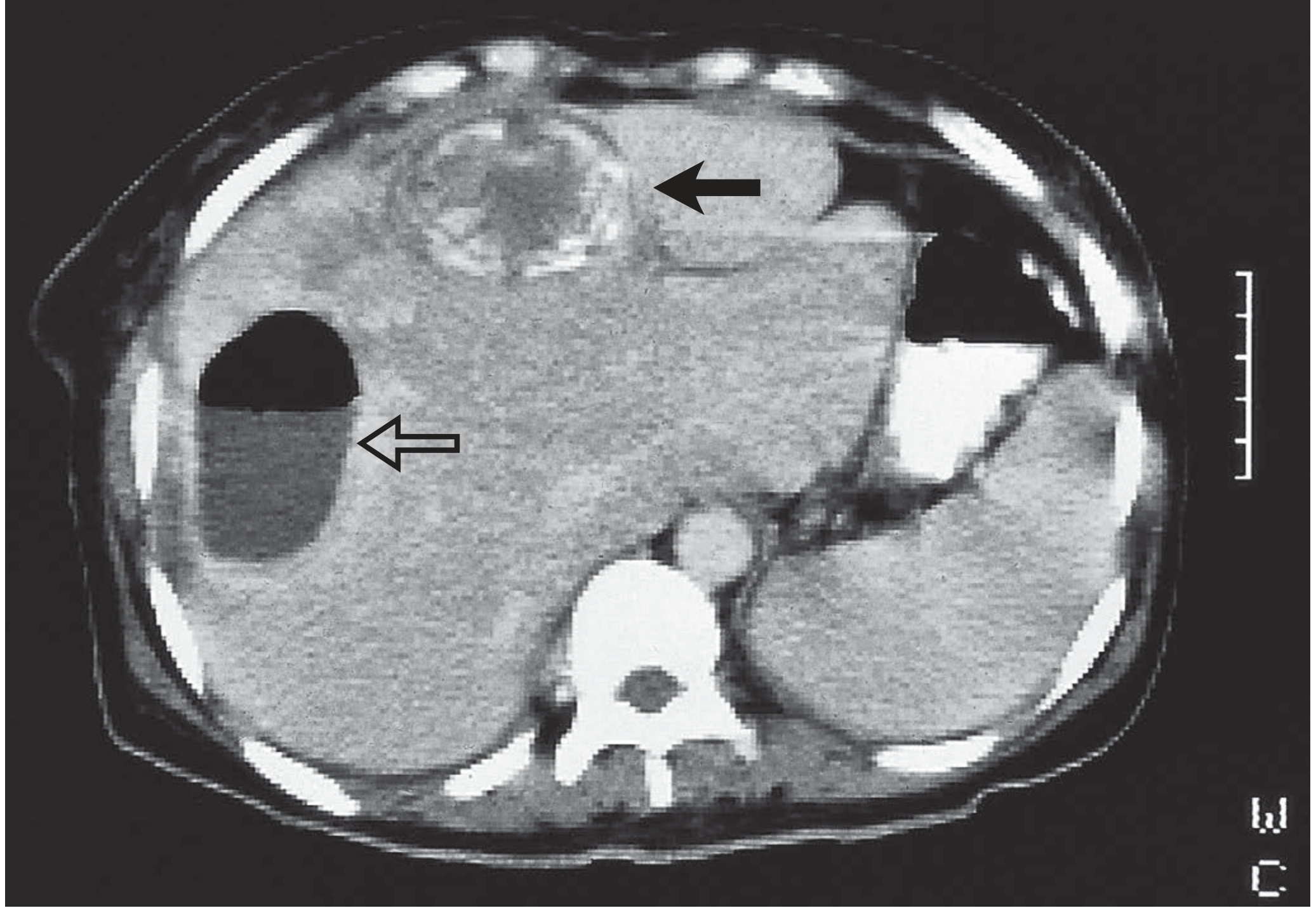
CT scan showing liver abscess with air-fluid level (open arrow) and a haemangioma for comparison (closed arrow). - Bailey & Love's Surgery
Differential Diagnosis
Simple cysts with debris, hydatid cysts, necrotic tumours, non-infected haematomas can all mimic abscesses.
Treatment
Step 1: Identify the source, aspirate for microbiology + culture
Step 2: Antibiotics - combination of two or more:
- Metronidazole and clindamycin: wide anaerobic coverage, excellent penetration into abscess cavity
- Third-generation cephalosporins and aminoglycosides: effective against Gram-negative organisms
Recurrent/Refractory Abscesses
- Occur when initial lesion was large, multiple abscesses present, or continued biliary communication
- May require surgical intervention or prolonged drainage
Prognosis
- Overall mortality has declined with improved imaging and antimicrobial therapy
- Recurrence rate: 12-38%, especially if the organism is not identified or the patient has diabetes
- Outcome increasingly dependent on underlying cause and comorbidities
- Bailey & Love's Surgery, 28th Ed; Current Surgical Therapy, 14th Ed
5. HYDATID CYST (Echinococcosis)
Aetiology / Life Cycle
- A zoonosis caused by the larval stage of Echinococcus tapeworms
- Three species: E. granulosus (most common), E. multilocularis, E. ligartus
- Definitive host: Dog (adult tapeworm attached to ileal villi; thousands of ova shed in faeces)
- Intermediate host: Sheep (usual); humans are accidental intermediate hosts - end-stage for the parasite
- No human-to-human transmission
- Endemic: Mediterranean, Middle East, Far East, South America, Australia, New Zealand, East Africa
How humans are infected: Oncospheres from ingested ova penetrate duodenal mucosa → enter bloodstream → reach liver (most commonly) or lungs → develop larval stage (hydatid cyst)
Cyst Structure
- Pericyst: Outer fibrous capsule from host tissues
- Ectocyst: Outer gelatinous membrane (from parasite)
- Endocyst: Inner germinal membrane (from parasite)
- Brood capsules: Intracystic masses producing scoleces (future worm heads)
- Hydatid sand: Free brood capsules and scoleces floating in hydatid fluid
- Daughter cysts: True replicas of the mother cyst
Epidemiology and Clinical Features
- Equal sex distribution; average age ~45 years
- ~75% in right lobe of liver; usually solitary
- Largely asymptomatic until complications occur
- Symptoms: abdominal pain, dyspepsia, vomiting
- Most frequent sign: hepatomegaly
- Jaundice and fever: each ~8% of patients
- Complications:
- Bacterial superinfection (mimics pyogenic abscess)
- Rupture into biliary tree (biliary colic, jaundice, cholangitis)
- Rupture into bronchial tree (cough, haemoptysis)
- Free rupture into peritoneum/pleura/pericardium → disseminated echinococcosis or fatal anaphylactic reaction (emergency presentation)
Diagnosis
Imaging (preferred):
- Ultrasound: Most widely used worldwide (available, affordable, accurate)
- CT scan: Best technique - space-occupying lesion with smooth outline and septa
WHO Ultrasound Classification of Hydatid Cysts (CE staging):
| Stage | Description |
|---|---|
| CL | Unilocular anechoic cyst without internal echoes or septations |
| CE 1 | Anechoic cyst with fine internal echoes ("hydatid sand") |
| CE 2 | Multivesicular with septation; honeycomb/cartwheel/rosette appearance (daughter cysts) |
| CE 3A | Detached laminated membrane (active, transitional) |
| CE 3B | Daughter cysts inside a solid matrix |
| CE 4 | No visible daughter cysts; mixed hypo/hyperechoic - "bag of wool" (inactive/degenerative) |
| CE 5 | Calcification of wall (partial or complete; does not always mean dead cyst) |
- Serology: Available but plagued by low sensitivity and specificity; used when imaging is inconclusive
- Note: Calcification is highly suggestive but does not always imply an inactive/dead cyst
CT scan showing hydatid cyst with characteristic features. - Bailey & Love's Surgery
Treatment
Medical (Albendazole):
- Active cysts should first receive a full course of albendazole before any procedure
- Also used when surgery is not possible
Interventional - PAIR (Percutaneous Aspiration, Injection, Re-aspiration):
- Aspiration → injection of scolicidal agent (povidone-iodine or hypertonic saline) → re-aspiration
Surgical Options:
- Laparoscopic marsupialisation (deroofing): Cyst aspirated → scolicidal agent injected → endocyst + daughter cysts removed → biliary communication oversewn → omentoplasty
- Pericystectomy: Complete removal with fibrous pericyst
- Hepatic segmentectomy: For deeply located or complex cysts
Key principles:
- Asymptomatic and inactive cysts (CE4, CE5) - leave alone, monitor by ultrasound
- Never aspirate without pre-treatment (risk of anaphylaxis and seeding)
- Multidisciplinary approach: hepatobiliary surgeon + physician + interventional radiologist
- Increasingly: laparoscopic approach
Pulmonary hydatid: Second most common organ affected (right lung, lower lobes); "meniscus/crescent sign" on CXR (air between pericyst and laminated membrane - sign of impending rupture); "water-lily sign" on CT (collapsed endocyst floating on residual fluid after rupture). Treatment is primarily surgical.
- Sabiston Textbook of Surgery, 22nd Ed; Bailey & Love's Surgery, 28th Ed
Quick Comparison: Liver Abscess vs Hydatid Cyst
| Feature | Pyogenic Abscess | Amoebic Abscess | Hydatid Cyst |
|---|---|---|---|
| Organism | Bacteria (Klebsiella, E. coli) | Entamoeba histolytica | Echinococcus granulosus |
| Transmission | No (endogenous/biliary/portal) | Faeco-oral | Contact with dogs/sheep |
| Fever | High fever | Moderate fever | Low/absent (unless infected) |
| Pain | Severe RUQ | Moderate RUQ | Mild/absent |
| Aspirate | Pus (culture positive) | "Anchovy sauce" | Hydatid sand/clear fluid |
| CT | Rim enhancement, air-fluid | Peripherally located, no septa | Daughter cysts, calcification, septa |
| Treatment | Antibiotics + drainage | Metronidazole (medical) | Albendazole + PAIR/surgery |
| Danger | Sepsis, bacteraemia | Pleuropulmonary spread | Anaphylaxis on rupture |
Only according to Bailey and love surgery book
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Here is a complete, structured review drawn exclusively from Bailey and Love's Short Practice of Surgery, 28th Edition.
Liver - Bailey & Love's Short Practice of Surgery (28th Ed)
1. LIVER ANATOMY
Embryology
Liver development begins at 3-4 weeks' gestation when a hepatic foregut diverticulum buds into the ventral wall of the primitive midgut. This diverticulum is the anlage for the liver, extrahepatic biliary ducts, gallbladder, and ventral pancreas. The basement membrane surrounding the liver bud is then lost and cords of bipotential hepatoblasts invade the septum transversum, differentiating into hepatocytes and cholangiocytes.
Summary Box - Liver Anatomy Key Points
- There are two anatomical lobes with a separate blood supply, bile duct and venous drainage
- There is a dual blood supply: 80% portal vein and 20% hepatic artery
- The liver regenerates to 90-100% of its previous volume following resection
- Resection is based on anatomical lines to preserve maximal functioning liver and blood supply
Ligaments and Peritoneal Reflections
The liver is covered by visceral peritoneum (serosa), with a layer of connective tissue, the Glisson capsule, underneath. At the porta hepatis, the capsule envelops and travels along the portal tracts (triads) into the liver, carrying branches of the hepatic artery, portal vein, and bile ducts.
| Ligament | Description and Surgical Significance |
|---|---|
| Falciform ligament | Remnant of the umbilical vein; runs cephalad from umbilicus, enters liver at interlobar fissure, attaches it to anterior abdominal wall. Dividing its cephalad leaves exposes the suprahepatic IVC |
| Left triangular ligament | On superior surface of left lobe; dividing it mobilises liver from diaphragm, exposing left lateral wall of IVC |
| Right triangular ligament | Fixes right lobe to undersurface of right hemidiaphragm; division allows liver to be rotated to the left |
| Lesser omentum | Between stomach and liver; contains hilar structures in its right free edge |
Blood Supply
The liver is composed of eight segments (Couinaud nomenclature), each supplied by terminal branches of the portal vein (80% of blood flow) and hepatic artery (20%), and drained by bile ducts and hepatic veins. The shape of the segments varies among individuals, but the configuration remains relatively constant.
Figure 69.1: The functional division of the liver and liver segments according to Couinaud's nomenclature. (a) As seen in the patient. (b) In the ex vivo position.
Arterial supply: Variable in origin, but in most individuals derived from the coeliac trunk (left gastric + common hepatic + splenic arteries). After supplying the gastroduodenal artery, the hepatic artery branches to produce right and left hepatic arteries, the larger right branch supplying the right lobe.
2. LIVER BLOOD TESTS (LFTs)
"The liver performs a myriad of biochemical, metabolic and immunological functions. Anhepatic humans survive for 24-48 hours. It is the only organ in the body that regenerates. Awareness of currently available liver blood tests and their significance is essential."
Main Functions of the Liver (Summary Box 69.2)
- Maintaining core body temperature
- pH balance and correction of lactic acidosis
- Synthesis of clotting factors
- Glucose metabolism, glycolysis and gluconeogenesis
- Urea formation from protein catabolism
- Bilirubin formation from haemoglobin after breakdown of effete red cells in the spleen
- Drug and hormone metabolism and excretion
- Removal of gut endotoxins and foreign antigens
- Vitamin and mineral storage: A, D, E, K and B12
- Immunological function as part of the mononuclear phagocyte system
- Albumin production for transport of fatty acids, steroids and waste products
- Angiotensin synthesis
- Cytochrome P450 detoxifies contaminants, pollutants, insecticides, food additives and alcohol
Clinical Signs of Liver Dysfunction
Symptoms vary with severity, aetiology, and acute vs chronic development. The most common include:
Jaundice, drowsiness, abdominal pain/swelling, nausea, tremors, vomiting, malaise, confusion and disorientation, bruising, peripheral oedema, and foetor hepaticus (strong musty smell to the breath).
Assessment of Chronic Liver Disease
Two key prognostic models:
1. Child-Turcotte-Pugh (CTP) Classification - originally developed to predict mortality following shunt surgery in cirrhosis; modified to predict mortality after any surgery.
2. MELD Score (Model for End-Stage Liver Disease) - devised to predict short-term prognosis following TIPSS; adopted to prioritise patients on liver transplant waiting lists. Survival probability calculated based on: INR + serum bilirubin + creatinine.
Features of Chronic Liver Disease (Summary Box 69.6)
| System | Features |
|---|---|
| General | Lethargy, fever, jaundice, protein catabolism (wasting) |
| Haematological | Coagulopathy (bruising) |
| Cardiovascular | Hyperdynamic circulation (high cardiac output, large pulse volume, low BP, flushed warm extremities) |
| Neurological | Hepatic encephalopathy |
| Portal HTN | Ascites, oesophageal varices, splenomegaly and hypersplenism |
| Cutaneous | Spider naevi, palmar erythema |
Hepatic encephalopathy grades:
- Grade 1: Inverted sleep pattern, agitation, forgetfulness, irritability, apraxia
- Grade 2: Lethargy, time and/or place disorientation, personality change, ataxia
- Grade 3: Somnolence to semistupor but responds to verbal stimuli, place disorientation, asterixis, hyperactive reflexes
- Grade 4: Coma
King's College Criteria (non-paracetamol ALF - poor prognosis indicators)
- Duration of jaundice before development of encephalopathy >7 days
- PT >50 seconds (approximate INR >3.5)
- Serum bilirubin >18 mg/dL (300 µmol/L)
Causes of Acute Liver Failure (Summary Box 69.3)
- Viral hepatitis (A, B, C, D, E)
- Drug reactions: halothane, isoniazid-rifampicin, antidepressants, NSAIDs, valproic acid
- Paracetamol overdose
- Prescription medicines: antibiotics, anticonvulsants, statins
- Mushroom poisoning
- Toxins (carbon tetrachloride)
- Shock and multiorgan failure
- Autoimmune disease
- Acute Budd-Chiari syndrome
- Metabolic: Wilson's disease
- Cancer
- Fatty liver of pregnancy
- Heat stroke; Reye's syndrome (children post-viral infection)
- SARS-CoV-2 can cause liver failure in up to 20% of patients with a severe episode
3. PORTAL HYPERTENSION
"Portal hypertension is most commonly due to liver cirrhosis, although it also occurs with extrahepatic portal vein occlusion, intrahepatic veno-occlusive disease and occlusion of the main hepatic veins (Budd-Chiari syndrome)."
Portal hypertension per se produces no symptoms and is generally diagnosed following presentation with decompensated chronic liver disease causing encephalopathy, ascites, or variceal bleeding.
Surgical involvement occurs in four situations:
- Ascites
- Oesophageal varices
- Portosystemic shunting for problems not managed by other methods
- Left-sided portal hypertension and hypersplenism
Causes of Portal Hypertension (Summary Box 69.9)
| Type | Examples |
|---|---|
| Pre-sinusoidal - Extrahepatic | Portal vein thrombosis, splenic vein thrombosis (pancreatitis, pancreatic tumour), myelofibrosis, arterioportal shunt, tropical splenomegaly |
| Pre-sinusoidal - Intrahepatic | Schistosomiasis, congenital hepatic fibrosis, portal infiltration (sarcoidosis), drugs/toxins, veno-occlusive disease |
| Sinusoidal | Cirrhosis (most common) |
| Post-sinusoidal | Budd-Chiari syndrome, veno-occlusive disease, congestive cardiac failure |
Management of Variceal Bleeding
Varices are ubiquitous in patients with portal hypertension irrespective of aetiology. The lower oesophagus is the most common site. Variceal haemorrhage is a medical emergency; failure to control bleeding with current medical management occurs in 10-20% of cases.
Resuscitation:
- Admit to ITU; large-bore peripheral cannulae; resuscitation with blood
- LFTs reveal underlying liver disease; coagulation profile identifies coagulopathy
- Hypervolaemia may increase portal pressure and exacerbate bleeding
- Vitamin K 10 mg IV; coagulopathy requires FFP + major transfusion protocol
- Thrombocytopenia secondary to hypersplenism treated if platelet count <50 × 10⁹/L
- Treatment protocols: splanchnic vasoconstrictors (terlipressin, octreotide, somatostatin) + prophylactic antibiotics
- 30% will have a non-variceal source of bleeding - confirm endoscopically once haemodynamically stable
Management of Bleeding Oesophageal Varices (Summary Box 69.10):
- Blood transfusion
- Correct coagulopathy
- Oesophageal balloon tamponade (Sengstaken-Blakemore or Minnesota tube)
- Terlipressin (drug therapy)
- Endoscopic sclerotherapy or banding
- Assess portal vein patency (Doppler USS or CT)
- TIPSS (Transjugular Intrahepatic Portosystemic Stent Shunt)
- Surgery: portosystemic shunts / splenectomy and gastric devascularisation / Sugiura procedure
Balloon Tamponade: Sengstaken-Blakemore tube (1950) or Minnesota tube (addition of an oesophageal aspiration port) - only as a 'bridge' to definitive treatment.
TIPSS: Preferred over surgical shunts as previous shunts increase complexity/morbidity of liver transplantation.
Sugiura Procedure: Combines splenectomy with oesophagogastric devascularisation. Permanently interrupts the intraoesophageal portocaval shunt while preserving perioesophageal varices. Upper half of stomach and 8-10 cm of oesophagus cleared, then oesophageal transection with stapler just above cardia.
Surgical Shunts:
- Side-to-side portocaval anastomosis
- End-to-side portocaval
- Mesocaval 'H graft'
- Splenorenal anastomosis
- Selective shunts have lower incidence of encephalopathy; no evidence prophylactic shunting is beneficial
Liver transplantation is the only therapy that treats portal hypertension AND the underlying liver disease.
Ascites Management (Summary Box 69.11 & 69.12)
Diagnosis of cause of ascites:
- Imaging (USS/CT): irregular cirrhotic liver, portal vein patency, splenomegaly
- Aspiration: culture/microscopy, protein content, cytology, amylase level
- SAAG (Serum-Ascites Albumin Gradient): High gradient (>1.1 g/dL) indicates portal hypertension
Treatment:
- Salt restriction
- Diuretics: spironolactone or frusemide (regular biochemical monitoring required)
- Abdominal paracentesis
- Peritoneovenous shunts
- TIPSS
- Liver transplantation
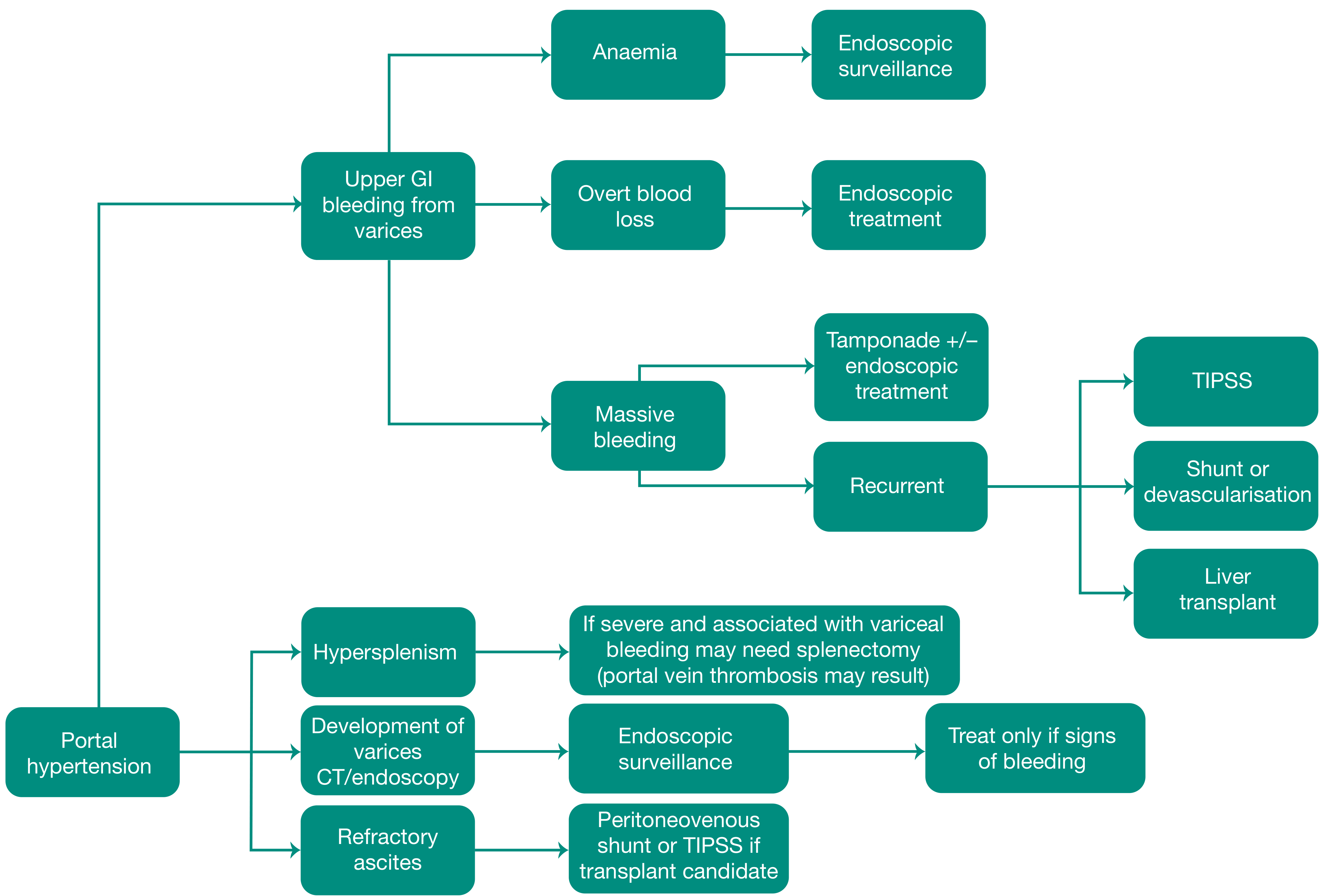
Figure 69.12: Management of complications of portal hypertension (CT, GI, TIPSS). - Bailey & Love
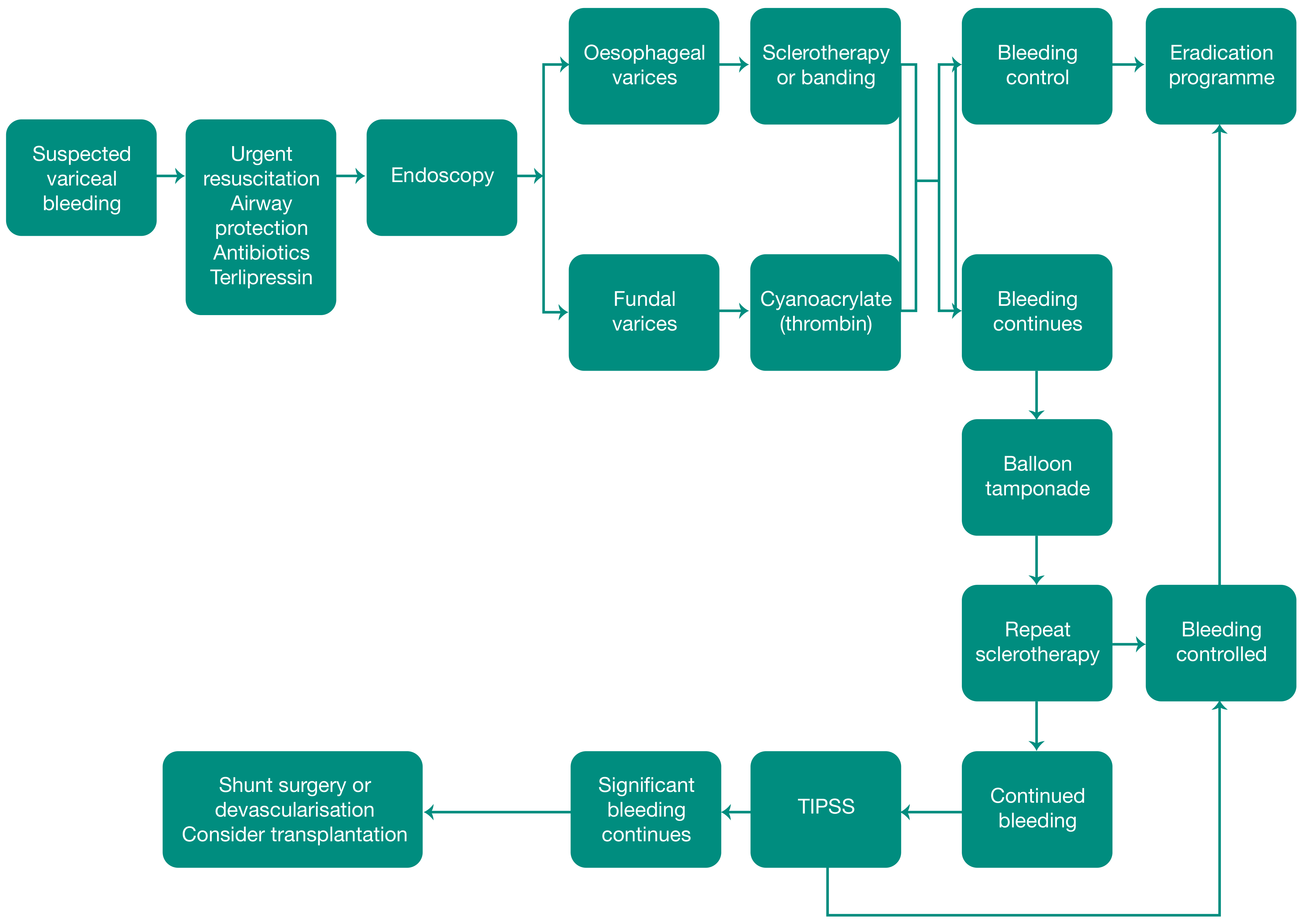
Figure 69.13: The management of variceal bleeding (TIPSS). - Bailey & Love
4. LIVER ABSCESS
Epidemiology
- Occurs at a fairly constant rate of approximately 1 in 5000 hospital admissions
- Bacterial, parasitic and fungal organisms can cause liver abscess; worldwide, bacteria remain the most common
- Infection is usually polymicrobial: Klebsiella, Escherichia coli and the Streptococcus milleri group are the usual organisms
- Increased incidence in: elderly, diabetics, and the immunosuppressed
Sources of Infection
- Biliary tract pathology - most common source (35%)
- Portal spread from GI tract (diverticulitis, appendicitis) - (20%)
- Contiguous spread from subphrenic or intra-abdominal collections
- Bacteraemia secondary to trauma
- Infected cysts and necrotic tumours following chemotherapy
- Cryptogenic (cause not identified) - 10%
Clinical Features
- Anorexia, fever, malaise
- Right upper quadrant discomfort
Diagnosis
- Suggested by finding of a multiloculated cystic mass on ultrasonography or CT scan
- Confirmed by aspiration
- CT shows air-fluid level and rim enhancement
Figure 69.18: Liver abscess - CT scan showing air-fluid level and rim enhancement (open arrow). Second lesion is a haemangioma (closed arrow). - Bailey & Love
Differential diagnosis: Simple cysts with debris, hydatid cysts, necrotic tumours, and non-infected haematomas (after unrecognised trauma) can all be mistaken for abscesses.
Treatment
Step 1: Identify the source + aspiration for microbiology and culture (repeated aspirations may be required)
Step 2: Antibiotics (combination of two or more):
- Metronidazole + clindamycin: wide anaerobic coverage, excellent penetration into the abscess cavity
- Third-generation cephalosporins + aminoglycosides: very effective against most Gram-negative organisms
Recurrent or Refractory Abscesses
- Occur when initial lesion was large, abscesses were multiple, or there is continued communication with the biliary tree
- Recurrence rate: 12-38% (depending on whether organism identified and whether patient has diabetes)
- Re-aspiration or insertion of a drain required
- If unsuccessful, laparoscopy (allows full examination of peritoneal cavity, especially when source not identified) has replaced laparotomy
Prognosis
- Overall mortality has declined because of improved imaging and effective antimicrobial therapy
- Outcome increasingly dependent on underlying cause and comorbidities
5. HYDATID CYST
Summary Box 69.13 - Infections of the Liver (Bailey & Love Key Points)
- Pyogenic liver abscesses: 1/5000 admissions
- Worldwide billions of people have parasitic infections
- Parasitic infections cause liver abscess and biliary tract damage
- Biliary tract involvement predisposes to cholangiocarcinoma
- Parasitic infections mimic pyogenic abscesses
- Obstructive jaundice from calcified flukes or biliary tract involvement
Aetiology and Life Cycle
Human echinococcosis (hydatidosis, hydatid disease) is a parasitic disease caused by the larval stages of cestodes (tapeworms) of the genus Echinococcus.
- Definitive host: Dog (adult worm in small intestine; eggs passed in faeces - highly resistant to temperature extremes, survive long periods)
- Intermediate hosts: Sheep, cattle, and humans (accidental)
- Transmission to humans: Close contact with infected dog → oral contamination by ova → entry into GI tract → development of larval stage in organs
- The liver is the organ most often affected; the lung is next most common
- E. multilocularis: variant in colder climates - spreads by actual invasion rather than expansion
Cyst Structure - Three Layers
- Outer pericyst: Derived from compressed host organ tissues
- Intermediate hyaline ectocyst: Non-infective
- Inner endocyst: The germinal membrane - contains viable parasites that can separate, forming daughter cysts
WHO Classification (WHO-IWGE, 2003) - Ultrasound Staging
Three Activity Groups:
- Group 1 (Active): Cysts larger than 2 cm, often fertile
- Group 2 (Transitional): Cysts starting to degenerate; host resistance or treatment; may still contain viable protoscolices
- Group 3 (Inactive): Degenerated, partially or totally calcified; unlikely to contain viable protoscolices
| Stage | Description |
|---|---|
| CL (cystic lesion) | Unilocular anechoic cyst without internal echoes or septations |
| CE 1 | Uniformly anechoic cyst with fine internal echoes = "hydatid sand" (protoscolices) |
| CE 2 | Cyst with internal septation - multivesicular: honeycomb / cartwheel / rosette formation (daughter cysts) |
| CE 3A (transitional) | Daughter cysts with detached laminated membrane |
| CE 3B (transitional) | Daughter cysts inside a solid matrix |
| CE 4 (inactive) | Daughter cysts no longer visible; mixed hypo/hyperechoic - "bag of wool" appearance |
| CE 5 (inactive) | Calcification of wall - partial or complete |
Clinical Features (Summary Box 6.9)
- In the UK, the usual sufferer is a sheep farmer
- While any organ may be involved, the liver is by far the most commonly affected
- Elective clinical presentation: gradually enlarging painful mass in the right upper quadrant (hepatic lesion causes dull pain from stretching of the liver capsule)
- Disease may be asymptomatic - discovered coincidentally at postmortem or on incidental imaging
- Emergency presentation: anaphylactic shock due to rupture of the hydatid cyst
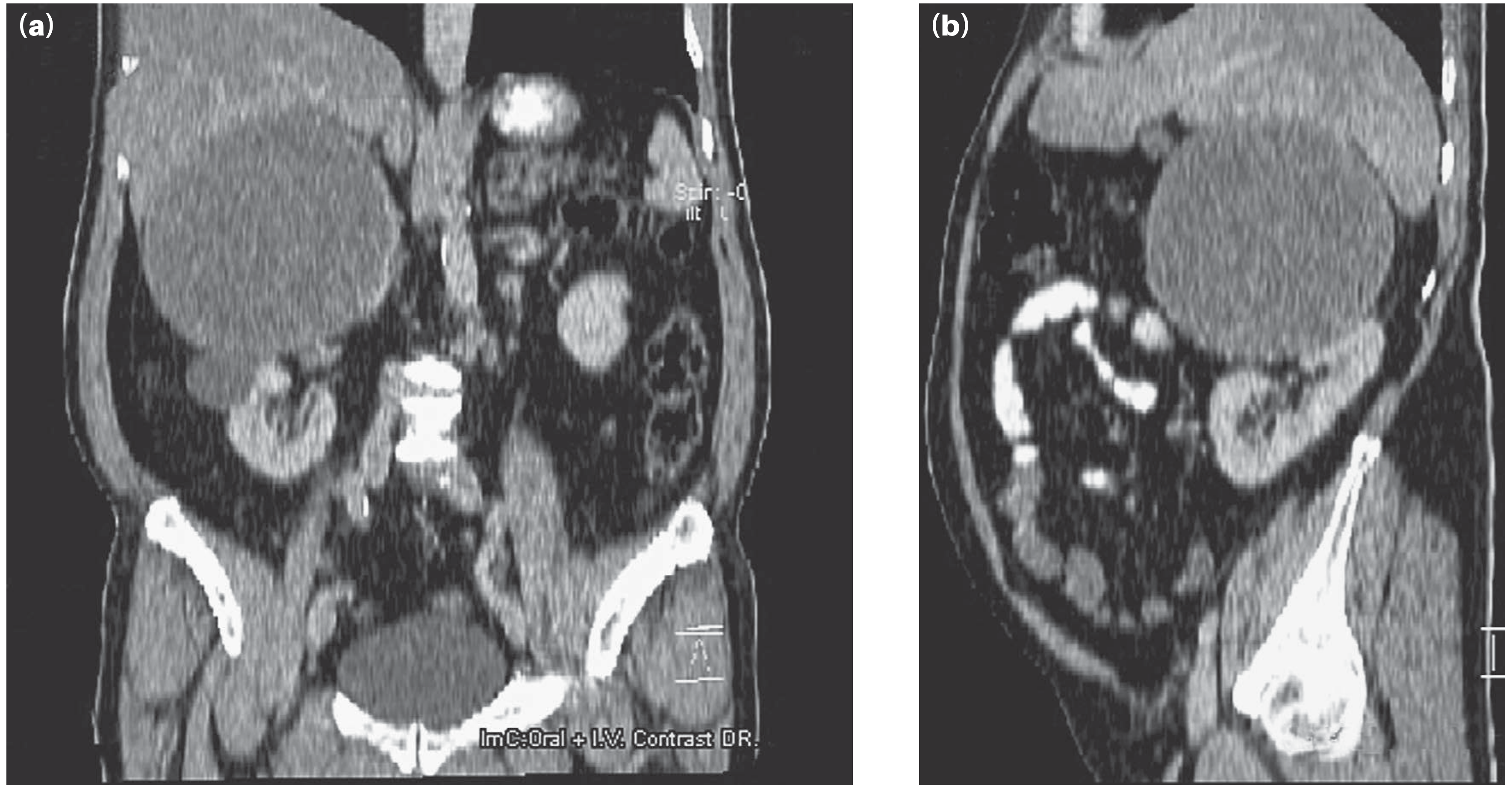
- CT scan is the best imaging technique - diagnostic feature is a space-occupying lesion with a smooth outline with septa

Figure 6.12: CT scan showing disseminated hydatid cysts of the abdomen - Bailey & Love
Treatment (Summary Box - Hydatid Cyst of the Liver)
- Ideally managed in a tertiary unit by a multidisciplinary team of hepatobiliary surgeon, physician and interventional radiologist
- Leave asymptomatic and inactive cysts (CE4, CE5) alone - monitor size by ultrasonography
- Active cysts: First treat with a full course of albendazole
- Several procedures available: PAIR, pericystectomy with omentoplasty, hepatic segmentectomy
- Increasingly, a laparoscopic approach is being tried
Surgical Approach (from Chapter 69):
- Options range from liver resection or local excision to deroofing with evacuation of contents
- Contamination of peritoneal cavity with active hydatid daughters must be avoided by:
- Continuing albendazole + adding preoperative praziquantel
- Packing peritoneal cavity with 20% hypertonic saline-soaked packs
- Instilling 20% hypertonic saline into cyst before opening
- Biliary communication must be actively sought and sutured
- Omentoplasty (pedicled greater omentum) reduces bile leaks and infection
- Calcified cysts may be dead; if doubt exists whether cyst is active, follow on ultrasonography
PAIR procedure:
- Percutaneous Aspiration, Injection (scolicidal agent - povidone-iodine or hypertonic saline), Re-aspiration
Laparoscopic marsupialisation (deroofing):
- Cyst aspirated (avoiding spillage) → scolicidal agent instilled → endocyst + daughter cysts removed → biliary communication oversewn → pedicled omentum sutured to margins (omentoplasty)
- If cyst small and superficial: cystopericystectomy (entire cyst removed intact)
Pulmonary Hydatid Disease
- Lung is the second commonest organ affected
- Right lung, lower lobes slightly more often involved; usually single
- "Meniscus" / "Crescent" sign on CXR: air between pericyst and laminated membrane = sign of impending rupture
- "Water-lily sign" on CT: collapsed endocyst floating on residual fluid after rupture
- Treatment: primarily surgical
All content above is drawn exclusively from Bailey and Love's Short Practice of Surgery, 28th Edition (ISBN 9780367548117).
Hypertension in pediatric
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
I now have comprehensive content. Let me compile the full answer:
Hypertension in Pediatrics
Sources: Rosen's Emergency Medicine, Tintinalli's Emergency Medicine, National Kidney Foundation Primer on Kidney Diseases 8e, Comprehensive Clinical Nephrology 7e
1. DEFINITION AND CLASSIFICATION
Unlike adults, pediatric blood pressure (BP) is interpreted using sex, age, and height (for children aged 1-12 years). The 2017 American Academy of Pediatrics (AAP) guidelines are the current standard.
BP Classification Table (AAP 2017)
| Category | Age 1 to <13 years | Age ≥13 years |
|---|---|---|
| Normal BP | <90th percentile | <120/80 mmHg |
| Elevated BP | ≥90th to <95th percentile OR 120/80 to <95th percentile | 120/<80 to 129/<80 mmHg |
| Stage 1 Hypertension | ≥95th percentile to <95th + 12 mmHg, OR 130/80 to 139/89 mmHg (whichever is lower) | 130/80 to 139/89 mmHg |
| Stage 2 Hypertension | ≥95th percentile + 12 mmHg OR ≥140/90 mmHg (whichever is lower) | ≥140/90 mmHg |
- Elevated BP = sustained on 3 or more occasions
- Normative data is based on children with normal BMI (NHANES data)
- For children ≥13 years: definitions align with adult AHA/ACC criteria
- Tintinalli's Emergency Medicine; National Kidney Foundation Primer
Hypertensive Crisis Terminology
- Hypertensive urgency: Severely elevated BP without evidence of target organ damage
- Hypertensive emergency: BP exceeding the 99th percentile for age/sex with acute end-organ damage requiring immediate treatment
- Acute severe hypertension (2017 AAP preferred term): Any acute symptomatic presentation of hypertension
- Target organs most commonly damaged: CNS, kidneys, cardiovascular system
- Hypertensive crises in younger children are usually secondary to an underlying disease
2. EPIDEMIOLOGY
- Prevalence of clinical hypertension in pediatrics: approximately 3.5%
- Essential hypertension now affects 3-5% of US adolescents
- Boys, adolescents, and Hispanic and African American races have higher rates in the USA
- Associated risk factors: obesity, family history, sedentary lifestyle, high dietary sodium, African ancestry, history of prematurity and/or low birth weight
- If left untreated: increased risk of adult hypertension, cardiovascular disease, and metabolic syndrome
- Rosen's Emergency Medicine; Comprehensive Clinical Nephrology
3. AETIOLOGY
Primary (Essential) Hypertension
- Once considered rare in children; now routinely encountered in clinical practice
- More prevalent in adolescents, especially obese adolescents
- No identifiable underlying cause
- Risk factors: obesity, family history, sedentary lifestyle, high sodium diet
Secondary Hypertension
Elevated BP due to an identifiable, underlying cause. Secondary causes are more common in younger children.
Causes by Age Group
| Age Group | Common Causes |
|---|---|
| Newborn | Renal: thrombosis (renal vein/artery), stenosis, polycystic kidney disease; Heart: coarctation of the aorta; Endocrine: pheochromocytoma, Cushing's disease |
| Preschool/Kindergarten (<6 yr) | Renal: parenchymal disease, vascular disease; Heart: coarctation of the aorta; Endocrine: pheochromocytoma, Cushing's disease |
| School age (6-10 yr) | Endocrine: pheochromocytoma, Cushing's disease, thyrotoxicosis |
| Adolescence | Essential hypertension (especially obese); Renal: parenchymal, vascular; Endocrine: pheochromocytoma, Cushing's, thyrotoxicosis; Drugs: cocaine, amphetamines, NSAIDs, MAO inhibitors, steroids, calcineurin inhibitors (cyclosporine/tacrolimus) |
- Tintinalli's Emergency Medicine
Summary of Secondary Causes (By Category)
- Renal (most common overall): Glomerulonephritis, haemolytic-uraemic syndrome, FSGS, renal dysplasia, polycystic kidney disease, chronic infections, obstructive lesions; renovascular disease (renal artery stenosis, fibromuscular dysplasia) - most common secondary cause in children
- Cardiovascular: Coarctation of the aorta
- Endocrine: Pheochromocytoma/neuroblastoma (catecholamines), Cushing's syndrome (cortisol excess), hyperthyroidism
- Neurological: Elevated intracranial pressure (space-occupying lesions, acute haemorrhage, infection, CSF obstruction) → body elevates BP to maintain cerebral perfusion pressure
- Medications/Toxins: Oral contraceptives, steroids, stimulants (cocaine, amphetamines), NSAIDs, calcineurin inhibitors
- Genetic/Structural: Neurofibromatosis type 1, monogenic tubular disorders
- Neonatal special risk: Umbilical vein catheter manipulation → risk of renal vein thrombosis
4. CLINICAL FEATURES
Symptoms (Range from Mild to Life-Threatening)
| Severity | Manifestations |
|---|---|
| Mild | Headache, nausea, vomiting, visual changes, anxiety |
| Severe | Hypertensive encephalopathy, focal neurological deficits |
| Cardiac | Chest pain, shortness of breath, acute heart failure, pulmonary oedema |
| Renal | Anuria, acute kidney injury |
| Neonates/Young infants | Feeding problems, irritability or lethargy, respiratory distress, seizures |
Many children are completely asymptomatic - hypertension is often detected on routine examination.
History Points to Elicit
- Maternal complications at birth, gestational age
- Umbilical vein catheter manipulation (risk of renal vein thrombosis)
- Dietary salt intake
- Family history of hypertension
- Palpitations, weight loss, flushing, diarrhoea (endocrine causes)
- Snoring/pauses in sleep (obstructive sleep apnoea)
- Medications and substances
- Rosen's Emergency Medicine
Physical Examination
- 4-extremity blood pressure - to look for coarctation of the aorta (BP higher in arms than legs)
- Signs of secondary causes: café-au-lait spots (NF1), moon face/buffalo hump (Cushing's), abdominal bruit (renal artery stenosis)
5. BP MEASUREMENT
- Gold standard: Auscultation - all normative pediatric data generated by auscultation
- Oscillometric devices: Known to overestimate BP by up to 5-10 mmHg in children; elevated readings must always be confirmed by manual auscultation
- Confirmed hypertension = BP elevated on 3 or more separate occasions
Ambulatory Blood Pressure Monitoring (ABPM)
- White-coat hypertension: Elevated office BP + normal ABPM (isolated office hypertension)
- Masked hypertension: Normal office BP + hypertension on ABPM
- Advantages: Distinguishes white-coat from true HTN, detects masked HTN, characterises BP during daily activities and sleep, more closely correlates with end-organ changes (LVH) than office-based readings
- 2017 AAP guidelines: Recommend ABPM confirmation of elevated readings where possible; children with CKD + HTN should have annual ABPM
- National Kidney Foundation Primer
6. INVESTIGATIONS / DIAGNOSTIC EVALUATION
Initial Workup (for all children with confirmed HTN)
- Basic metabolic panel (BMP): Electrolytes, creatinine, BUN
- Urinalysis (UA): Haematuria, proteinuria (suggests renal parenchymal disease)
- Lipid panel: Fasting lipid profile
- Kidney ultrasound: Renal parenchymal disease, structural abnormalities
Additional Tests Based on Clinical Context
| Test | Indication |
|---|---|
| Echocardiogram | Exclude coarctation of the aorta; assess left ventricular hypertrophy (LVH) |
| Renal Doppler ultrasound | Assess for renovascular disease, renal artery stenosis, renal vein thrombosis |
| Renin + Aldosterone | Renovascular disease, mineralocorticoid excess (Conn's syndrome) |
| Urine catecholamines | Pheochromocytoma |
| ECG | Assess for LVH, structural cardiac causes |
| Sleep study | History of snoring and pauses in breathing |
| Urine toxicology | Suspected drug abuse |
| HbA1c + liver enzymes | Obese children/adolescents (screen for fatty liver, diabetes) |
- Rosen's Emergency Medicine; National Kidney Foundation Primer
7. MANAGEMENT
Long-Term Treatment Goals
- Achieve BP <90th percentile, or <130/80 mmHg in adolescents ≥13 years
- Children with CKD: target <50th percentile based on ABPM
- Purpose: Reduce end-organ damage and cardiovascular risk in adulthood
A. Lifestyle Modifications (First-Line for Essential Hypertension)
Trial for 6-12 months before pharmacologic therapy in most patients with essential HTN:
- DASH diet: Dietary Approaches to Stop Hypertension - low sodium, plant-based, whole grains, low-fat dairy, lean meats
- Moderate to vigorous exercise on most days of the week
- Achievement and maintenance of normal BMI
- Limited screen time
- Avoidance of precipitating medications/substances
B. Pharmacologic Therapy - Indications
Drug treatment is indicated when:
- HTN persists despite lifestyle changes
- Secondary hypertension identified
- HTN associated with end-organ damage
- HTN associated with chronic disorders (diabetes, CKD)
- Stage 2 hypertension in adolescents
Antihypertensive Drug Classes (Approved for Paediatric Use)
| Drug Class | Examples | Paediatric Dosing Notes |
|---|---|---|
| ACE Inhibitors | Captopril, Enalapril | Captopril: Neonate 0.01-0.05 mg/kg Q8-12h; Infant: 0.05-0.3 mg/kg BID-TID; Child: 0.3-0.5 mg/kg BID-TID; max 6 mg/kg/24h. Adjust in renal failure. Contraindicated in pregnancy |
| Calcium Channel Blockers | Amlodipine | <6 yr: 0.1 mg/kg/day (max 5 mg) once daily-BID; ≥6-17 yr: start 2.5 mg once daily; max 10 mg/24h. Allow 5-7 days before adjusting dose |
| Beta-blockers | Metoprolol, Atenolol | Metoprolol ≥1 yr: 1-2 mg/kg/24h PO ÷ BID; max 6 mg/kg/24h up to 200 mg/24h |
| Diuretics | Hydrochlorothiazide, Spironolactone | Hydrochlorothiazide: ≥6 mo child: 1-2 mg/kg/24h ÷ once daily-BID; max 100 mg/24h |
| Alpha-blockers / Vasodilators | Hydralazine | Infant/child: 0.75-1 mg/kg/24h PO ÷ Q6-12h; max 7.5 mg/kg/24h; ARBs also approved |
C. Management of Hypertensive Emergency
- Immediate IV antihypertensives - avoid rapid correction (risk of cerebral ischaemia)
- Target: Reduce BP by no more than 25% in the first 8 hours
- IV agents used: Labetalol, hydralazine, nicardipine, sodium nitroprusside
- Identify and treat underlying cause
- Monitor for end-organ damage: neurological status, urine output, ECG
8. COMPLICATIONS / END-ORGAN DAMAGE
| Organ System | Complication |
|---|---|
| CNS | Hypertensive encephalopathy, stroke, seizures |
| Cardiovascular | Left ventricular hypertrophy (LVH), heart failure |
| Renal | Acute kidney injury, CKD progression, proteinuria |
| Eyes | Hypertensive retinopathy, papilloedema |
| Long-term | Increased risk of adult hypertension, CVD, metabolic syndrome |
9. QUICK SUMMARY - KEY POINTS
| Feature | Key Point |
|---|---|
| Definition | BP >95th percentile on ≥3 occasions (age 1-12) or >130/80 mmHg (age ≥13) |
| Prevalence | ~3.5% in paediatrics; 3-5% in US adolescents |
| Most common secondary cause | Renal disease (glomerulonephritis, renovascular disease) |
| Most common cause overall (adolescents) | Essential/primary hypertension |
| Neonates and young children | Always suspect secondary cause |
| BP measurement | Auscultation is gold standard; oscillometric overestimates by 5-10 mmHg |
| ABPM role | Diagnose white-coat and masked HTN; preferred for CKD monitoring |
| First-line treatment | Lifestyle modification (DASH diet, exercise, weight management) |
| Pharmacologic first-line | ACE inhibitors or CCBs most commonly used |
| Emergency target | Reduce BP no more than 25% in first 8 hours |
Syndrome which includes hypertension
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
I now have excellent content from multiple authoritative textbooks. Here is the comprehensive answer:
Syndromes That Include Hypertension
Hypertension is a feature of many distinct syndromes, spanning endocrine, renal, genetic, cardiovascular, and obstetric categories. Below is a systematic classification.
1. ENDOCRINE SYNDROMES
A. Conn Syndrome (Primary Aldosteronism)
- Pathology: Tumour of zona glomerulosa cells (or bilateral adrenal hyperplasia) → excess aldosterone secretion
- Mechanism: Aldosterone drives renal sodium and water retention → increased blood volume and BP
- Key features:
- Hypertension (almost always present)
- Hypokalemia (muscle weakness, occasionally paralysis from depressed action potentials)
- Mild metabolic alkalosis
- Slight increase in extracellular fluid and blood volume
- Mild hypernatraemia (usually <4-6 mEq/L rise)
- Suppressed plasma renin (hallmark diagnostic criterion - due to feedback suppression from volume expansion)
- Treatment: Surgical removal of tumour OR spironolactone/eplerenone (mineralocorticoid receptor antagonists)
- Guyton and Hall Medical Physiology; Fuster & Hurst's The Heart
B. Cushing Syndrome (Glucocorticoid Excess / Hypercortisolism)
- Pathology: Excess cortisol from any cause (exogenous steroids, ACTH-dependent, ACTH-independent)
- Key clinical features (with approximate frequencies):
- Truncal obesity (90%)
- Hypertension (85%) - due to mineralocorticoid effects of cortisol + increased angiotensinogen
- Decreased glucose tolerance / diabetes (80%)
- Hirsutism (70%)
- Wide purple abdominal striae (65%)
- Osteoporosis (55%)
- Moon face, plethoric facies
- Easy bruising, thin skin
- Buffalo hump (dorsocervical fat pad)
- Proximal muscle weakness
- Mechanism of hypertension: Cortisol has weak mineralocorticoid activity; also upregulates angiotensinogen, increases vascular sensitivity to catecholamines
- Harvey Cushing originally described 11 patients with moon facies, truncal obesity, hypertension, and other features in 1932
- Swanson's Family Medicine Review; Campbell-Walsh-Wein Urology
C. Pheochromocytoma
- Pathology: Catecholamine-secreting tumour of adrenal medulla (or extra-adrenal paraganglioma)
- Classic presentation: "Spells" of headache, hyperhidrosis, palpitations, cardiac arrhythmias, tremulousness, anxiety
- Hypertension features:
- Paroxysmal hypertension is the classic sign (but documented in only ~30-50% of patients)
- Can occur on background of baseline essential hypertension
- ~5% of patients remain normotensive
- Norepinephrine-secreting → alpha-adrenergic vasoconstriction → predominantly diastolic hypertension
- Epinephrine-secreting → beta-adrenergic cardiac stimulation → mainly systolic hypertension + tachycardia + sweating, tremors, flushing
- Patients with epinephrine-predominant tumours: hypertension alternating with hypotension
- Can lead to intracranial haemorrhage; seizures in ~5%
- Mechanism: Periodic bursts of catecholamine release → moderate to severe hypertensive episodes → target organ injury
- Note: BP is often only modestly correlated with plasma catecholamine levels
- Fuster & Hurst's The Heart; Campbell-Walsh-Wein Urology
D. Congenital Adrenal Hyperplasia (CAH) - certain forms
- Most common form (21-β-hydroxylase deficiency): Usually causes hypotension from salt-wasting
- 11-β-hydroxylase deficiency form: Accumulation of deoxycorticosterone (mineralocorticoid activity) → hypertension + virilisation
- 17-α-hydroxylase deficiency: Excess mineralocorticoids → hypertension + hypokalemia + absent puberty
- Guyton and Hall Medical Physiology
2. RENAL / GENETIC SYNDROMES
E. Liddle Syndrome
- Genetics: Autosomal dominant gain-of-function mutation in ENaC (epithelial sodium channel - beta or gamma subunit C-terminus), the amiloride-sensitive Na⁺ channel of the collecting tubule
- Mechanism: ENaC constitutively overexpressed at cell membrane, not inhibited by intracellular Na⁺ → permanent sodium retention → hypertension
- Key features:
- Severe hypertension
- Hypokalemia
- Suppressed aldosterone and suppressed renin (distinguishes from Conn's)
- Resembles hyperaldosteronism but aldosterone is actually low ("apparent mineralocorticoid excess" phenotype)
- Pharmacology: Resistant to spironolactone (mineralocorticoid receptor blocker); responsive to amiloride and triamterene (ENaC blockers) - this is the diagnostic differentiator
- Distinguished from AME syndrome: AME responds to both spironolactone and amiloride; Liddle responds only to amiloride
- Brenner & Rector's The Kidney
F. Gordon Syndrome (Pseudohypoaldosteronism Type 2 / Familial Hyperkalemic Hypertension)
- Mirror image of Gitelman syndrome
- Genetics: Autosomal dominant; mutations in WNK kinases (WNK1, WNK4) or KLHL3/CUL3
- Key features:
- Hypertension
- Hyperkalemia (in contrast to Conn's/Liddle's which have hypokalemia)
- Mild hyperchloremic metabolic acidosis (non-anion gap)
- Normal GFR
- Hypercalciuria; normal serum magnesium
- Mechanism: Increased NaCl reabsorption in distal tubule → volume expansion → hypertension + impaired K⁺/H⁺ secretion → hyperkalemia + acidosis
- Comprehensive Clinical Nephrology; National Kidney Foundation Primer
G. Apparent Mineralocorticoid Excess (AME) Syndrome
- Deficiency of 11-β-hydroxysteroid dehydrogenase type 2 (11β-HSD2)
- Normally, 11β-HSD2 converts cortisol (which binds mineralocorticoid receptor) to inactive cortisone in the kidney
- When deficient: cortisol acts like aldosterone → sodium retention, potassium wasting → hypertension
- Features: severe early-onset hypertension, hypokalemia, suppressed aldosterone and renin
- Differential: responds to both spironolactone and amiloride (unlike Liddle's)
3. CARDIOVASCULAR SYNDROMES
H. Coarctation of the Aorta
- Structural narrowing of the descending aorta (usually at or just distal to ductus arteriosus)
- Hypertension pattern: Upper body/arm hypertension with reduced or absent femoral pulses
- Classical finding: BP in legs lower than arms (normally legs > arms by ~20 mmHg)
- A key secondary cause of hypertension in neonates and children
- Associated with Turner syndrome, bicuspid aortic valve
- May go undiagnosed depending on degree of narrowing
4. OBSTETRIC SYNDROMES
I. Pre-eclampsia
- Definition: New-onset hypertension (SBP ≥140 mmHg AND/OR DBP ≥90 mmHg) after 20th week of gestation + at least one additional feature (proteinuria, thrombocytopenia, renal insufficiency, impaired liver function, pulmonary oedema, cerebral/visual symptoms)
- Mechanism: Abnormal cytotrophoblast invasion of spiral arterioles → reduced uteroplacental perfusion → placental ischaemia → widespread maternal vascular endothelial dysfunction:
- Enhanced ET-1, thromboxane, superoxide
- Increased vascular sensitivity to Angiotensin II
- Decreased NO and prostacyclin (vasodilators)
- Elevated sFlt-1 (soluble VEGF receptor) → sequesters free VEGF and PlGF → impaired angiogenesis + renal endotheliosis + proteinuria
- Progression to eclampsia: seizures + high risk of fetal and maternal mortality
- Hypertension remits after delivery - placenta is the central culprit
- Complicates up to 10% of pregnancies
HELLP Syndrome
- Haemolysis, Elevated Liver enzymes, Low Platelets
- Severe variant of pre-eclampsia
- Features: hypertension + haemolysis + elevated AST/ALT + thrombocytopenia
- Fuster & Hurst's The Heart; Brenner & Rector's The Kidney
5. METABOLIC SYNDROME
J. Metabolic Syndrome (Syndrome X / Insulin Resistance Syndrome)
- Characterised by the cluster of:
- Hypertension
- Insulin resistance / impaired glucose tolerance / type 2 diabetes
- Dyslipidaemia (high triglycerides, low HDL)
- Central/truncal obesity (increased waist circumference)
- Associated with increased risk for diabetes and cardiovascular disease
- Obstructive sleep apnoea may predict metabolic syndrome even in the absence of other features
- Antipsychotic medications (especially clozapine, olanzapine) are a cause - up to 40% of patients on long-term antipsychotics have impaired glucose tolerance
- Treatment: weight reduction, increased physical activity, metformin; GLP-1 agonists (liraglutide) show benefit
- Goldman-Cecil Medicine
6. NEUROLOGICAL / OTHER SYNDROMES
K. Obstructive Sleep Apnoea (OSA) Syndrome
- Commonly associated with: hypertension, obesity, increased proinflammatory cytokines, impaired glucose tolerance, insulin resistance
- Mechanism: intermittent hypoxia → sympathetic activation → sustained hypertension
- May predict metabolic syndrome independently
- Harrison's Principles of Internal Medicine
L. Neurofibromatosis Type 1 (NF1)
- Hypertension in NF1 may result from renal artery stenosis (fibromuscular dysplasia involving renal vasculature) or pheochromocytoma (2-5% of NF1 patients)
M. Turner Syndrome
- Hypertension secondary to coarctation of the aorta (present in ~10-20%) and intrinsic cardiovascular abnormalities
Quick Reference Summary Table
| Syndrome | Mechanism of HTN | Key Distinguishing Lab/Feature |
|---|---|---|
| Conn's (Primary Aldosteronism) | Aldosterone excess → Na⁺ retention | ↓ renin, ↑ aldosterone, hypokalemia |
| Cushing Syndrome | Cortisol mineralocorticoid effect + ↑ angiotensinogen | Moon face, striae, truncal obesity |
| Pheochromocytoma | Catecholamine surges | Paroxysmal spells, ↑ urine catecholamines |
| Liddle Syndrome | ENaC gain-of-function → Na⁺ retention | ↓ aldosterone, ↓ renin; responds to amiloride NOT spironolactone |
| Gordon Syndrome (PHA2) | Excess NaCl reabsorption | Hyperkalemia + metabolic acidosis |
| AME Syndrome | 11β-HSD2 deficiency → cortisol acts as aldosterone | ↓ aldosterone, ↓ renin; responds to spironolactone |
| Coarctation of Aorta | Mechanical obstruction | Arms BP > legs BP; absent femoral pulses |
| Pre-eclampsia | Endothelial dysfunction, ↓ NO/prostacyclin | New HTN after 20 weeks + proteinuria |
| HELLP Syndrome | Pre-eclampsia variant | HTN + haemolysis + ↑ LFTs + ↓ platelets |
| Metabolic Syndrome | Insulin resistance, obesity, SNS activation | Cluster of HTN + obesity + dyslipidaemia + glucose intolerance |
| OSA Syndrome | Intermittent hypoxia → SNS activation | Snoring, apnoeas, daytime somnolence |
| CAH (11β-/17α-hydroxylase deficiency) | Excess deoxycorticosterone (mineralocorticoid) | Virilisation or absent puberty |
This is a shared conversation. Sign in to Orris to start your own chat.