Cushing syndrome with flowcharts
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Finding Sources
Reading File
Loading Image
Reading File
Reading File
Searching PubMed
"Cushing syndrome"[MeSH Terms] AND "diagnosis"[MeSH Terms]
Finding Sources
Reading File
Loading Image
I now have all three key flowcharts and comprehensive clinical content. Let me compile the full, detailed response.
Cushing Syndrome
Overview
Cushing syndrome is the clinical state resulting from prolonged, inappropriate exposure to excess glucocorticoids - either exogenous (iatrogenic, the most common cause in developed countries) or endogenous (spontaneous). Spontaneous Cushing syndrome occurs in 2-5 per million people per year. Cushing disease specifically refers to the subset caused by an ACTH-secreting pituitary adenoma.
- Campbell-Walsh Wein Urology, p. 3134
- Goldman-Cecil Medicine, p. 2410
Clinical Features
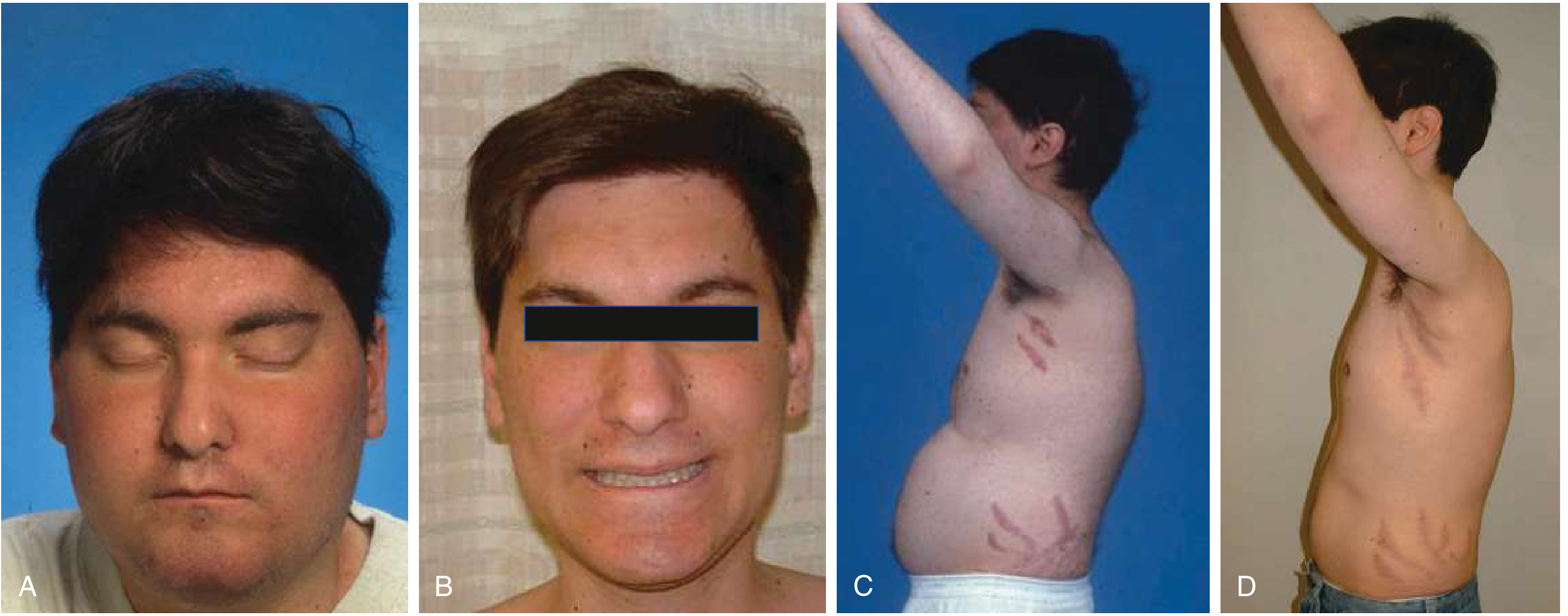
Clinical features of Cushing disease - before (A, C) and after (B, D) transsphenoidal resection. Note "moon facies," facial plethora, abdominal obesity with thin extremities, and violaceous striae.
| System | Findings | Prevalence |
|---|---|---|
| Fat redistribution | Central obesity, moon facies, buffalo hump, supraclavicular fat pads | 90-100% |
| Skin | Violaceous striae (>1 cm), thin skin, easy bruising, hirsutism, facial plethora, acne, hyperpigmentation (ACTH-dependent only) | 70-90% |
| Reproductive | Menstrual disturbances, decreased libido, erectile dysfunction | 70-90% |
| Cardiovascular | Hypertension | 70-90% |
| Musculoskeletal | Proximal muscle weakness, osteoporosis, back pain | 50-70% |
| Metabolic | Glucose intolerance/diabetes, hypokalemic alkalosis, hypercalciuria, renal stones | 50-70% |
| Neuropsychiatric | Depression, irritability, emotional lability, psychosis, disrupted sleep | 50-70% |
| Immunologic | Granulocytosis, lymphopenia, impaired wound healing, recurrent infections | 20-50% |
| Hypercoagulable | DVT, pulmonary embolism | 20-50% |
| Tumor mass effects | Headache, visual field loss, hypopituitarism (pituitary adenoma) | Variable |
- Goldman-Cecil Medicine, p. 2410
- Campbell-Walsh Wein Urology, p. 3138
Etiology & Classification
| Category | Cause | Frequency |
|---|---|---|
| Exogenous | Iatrogenic/factitious glucocorticoid use | Most common overall |
| ACTH-dependent (80% of endogenous) | Pituitary corticotroph adenoma (Cushing disease) | ~70% of spontaneous |
| Ectopic ACTH secretion (small cell lung Ca, pulmonary neuroendocrine tumor, thymic tumor, pancreatic NET, pheo) | ~10% of spontaneous | |
| Ectopic CRH secretion | Rare | |
| ACTH-independent (20% of endogenous) | Adrenal adenoma | ~10% |
| Adrenal carcinoma | ~10% | |
| Primary pigmented nodular adrenal disease (PPNAD) | Rare | |
| Primary bilateral macronodular adrenal hyperplasia | Rare | |
| McCune-Albright syndrome | Rare |
- Goldman-Cecil Medicine, p. 2451 (Table 208-2)
- Quick Compendium of Clinical Pathology, p. 43
Key causes of ectopic ACTH secretion (Goldman-Cecil, Table 208-3):
- Carcinoma of lung (small cell): 19-50%
- Pulmonary neuroendocrine tumor: 2-37%
- Thymic neuroendocrine tumor: 8-12%
- Pancreatic neuroendocrine tumor: 4-12%
- Pheochromocytoma/paraganglioma: 5-12%
- Medullary thyroid carcinoma: 0-5%
Pathophysiology
The zona fasciculata of the adrenal cortex secretes up to 20 mg of cortisol daily, regulated by the hypothalamic-pituitary-adrenal (HPA) axis:
- Hypothalamus releases CRH (and vasopressin) → stimulates anterior pituitary corticotrophs
- Anterior pituitary releases ACTH (cleaved from POMC) → stimulates adrenal cortex
- Cortisol feeds back to suppress both CRH and ACTH
- Normal cortisol follows a circadian rhythm: peak in the morning, nadir at ~11 PM
In Cushing syndrome, this normal feedback loop is disrupted - cortisol remains elevated even at midnight, which is the basis for the late-night salivary cortisol test.
- Campbell-Walsh Wein Urology, p. 3134
Pseudo-Cushing States (Must Exclude)
The following conditions can cause hypercortisolism with some clinical features of Cushing syndrome:
With some clinical features: Pregnancy, depression, alcohol dependence, glucocorticoid resistance, morbid obesity, poorly controlled diabetes
Without clinical features: Physical stress (surgery, pain), malnutrition/anorexia nervosa, intense chronic exercise, hypothalamic amenorrhea, corticosteroid-binding globulin excess
- Campbell-Walsh Wein Urology, Box 106.1, p. 3138
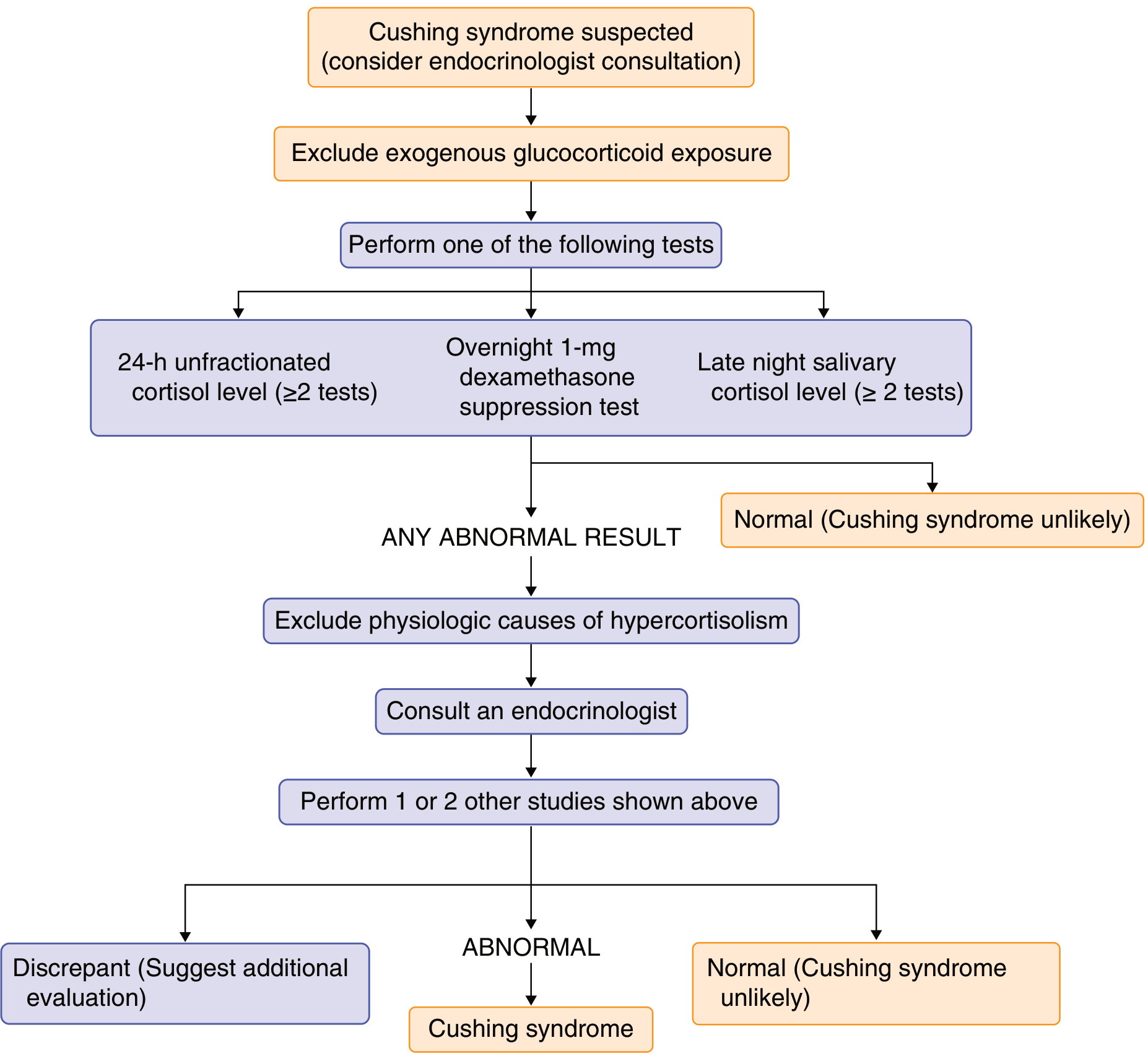
Diagnosis
Flowchart 1 - Screening for Cushing Syndrome (Endocrine Society / Goldman-Cecil, Fig. 205-8)
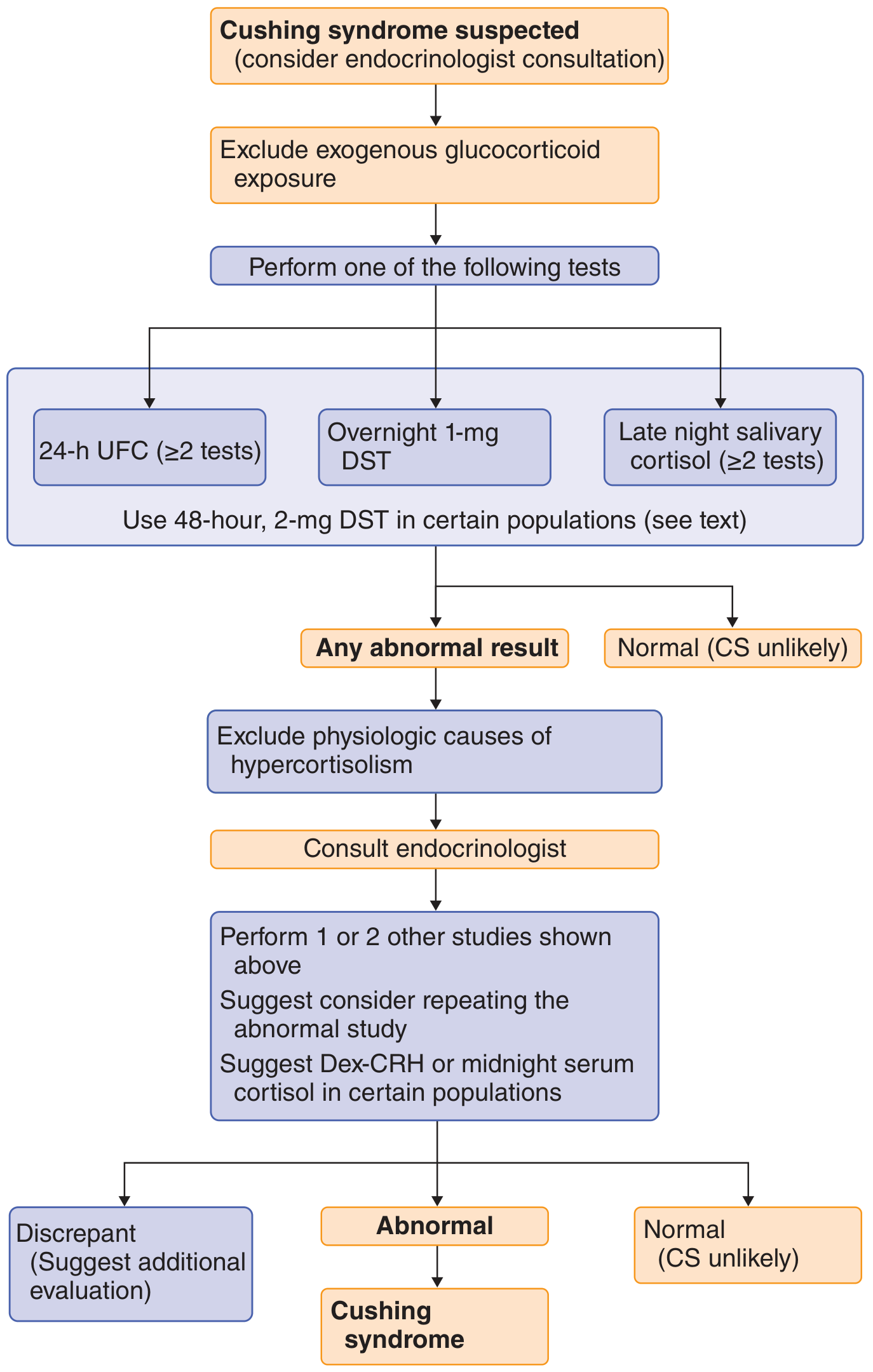
Flowchart 2 - Detailed Algorithm (Goldman-Cecil Fig. 208-4, based on Endocrine Society Clinical Practice Guideline)
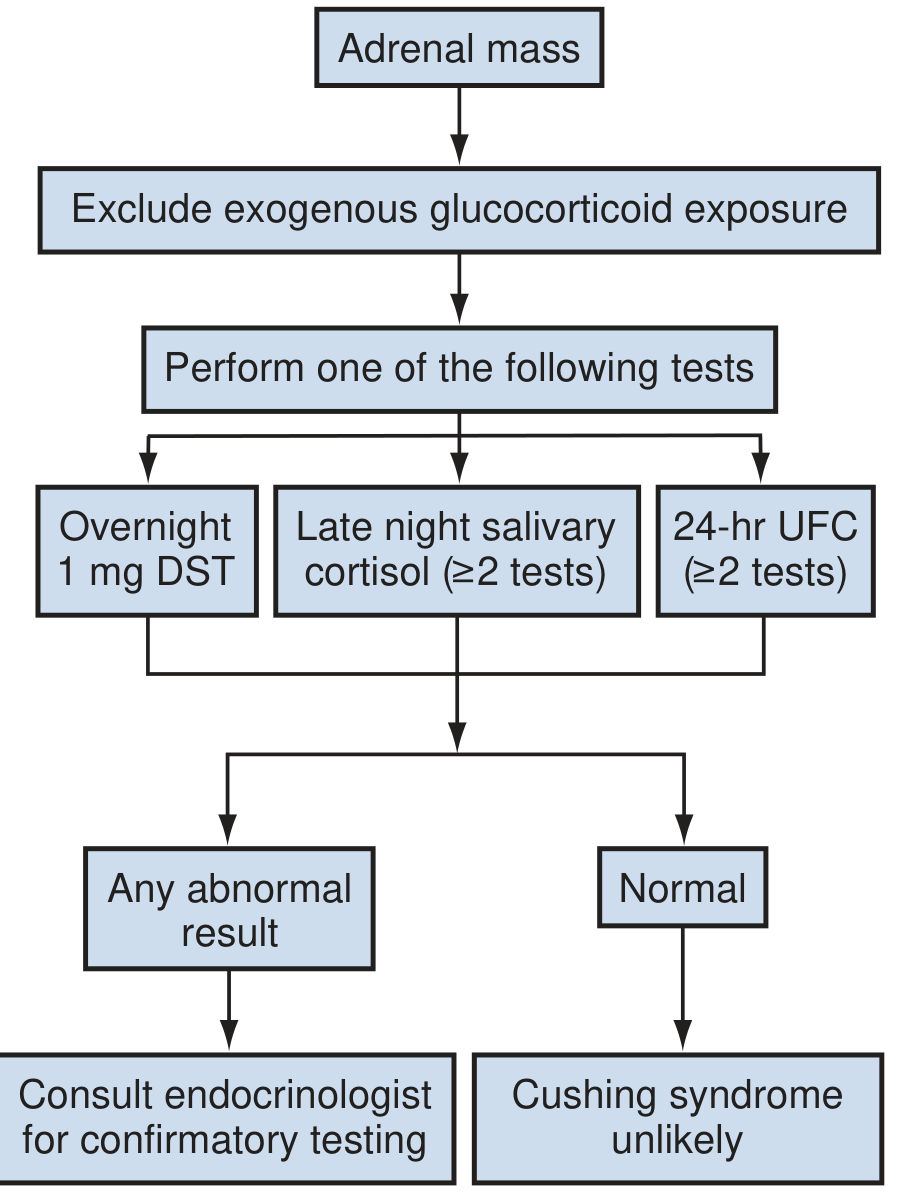
Flowchart 3 - Adrenal Incidentaloma Screening (Campbell-Walsh, Fig. 106.9)
Step 1: Confirm Hypercortisolism
First, exclude exogenous glucocorticoid exposure. Then perform at least two of the following screening tests (at least 2 results must be abnormal):
| Test | Method | Positive (Cushing) Result | Notes |
|---|---|---|---|
| 1-mg Overnight DST | Dexamethasone 1 mg at 11 PM; measure cortisol at 8 AM | Serum cortisol >1.8 μg/dL | Cut-off of 5 μg/dL is more specific but less sensitive. False positives with CYP3A4 inducers (rifampin, phenytoin) |
| 24-hr Urinary Free Cortisol (UFC) | Two separate 24-hr collections | Above upper normal limit (must exceed 4× normal to be diagnostic) | Biologic variation is a limitation |
| Late-Night Salivary Cortisol | Sample at 11 PM-midnight (×2) | >0.09 μg/uL (>145 ng/dL) | Sensitivity 80-90%, specificity 70-90%; best screening test by some authors (100% specificity, 91-93% sensitivity in some series); measures free cortisol; unaffected by CBG |
- Goldman-Cecil Medicine, p. 2451
- Quick Compendium of Clinical Pathology, p. 43
DST interpretation table (Goldman-Cecil, Table 205-10):
| Cause | Plasma ACTH | Low-Dose DST | High-Dose DST | CRH Stimulation |
|---|---|---|---|---|
| Adrenal adenoma | Undetectable | No suppression | No suppression | No response |
| Pituitary adenoma (Cushing disease) | Elevated | No suppression | Suppression | Exaggerated response |
| Ectopic ACTH | Very elevated | No suppression | No suppression | No response |
Step 2: Determine ACTH Dependence - Measure Plasma ACTH
| ACTH Level | Interpretation | Next Step |
|---|---|---|
| <5 pg/mL (undetectable) | ACTH-independent (adrenal source) | Adrenal imaging (CT/MRI) |
| 5-15 pg/mL | Borderline - consider CRH stimulation; suppressed DHEA-S supports ACTH-independent | Further testing |
| >15 pg/mL | ACTH-dependent (pituitary or ectopic) | CRH stimulation, MRI pituitary, IPSS |
| >100 pg/mL | Very high - suggests ectopic ACTH or adrenal insufficiency |
Step 3: Localize the ACTH Source (ACTH-Dependent Only)
| Test | Sensitivity | Specificity | Notes |
|---|---|---|---|
| MRI pituitary | ~60% | Variable | 10% of normal people have pituitary MRI abnormalities; many microadenomas invisible |
| High-dose DST (2 mg q6h × 2 days) | ~80% | ~65% | Pituitary tumors suppress; ectopic does not (but some ectopic tumors have GC receptors - decreasing utility) |
| CRH stimulation test | 93% | 100% | ACTH should rise >35% above baseline in Cushing disease; no response in ectopic ACTH |
| Bilateral Inferior Petrosal Sinus Sampling (BIPSS) | ~95% | ~95% | Gold standard for distinguishing pituitary vs ectopic ACTH; central-to-peripheral ACTH ratio >3 (or >2 after CRH) = pituitary source; small risk of stroke |
- Goldman-Cecil Medicine, p. 2411
- Quick Compendium of Clinical Pathology, p. 43
Flowchart 4 - Differential Diagnosis and Treatment of Cushing Syndrome (Goldman-Cecil Fig. 208-5)
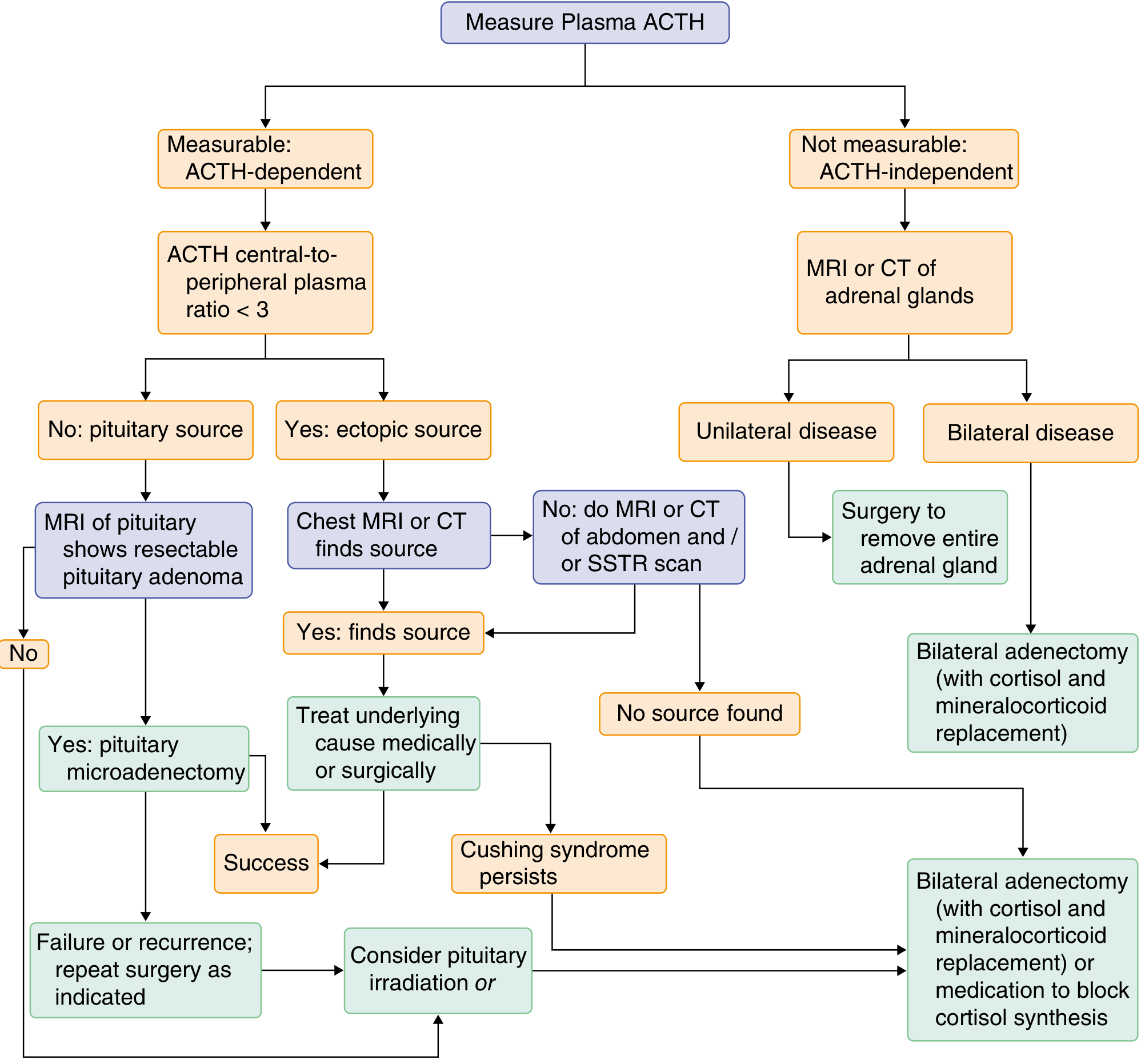
This is the most comprehensive decision flowchart, covering the full pathway from plasma ACTH measurement through treatment selection.
Treatment
Treatment must be multidisciplinary (primary care, endocrinology, neurosurgery, adrenal surgery). Goals: correct hypercortisolism, restore the HPA axis, manage sequelae.
By Cause
1. Exogenous Cushing syndrome
- Gradual tapering of glucocorticoids (HPA axis recovery takes weeks to months)
- Watch for "steroid withdrawal syndrome" - inability to tolerate dose reduction despite apparent HPA normalization
2. Cushing Disease (pituitary adenoma)
- First-line: Transsphenoidal resection of microadenoma - cure rate 60-90% by experienced neurosurgeons
- Macroadenomas: <15% cure rate with surgery
- Postoperative Addisonian state is common; glucocorticoid replacement for up to 1 year
- Recurrence in ~25% - repeat surgery or alternatives
- Alternatives for failed surgery: pituitary irradiation, bilateral adrenalectomy (risk of Nelson syndrome), medical therapy
3. Adrenal Adenoma (ACTH-independent)
- Laparoscopic adrenalectomy - curative in >90% of cases
- Resolution of symptoms takes months to years; watch for postoperative adrenal insufficiency from contralateral gland suppression
4. Adrenal Carcinoma
- Surgery (often multiple operations for primary lesion, recurrences, metastases)
- Adjuvant mitotane (target serum level 14-20 mg/L) for adrenolytic effect
5. Ectopic ACTH secretion
- Resect the primary tumor if localized and non-metastatic
- If unresectable: bilateral adrenalectomy or medical therapy
Medical therapy (when surgery not possible/failed):
-
Ketoconazole - adrenal steroidogenesis inhibitor (max 1600 mg/day)
-
Metyrapone - 11β-hydroxylase inhibitor
-
Mitotane - adrenolytic
-
Mifepristone - glucocorticoid receptor antagonist
-
Combination therapy for refractory cases
-
Goldman-Cecil Medicine, p. 2451-2452
-
Campbell-Walsh Wein Urology, p. 3139
-
Sabiston Textbook of Surgery, p. 1566
Nelson Syndrome
After bilateral adrenalectomy for Cushing disease, loss of cortisol feedback on the pituitary can lead to aggressive growth of the ACTH-secreting adenoma, causing severe hyperpigmentation and mass effects. Risk factors include: longer duration of Cushing disease before diagnosis, younger age, inadequate glucocorticoid replacement, and visible pituitary tumors prior to adrenalectomy.
- Goldman-Cecil Medicine
Summary: Key Numbers to Remember
| Parameter | Value |
|---|---|
| Incidence of spontaneous Cushing syndrome | 2-5 per million/year |
| % ACTH-dependent | 80% |
| % ACTH-independent | 20% |
| Pituitary adenoma (Cushing disease) as % of spontaneous | ~70% |
| Transsphenoidal cure rate (experienced surgeon) | 60-90% |
| Recurrence rate after pituitary surgery | ~25% |
| Adrenalectomy cure rate (primary adrenal Cushing) | >90% |
| 1-mg overnight DST: positive cutoff | Cortisol >1.8 μg/dL |
| Late-night salivary cortisol: positive cutoff | >145 ng/dL (>0.09 μg/uL) |
| ACTH >15 pg/mL | Suggests ACTH-dependent disease |
| BIPSS central:peripheral ratio | >3 = pituitary source |
Recent Evidence
A 2023 meta-analysis in JCEM (PMID 36453141) systematically reviewed dynamic testing (CRH stimulation, DDAVP, high-dose DST, BIPSS) for differentiating pituitary from ectopic ACTH-dependent Cushing - BIPSS remains the most reliable test. A 2024 systematic review (PMID 39002895) evaluated imaging modalities for localizing ectopic ACTH syndrome, finding no single modality is sufficient and multimodality imaging is needed.
This is a shared conversation. Sign in to Orris to start your own chat.