is ampoterecin b an antibiotics
Reading File
Finding Sources
Searching the Web
amphotericin B classification antibiotic or antifungal mechanism of action
Reading File
Reading File
Loading Image
Here is a thorough answer based on authoritative pharmacology textbooks:
Is Amphotericin B an Antibiotic?
Short answer: It depends on how you define "antibiotic."
The Terminology
The word antibiotic literally means "against life" and was originally coined to describe any substance produced by a microorganism that kills or inhibits another microorganism. Under that broad definition, yes - Amphotericin B qualifies as an antibiotic, because it is a natural product derived from a bacterium (Streptomyces nodosus) that kills fungi.
However, in everyday clinical language, "antibiotic" almost always means antibacterial - a drug that targets bacteria. Amphotericin B does not target bacteria at all.
So in clinical practice, Amphotericin B is correctly classified as an antifungal agent, specifically in the polyene class.
What Is Amphotericin B?
| Property | Detail |
|---|---|
| Drug class | Polyene antifungal (polyene macrolide) |
| Source | Produced naturally by Streptomyces nodosus |
| Structure | Amphoteric polyene macrolide with a large lactone ring |
| Clinical use | Serious systemic fungal infections and leishmaniasis |
- Katzung's Basic and Clinical Pharmacology, 16th Ed.: "Amphotericin A and B are antifungal antibiotics produced by Streptomyces nodosus."
- Lippincott Pharmacology: "Amphotericin B is a naturally occurring polyene antifungal produced by Streptomyces nodosus."
Mechanism of Action
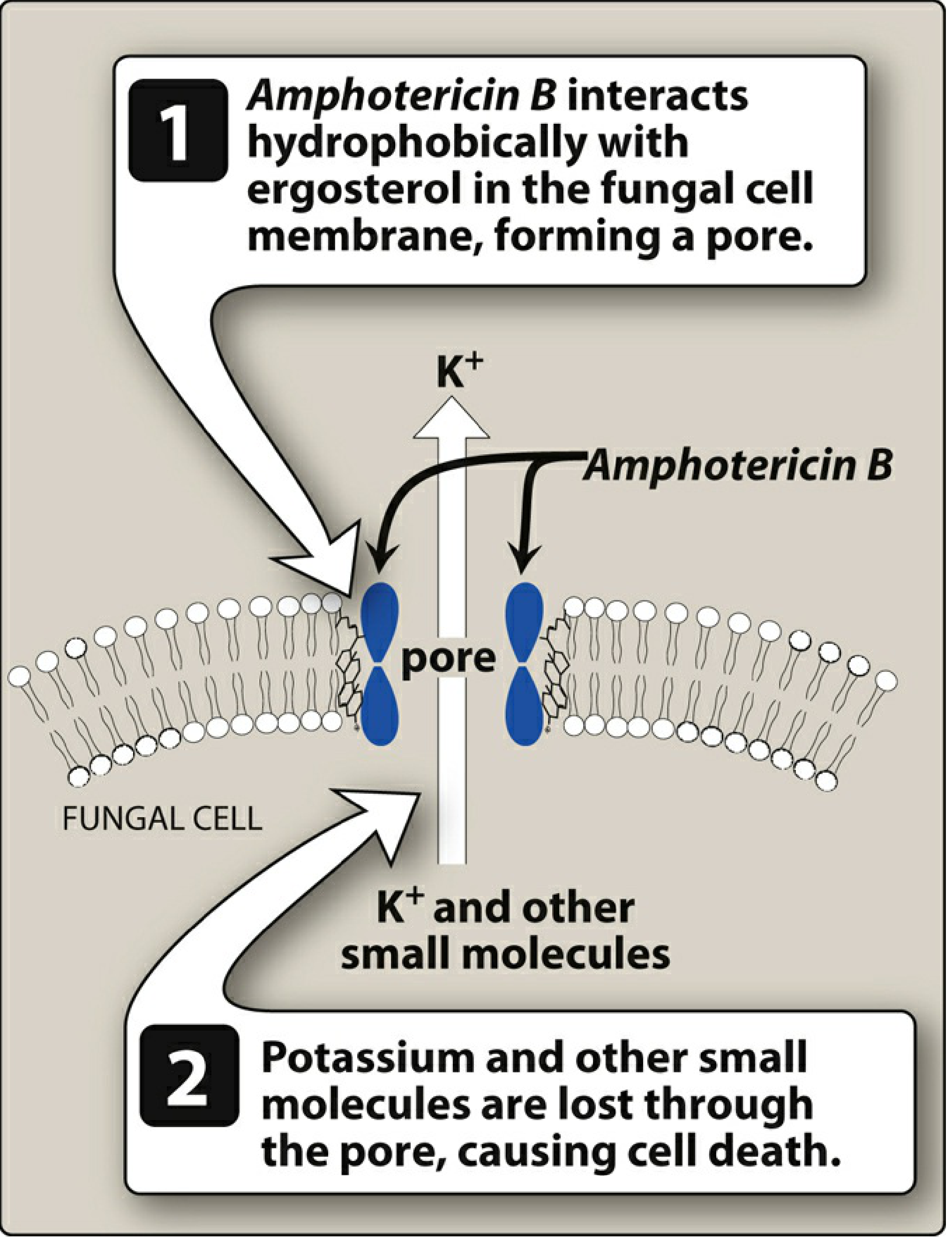
Amphotericin B works by binding to ergosterol - the sterol unique to fungal cell membranes (humans have cholesterol instead). Once bound, it forms pores (channels) in the membrane, causing potassium (K+) and other small molecules to leak out, leading to cell death.
This selective binding to ergosterol (rather than cholesterol) is why the drug targets fungi and not human cells - though it does have some affinity for human cholesterol, which accounts for its significant toxicity.
Antifungal Spectrum
Amphotericin B is effective (either fungicidal or fungistatic) against a wide range of organisms:
- Candida albicans
- Cryptococcus neoformans
- Histoplasma capsulatum
- Coccidioides immitis
- Blastomyces dermatitidis
- Many strains of Aspergillus
- Also used for leishmaniasis (a protozoal infection)
Resistance
Fungal resistance to Amphotericin B is infrequent but occurs through decreased ergosterol content in the fungal membrane, removing the drug's binding target.
Key Adverse Effects
Amphotericin B has a low therapeutic index and is the most toxic antifungal in current use:
- Nephrotoxicity (most significant - renal impairment)
- Infusion-related reactions: fever, chills, headache
- Hypokalemia (from K+ loss)
- Anemia
Lipid formulations (liposomal amphotericin B, amphotericin B lipid complex) were developed to reduce these side effects by limiting nonspecific binding to human cell membranes.
Summary
Amphotericin B is an antifungal, not an antibacterial. The reason some textbooks call it an "antifungal antibiotic" is simply because it is a naturally-derived compound from a bacterium - using the original broad definition of "antibiotic." Clinically, it belongs to the polyene antifungal class and is a first-line treatment for severe, life-threatening fungal infections.
why amphptericin B for leishmaniasis viserel
Finding Sources
Searching the Web
amphotericin B mechanism visceral leishmaniasis ergosterol Leishmania
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Excellent - got everything needed from Goodman & Gilman and Katzung. Here is the full answer:
Why Is Amphotericin B Used for Visceral Leishmaniasis?
The Core Reason: Leishmania Has Ergosterol, Just Like Fungi
This is the key insight. Human cells use cholesterol in their cell membranes. Fungi use ergosterol. And critically - Leishmania parasites also use ergosterol (not cholesterol) as their primary membrane sterol.
This makes Leishmania vulnerable to the exact same mechanism that amphotericin B uses against fungi.
As Goodman & Gilman's states directly:
"Leishmania has similar sterol composition to fungi, and amphotericin binds fungal sterols preferentially over host cholesterol."
How It Kills the Parasite (Mechanism)
The mechanism is identical to its antifungal action:
- Amphotericin B binds to ergosterol (and ergosterol precursors) in the Leishmania cell membrane
- This forms pores (channels) in the membrane
- Ions flood in/out of the cell uncontrollably
- The parasite dies from membrane disruption
Since human cells have cholesterol instead of ergosterol, amphotericin has much lower affinity for human membranes - giving it selective toxicity toward the parasite.
Why It Is Preferred Clinically
| Situation | Why Amphotericin B Is Used |
|---|---|
| Antimonial-resistant VL | First-line pentavalent antimonials (sodium stibogluconate) have high resistance rates in parts of India (Bihar) - >60% resistance in some regions |
| Immunocompromised patients | Amphotericin is effective even when the immune system is suppressed (HIV, transplant) |
| USA/non-endemic countries | FDA-recommended agent for visceral leishmaniasis |
| Efficacy | Cures >90-95% of VL cases - higher than antimonials |
- Goodman & Gilman's: "Amphotericin B is a highly effective antileishmanial agent that cures more than 90% of visceral leishmaniasis cases and is the drug of choice for antimonial-resistant cases."
Liposomal Amphotericin B - the Preferred Formulation
Regular amphotericin B is quite toxic (nephrotoxicity, infusion reactions). Liposomal amphotericin B (L-AmB) is the preferred form for visceral leishmaniasis because:
- The lipid shell preferentially delivers the drug to macrophages - which are exactly where Leishmania hides inside the body
- Much less nephrotoxicity than conventional amphotericin
- Shorter course possible - in India, even a single dose of liposomal amphotericin shows excellent cure rates
Dosing (Katzung):
- Liposomal preparation: 3 mg/kg/day IV on days 1-5, 14, and 21 (total 21 mg/kg)
- Conventional: 1 mg/kg every other day for up to 30 days
Summary in One Sentence
Amphotericin B kills Leishmania because the parasite uses ergosterol in its cell membrane (just like fungi), which the drug binds to form lethal pores - and it is clinically preferred because antimonial resistance is widespread and liposomal formulations deliver the drug directly to macrophages where the parasite lives.
pentamidine
Finding Sources
Searching the Web
pentamidine mechanism of action clinical uses pharmacology
Reading File
Reading File
Reading File
Reading File
Loading Image
Here is a complete pharmacology overview of pentamidine from multiple authoritative textbooks:
Pentamidine - Complete Pharmacology
Structure & Class
Pentamidine is an aromatic diamidine - two benzene rings connected by a pentyl chain, each capped with an amidine group (-C(=NH)-NH₂). It is formulated as the isethionate salt for clinical use.
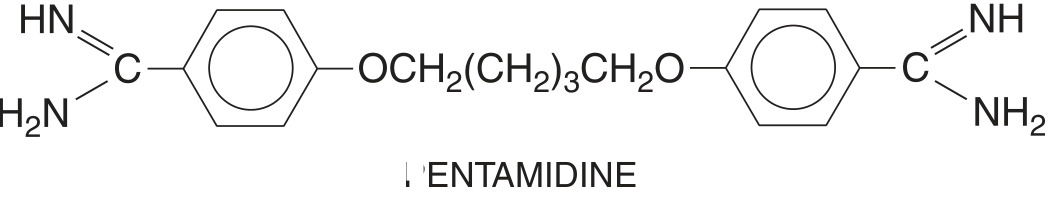
The positive charge on the molecule is important - it drives uptake by specific transporters in parasites.
Mechanism of Action
The mechanism of pentamidine is not fully established - this is explicitly stated across multiple textbooks. What is known:
- T. brucei concentrates pentamidine via an energy-dependent high-affinity uptake system (aquaglyceroporin transporter TbAQP2)
- Once inside the parasite, evidence suggests it interferes with synthesis of RNA, DNA, phospholipids, and proteins
- It likely acts by multiple mechanisms in different parasites
- Resistance occurs when parasites lose the ability to concentrate the drug (transporter mutation/loss)
"The mechanism of action of the diamidines is unknown. The compounds display multiple effects on any given parasite and act by disparate mechanisms in different parasites." - Goodman & Gilman's
Clinical Uses
| Indication | Role | Route & Dose |
|---|---|---|
| PCP (P. jirovecii pneumonia) - treatment | Alternative to TMP-SMX (preferred in sulfonamide allergy or failure) | IV 3 mg/kg/day x 21 days |
| PCP - prophylaxis | Alternative to TMP-SMX in AIDS/immunocompromised | Inhaled aerosol 300 mg monthly |
| West African Trypanosomiasis (T. b. gambiense) - early stage | First-line for children <6 yrs or <20 kg (fexinidazole preferred in adults) | IM/IV 4 mg/kg/day x 7-10 days |
| Visceral leishmaniasis | Alternative when antimonials fail | IM 2-4 mg/kg daily or every other day x up to 15 doses |
| Cutaneous leishmaniasis | Alternative | IM 2-4 mg/kg |
Key limitations:
- Does not cross the blood-brain barrier - therefore useless for late-stage trypanosomiasis (CNS involvement)
- Less effective than TMP-SMX for PCP
- Inferior to suramin for East African trypanosomiasis
Pharmacokinetics
| Parameter | Detail |
|---|---|
| Absorption | Poor oral absorption - must be given parenterally (IV or IM) or inhaled |
| Distribution | Distributes widely; concentrates in liver, kidney, adrenals, spleen, lungs |
| CSF penetration | Negligible - explains ineffectiveness in CNS disease |
| Protein binding | ~70% bound to plasma proteins |
| Half-life | Initial t½ ~6 hours; terminal t½ ~12 days (accumulates in tissues) |
| Elimination | Excreted very slowly in urine over weeks-months |
Adverse Effects
Pentamidine is a highly toxic drug - adverse effects occur in ~50% of patients receiving 4 mg/kg/day. This limits its use to situations where other options fail.
| Adverse Effect | Notes |
|---|---|
| Hypoglycemia | Due to inappropriate insulin release from pancreatic beta cells - appears 5-7 days after starting, can persist weeks; life-threatening |
| Hyperglycemia / diabetes | Can follow the hypoglycemic phase (beta cell destruction) |
| Nephrotoxicity | Reversible renal insufficiency - very common |
| Hypotension | Rapid IV infusion causes severe hypotension, tachycardia, dizziness - must infuse slowly over 2 hours with patient recumbent |
| Pancreatitis | Acute pancreatitis |
| Cardiac arrhythmias | Including ventricular arrhythmias, QT prolongation |
| Sterile abscesses | At IM injection sites |
| Hyperkalemia, hypocalcemia | Electrolyte disturbances |
| Thrombocytopenia, hepatotoxicity | Less common |
| Inhaled form | Generally well tolerated - may cause cough, dyspnea, bronchospasm |
Monitor blood glucose closely - hypoglycemia is unpredictable and potentially fatal.
Summary
| Feature | Key Point |
|---|---|
| Class | Aromatic diamidine |
| MOA | Unknown; likely disrupts DNA/RNA/protein synthesis; enters parasite via TbAQP2 transporter |
| Main uses | PCP (alternative), West African trypanosomiasis (early), leishmaniasis (alternative) |
| Cannot treat | CNS/late-stage trypanosomiasis (no CSF penetration) |
| Most dangerous ADR | Hypoglycemia (from beta cell destruction) + nephrotoxicity |
| Preferred form for PCP prophylaxis | Inhaled aerosol 300 mg/month |
- Katzung's Basic and Clinical Pharmacology, 16th Ed. (p. 1452)
- Goodman & Gilman's Pharmacological Basis of Therapeutics
- Lippincott Illustrated Reviews: Pharmacology
This is a shared conversation. Sign in to Orris to start your own chat.