whole body ct in detail and protocols for adult whole body and pediatric whole body ct , there is a question that Write down any two protocols for adult whole-body CT ?
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Searching the Web
whole body CT scan protocols adult pediatric indications technique parameters radiology
Finding Sources
Reading File
Reading File
I now have sufficient information from authoritative textbook sources to provide a detailed, comprehensive answer. Let me compile this into a well-structured response.
Whole-Body CT (WBCT): Comprehensive Overview
What Is Whole-Body CT?
Whole-body CT (WBCT), also called a "pan-scan", refers to CT imaging of the head, neck, chest, abdomen, and pelvis performed in a single session. It uses intravenous (IV) contrast and modern multidetector CT (MDCT) technology to rapidly acquire images of all major body regions. It is most commonly used in the setting of major trauma, but also has utility in oncological staging, occult disease detection, and unexplained weight loss.
- Radiation exposure from a WBCT is approximately 3× the average background atmospheric radiation exposure
- Diagnostic yield for unexplained weight loss: ~33.5% — Yamada's Textbook of Gastroenterology
- CT images from a pan-scan can be reconstructed to evaluate the entire spine (cervical, thoracic, lumbar) without additional scans
Adult Whole-Body CT — Detailed Protocol
Indications
- Blunt polytrauma (motor vehicle collision, falls from height, crush injuries)
- Penetrating trauma to the torso
- Hemodynamically stable patients with multisystem injury
- Occult injury detection in obtunded or intubated patients
- Oncologic staging / unexplained weight loss
- Suspected aortic or vascular injury
General Principles (Adult)
- Patient must be hemodynamically stable — CT is contraindicated in unstable patients (poor monitoring in scanner, limited rescue capability, aspiration risk)
- IV contrast is mandatory for trauma scans; oral and rectal contrast have largely fallen out of favor in trauma CT
- Contrasted scans can be acquired in:
- CT angiography (CTA) phase — arterial phase, smaller slice thickness, ideal for vascular injury
- Portal venous phase — standard IV contrast CT, best for solid organ injury
✏️ Two Key Protocols for Adult Whole-Body CT
Protocol 1: Trauma Pan-Scan Protocol (Blunt Polytrauma)
| Parameter | Detail |
|---|---|
| Coverage | Head → Neck → Chest → Abdomen → Pelvis |
| Contrast | IV contrast (iodinated); no oral/rectal contrast |
| Phases | Arterial phase (CTA) + Portal venous phase |
| Slice thickness | Thin sections (1–3 mm) for multiplanar reformats |
| Reconstructions | Axial + sagittal + coronal; spine reconstructed from existing dataset |
| Window settings | Bone window, soft tissue window, lung window all generated |
| Spinal evaluation | Thoracic & lumbar spine reconstructed from chest/abdomen CT data; cervical spine CT performed simultaneously with head CT |
| Additional vessels | CTA of vertebral and carotid arteries if blunt cerebrovascular injury suspected (high-risk: head, cervical spine, or chest injuries) |
| Special note | ECG gating still preferred for thoracic aorta if available and heart rate is controlled; modern non-gated protocols using gantry rotation < 0.3 sec show limited motion artefact |
| Sternum | Sagittal reformats of thoracic spine should include the sternum (part of the bony thoracic ring) |
"CT of the thoracic and lumbar spine should be performed as part of a polytrauma CT protocol that includes an intravenous contrast agent for the assessment of vascular injury. The precise imaging parameters will depend on the particular CT system but the axial imaging should allow sagittal and coronal reformats of sufficient diagnostic quality." — Grainger & Allison's Diagnostic Radiology
Protocol 2: Oncologic / Staging Whole-Body CT Protocol
| Parameter | Detail |
|---|---|
| Coverage | Head (if indicated) + Neck + Chest + Abdomen + Pelvis |
| Contrast | IV contrast (portal venous phase dominant); arterial phase if vascular involvement suspected |
| Phases | Single- or dual-phase depending on clinical question |
| Slice thickness | Standard 3–5 mm; thinner for specific lesion characterization |
| Reconstructions | Axial + coronal + sagittal |
| Female patients | Pelvis must always be included (e.g., for unexplained weight loss investigations) |
| Supplementary modality | May be combined with PET-CT for functional imaging (e.g., lymphoma, myeloma, melanoma restaging) |
| Special note | For multiple myeloma: whole-body low-dose CT (or PET-CT) is standard; must be performed in smouldering myeloma and confirmed smouldering MGUS |
| Melanoma | WBCT may be replaced by PET-CT which is highly sensitive for systemic metastasis |
"Whole-body CT imaging has been demonstrated to have a diagnostic yield of 33.5% for unexplained weight loss." — Yamada's Textbook of Gastroenterology
Pediatric Whole-Body CT — Protocol and Key Differences
Core Principle: ALARA
The "As Low As Reasonably Achievable" (ALARA) principle governs all pediatric CT decisions:
- Young, rapidly dividing tissues are more radiosensitive than adult tissues
- CT radiation creates a cumulative lifetime carcinogenic risk
- A dose-response relationship exists between CT-related radiation and brain cancer in children
- The adult pan-scan approach should be avoided in pediatric patients
"The adult trauma assessment with pan-scan should be avoided given long-term implications of ionizing radiation in children." — Sabiston Textbook of Surgery
What Changes in Pediatric CT Protocol?
| Parameter | Adult Protocol | Pediatric Protocol |
|---|---|---|
| Pan-scan default | Yes (in significant trauma) | No — selective imaging only |
| Chest CT | Routinely included | CXR preferred first; chest CT only if CXR suggests aortic injury |
| Abdominal CT | Routine with IV contrast | Guided by clinical presentation + mechanism |
| FAST ultrasound | Mainstay for abdominal screening | Limited utility in stable pediatric patients |
| Radiation dose | Standard adult dose | Reduced dose (weight-based/age-based technique) |
| Multiphase scans | Arterial + venous common | Minimized — single phase when possible |
| Follow-up studies | As needed | Judicious — avoid repeat CT |
| Scope | Full head-to-pelvis | Minimized regions — only what is clinically indicated |
Pediatric Specific Guidance
- Chest X-ray is still valuable and sensitive for significant chest injuries (pneumothorax, hemothorax, rib fractures) in pediatric chest trauma
- Occult pneumothorax on CT in children has unclear clinical relevance — most do not require management changes
- eFAST performs well for pneumothorax and hemothorax in experienced hands (sensitivity/specificity approaching 100%)
- Head CT: indicated for moderate-to-severe TBI; follows PECARN decision rules for mild TBI to avoid unnecessary radiation
- Rib fractures in infants/toddlers (especially posterior) → raise suspicion for non-accidental trauma (child abuse)
- CT abdomen/pelvis: mean radiation dose is 10–15 mSv (Miglioretti et al., 2013)
Pediatric CT Technical Modifications
- Use weight-based and age-adjusted kVp and mAs settings
- Smaller field of view (FOV) due to smaller body habitus
- Faster acquisition preferred to reduce motion artefact (no breath-holds in young children)
- Consider MRI as alternative for non-urgent abdominal/spinal assessment (no radiation)
Summary Comparison Table
| Feature | Adult WBCT | Pediatric WBCT |
|---|---|---|
| Default approach in major trauma | Pan-scan (head–neck–chest–abdomen–pelvis) | Selective, targeted imaging |
| Radiation concern | Moderate | High priority (ALARA) |
| IV contrast | Standard | Used selectively; single phase preferred |
| CXR role | Supplementary | Primary screening tool for chest |
| FAST utility | High in unstable patients | Limited in stable patients |
| Special protocols | Vascular (CTA), oncologic staging | Weight-based dose reduction |
| Contraindications | Hemodynamic instability | Hemodynamic instability + radiation risk |
Sources:
- Grainger & Allison's Diagnostic Radiology
- Sabiston Textbook of Surgery
- Current Surgical Therapy, 14e
- Rosen's Emergency Medicine
- Tintinalli's Emergency Medicine
- Yamada's Textbook of Gastroenterology
Hrct of lungs , technical aspects , volumetric HRCT, Expiratory HRCT , HRCT protocols , artifacts in detail i have to write in a high level exam as msc radiology student
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Searching Images
HRCT lung high resolution CT technique protocol expiratory
I now have comprehensive data from all major respiratory radiology textbooks. Let me compose the full high-level MSc Radiology answer.
HRCT of the Lungs — Complete MSc Radiology Answer
1. Introduction and Definition
High-Resolution CT (HRCT) of the lungs is a specialized CT technique designed to maximize spatial resolution of the lung parenchyma. It combines three essential technical elements:
- Narrow collimation / thin-slice thickness (~1 mm)
- High-spatial-frequency reconstruction algorithm ("sharp" or "lung" kernel)
- Single breath-hold acquisition (to eliminate respiratory motion artefact)
"HRCT is a technique combining narrow collimation/thin-slice thickness (1 mm) and image reconstruction using a high-spatial-frequency algorithm to maximize sharpness in the final image." — Murray & Nadel's Textbook of Respiratory Medicine
HRCT is best suited for the analysis of:
- Diffuse interstitial lung disease (DILD / ILD)
- Small airway disease
- Emphysema
- Bronchiectasis
- Airway disorders (tracheobronchomalacia)
- Pulmonary nodule characterization
2. Technical Aspects of HRCT
2.1 Slice Thickness (Collimation)
- Standard: ≈1 mm (thin-section)
- Reducing below 1 mm yields no significant further improvement in spatial resolution but decreases signal-to-noise ratio (SNR)
- Contrast: routine chest CT uses 3–5 mm reconstructions
2.2 Reconstruction Algorithm (Kernel)
- HRCT uses a high-spatial-frequency algorithm (also called "sharp," "bone," or "lung" kernel)
- This reduces image smoothing → structures appear visibly sharper
- Trade-off: image noise becomes more prominent (grainy appearance)
- Standard soft-tissue CT uses a low-spatial-frequency algorithm ("smooth" kernel) — opposite effect
2.3 CT Numbers and Hounsfield Units (HU)
| Structure | HU Range |
|---|---|
| Air | −1000 HU |
| Normal lung parenchyma | −700 to −900 HU |
| Fat | ~−100 HU |
| Water | 0 HU |
| Soft tissue | +20 to +60 HU |
| Blood clot | ~+100 HU |
| Bone | +400 to +1000 HU |
The total range encountered clinically spans ~2000 HU (−1000 to +1000), but the human eye perceives only 16–20 shades of grey — necessitating window settings.
2.4 Window Settings
| Window | Level (Centre) | Width | Use |
|---|---|---|---|
| Lung window | −700 HU | ~1200 HU | Parenchyma, airways, nodules |
| Mediastinal / soft-tissue window | +20 to +40 HU | ~400 HU | Pleura, hila, mediastinum |
| Bone window | +300–400 HU | ~1500 HU | Ribs, vertebrae |
"To view the lungs, an appropriate window level is −700 HU, with a window width of approximately 1200 HU. For soft tissues, mediastinum, or hila, a window level of 20 to 40 HU with a width of approximately 400 HU is preferred." — Murray & Nadel's Textbook of Respiratory Medicine
2.5 Field of View (FOV)
- A targeted (small) FOV focused on the lungs improves spatial resolution
- Large FOV reduces effective resolution per pixel
- HRCT typically uses the smallest FOV that encompasses both lungs
2.6 Matrix Size
- Standard: 512 × 512 pixel matrix
- Larger matrix → smaller pixel size → improved spatial resolution
2.7 Tube Current (mAs) and Voltage (kVp)
- Standard HRCT: 120 kVp
- For thin/small patients (<50 kg) and paediatrics: 100 kVp recommended (80 kVp causes unacceptable beam hardening)
- Tube current reduction is the most practical dose-reduction strategy:
- 50% reduction in mAs → 50% reduction in effective dose
- Low-dose CT (40–70 mAs) is feasible for lung parenchymal imaging due to inherent high contrast between air and tissue
- Automatic Exposure Control (AEC) / automatic tube current modulation is standard practice
2.8 Pitch
- Pitch = table movement per rotation ÷ beam collimation
- Higher pitch → faster acquisition, lower dose (for some systems)
- MSCT systems with effective mAs setting: dose remains constant regardless of pitch
2.9 Intravenous Contrast
- Not routinely used in HRCT
- Reasons to avoid: iodinated contrast can spuriously increase parenchymal opacification, interfering with interpretation — particularly problematic in comparison/follow-up studies
- IV contrast IS used when there is another indication (e.g., pulmonary embolism, vascular evaluation)
3. Volumetric HRCT
3.1 From Sequential ("Step-and-Shoot") to Volumetric CT
Old technique (single-slice CT):
- Acquired images sequentially with table increments ("step-and-shoot")
- Non-contiguous 1 mm HRCT slices with 10–20 mm gaps between slices
- Problem: misregistration between successive breath-holds
- Could mistake a pulmonary vessel for a nodule — no adjacent slices for comparison
- Required the radiologist to decide intraoperatively whether thin sections were needed
Modern volumetric (helical/spiral) CT:
- X-ray tube rotates continuously while the table moves at a constant speed → spiral data acquisition
- Entire thorax imaged in a single breath-hold (cervicothoracic junction → diaphragm)
- Produces a single contiguous block of anatomic data reconstructable into any slice thickness or imaging plane
3.2 Multislice CT (MSCT) — The Current Standard
MSCT acquires data through multiple parallel detector rows simultaneously during a single tube rotation:
| Generations | Slices/rotation |
|---|---|
| Early MSCT | 4, 8, 16 |
| Modern | 64, 128, 256 |
| Latest | 320, up to 920 slices |
Key advantages of MSCT over single-slice helical CT:
- Volumetric isotropic imaging — contiguous image reconstruction
- Multiplanar and 3D reformats — axial, sagittal, coronal from same dataset
- Retrospective reconstruction — narrow sections (1 mm) acquired but reconstructed as wider sections (3 mm) for routine display; thin-section data preserved for later review without rescanning
- Temporal resolution — gantry rotation times as low as 0.33 sec/rotation
- Improved contrast opacification — rapid scanning during peak contrast phases
"With MSCT the ability to reconstruct narrow-section images retrospectively has transformed the process of nodule characterisation." — Murray & Nadel's Textbook of Respiratory Medicine
3.3 Isotropic Volumetric Imaging
Modern 64-channel+ MSCT can acquire isotropic voxels (equal dimensions in all three planes, typically ~0.5–1 mm³). This enables:
- High-quality reformatted images in any plane
- Virtual bronchoscopy
- Quantitative CT analysis (emphysema quantification, airway wall measurement)
3.4 Postprocessing from Volumetric Data
| Technique | Principle | HRCT Application |
|---|---|---|
| MPR / CMPR | 2D alternate plane views | Airway evaluation, PE |
| Maximum Intensity Projection (MIP) | Only highest-density voxel per ray displayed | Micronodule detection, vascular anatomy |
| Minimum Intensity Projection (MinIP) | Only lowest-density voxel per ray | Emphysema, air trapping, mosaic pattern |
| Volume Rendering | Histogram-based opacity mapping | 3D airway, angiography |
| Virtual Bronchoscopy | Surface/volume rendering → endoscopic simulation | Airway stenosis, subglottic lesions |
| Quantitative CT | Density mask thresholding | Emphysema quantification (−950 HU threshold) |
"Every chest CT is now effectively both a standard, as well as a high-resolution, CT, combining the advantages of each in a single study." — Fishman's Pulmonary Diseases and Disorders
4. Expiratory HRCT
4.1 Rationale and Physiology
Normally, lung CT attenuation increases on expiration due to volume averaging (voxels contain less air as lung deflates). In the presence of air trapping (caused by small airway obstruction), this normal increase in attenuation does not occur — air is trapped in the affected lobules.
Expiratory CT provides the best currently available imaging test to:
- Demonstrate small airway air trapping
- Detect mosaic attenuation pattern caused by small airway disease
- Diagnose tracheobronchomalacia (dynamic collapse of trachea/central bronchi)
- Evaluate bronchiolitis obliterans (e.g., post-transplant BOS)
- Differentiate mosaic attenuation causes: small airway disease vs. vascular disease vs. infiltrative disease
4.2 Technique
Standard technique:
- Postexpiratory thin-section CT acquired during suspended respiration following a forced exhalation
- Ideally reflects residual volume (RV)
- Each postexpiratory image compared with the inspiratory image at the same anatomical level
- Typically acquired at 3 representative levels: upper, middle, and lower lung zones
Dynamic expiratory CT (cine technique):
- CT images acquired during the forced expiratory vital capacity manoeuvre (not just at end-expiration)
- Permits superior detection of tracheobronchomalacia (dynamic collapse best seen during expiration)
- Recommended when patients have difficulty performing the end-expiration breath-hold manoeuvre
- Inspiratory acquisition ideally reflects total lung capacity (TLC)
Technical parameters:
- Low-dose or ultra-low-dose technique (iterative reconstruction or soft-tissue kernel with filtered back projection) to improve conspicuity of air trapping while minimizing dose
- MDCT with thin collimation over the lungs
4.3 Assessment of Air Trapping
Qualitative assessment:
- Areas of abnormally low attenuation that fail to increase normally on expiration = air trapping
- Associated features: reduced vessel calibre and paucity, lack of change in cross-sectional lung area
- MinIP technique enhances conspicuity of air trapping vs. normal parenchyma
Semiquantitative scoring (Stern et al.):
| Score | % of Cross-Sectional Lung Affected |
|---|---|
| 0 | No air trapping |
| 1 | 1–25% |
| 2 | 26–50% |
| 3 | 51–75% |
| 4 | 76–100% |
Total air trapping score = sum across all levels for each lung. Correlates with degree of airflow obstruction on PFTs.
Quantitative CT densitometry:
- Density mask technique: pixels with HU < −910 thresholded and highlighted (air trapping pixels)
- Expiratory/inspiratory (E/I) ratios calculated
- Threshold of −910 HU for expiratory scans
4.4 Clinical Indications for Expiratory CT
| Indication | Rationale |
|---|---|
| COPD / emphysema | Small airway disease, air trapping quantification |
| Asthma | Air trapping in asymptomatic intervals |
| Constrictive/obliterative bronchiolitis | Best diagnostic test; post-BMT, post-lung transplant |
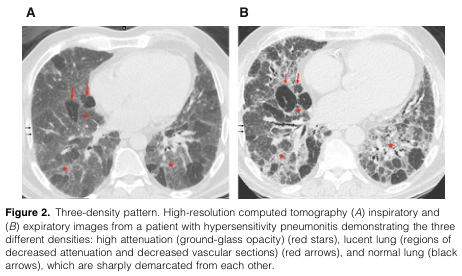
| Hypersensitivity pneumonitis | "Three-density pattern" — GGO + air trapping + normal lung |
| Mosaic attenuation pattern | Differentiate small airway vs. vascular cause |
| Tracheobronchomalacia | Dynamic collapse on expiration |
| Bronchiolitis obliterans syndrome (BOS) | Air trapping is a diagnostic criterion |
5. HRCT Protocols
Protocol 1: Standard Inspiratory HRCT (ILD Protocol)
| Parameter | Setting |
|---|---|
| Patient position | Supine |
| Respiration | Full inspiration (total lung capacity), breath-hold |
| Slice thickness | 1 mm |
| Reconstruction algorithm | High-spatial-frequency ("sharp" / "lung" kernel) |
| kVp | 120 kV (100 kV in thin patients) |
| mAs | Low-dose (40–70 mAs) acceptable for parenchymal imaging |
| Coverage | Lung apices → posterior costophrenic angles |
| IV contrast | Not routine; avoid (falsely increases parenchymal density) |
| Reconstructions | Axial (primary); sagittal + coronal if MSCT |
| Window settings | Lung window (−700 HU / 1200 HU) + mediastinal window |
| Prone series | Added if posterior fibrosis suspected → eliminates dependent atelectasis |
Prone HRCT: When early interstitial fibrosis is suspected, prone imaging eliminates the dependent increased opacification seen in posterobasal segments on supine imaging. Not needed if diffuse lung disease is obvious on CXR.
Protocol 2: HRCT with Expiratory Series (Small Airway / Airway Disease Protocol)
| Phase | Parameters | Rationale |
|---|---|---|
| Inspiratory (supine) | 1 mm, full inspiration, same as above | Baseline morphology |
| Expiratory (supine) | 3 selected levels at end-expiration OR full volumetric | Air trapping, mosaic pattern |
| Optional prone inspiratory | 1 mm | Rule out dependent atelectasis |
| Dynamic expiratory (cine) | Acquired during forced expiration | Tracheobronchomalacia |
Protocol 3: Standard Full-Protocol (Diffuse Lung Disease — Complete)
| Acquisition | Details |
|---|---|
| Supine inspiratory (volumetric) | 1 mm, full inspiration |
| Supine expiratory | 3 levels OR volumetric low-dose |
| Prone inspiratory | 1 mm, full inspiration (if fibrosis suspected) |
| Multiplanar reconstructions | Sagittal + coronal from volumetric data |
Common HRCT Chest CT Protocols Summary Table
| Protocol | Contrast | Inspiratory | Expiratory | Prone | Primary Use |
|---|---|---|---|---|---|
| HRCT standard | No | Yes (1 mm) | No | Optional | ILD, nodules |
| HRCT + expiratory | No | Yes | Yes | Optional | Small airway, BOS, HP |
| CTPA | Yes (arterial) | Yes (3 mm) | No | No | Pulmonary embolism |
| Lung cancer staging | Yes | Yes | No | No | Staging, mediastinum |
| Low-dose screening | No | Yes (1 mm) | No | No | Lung cancer screening |
6. Artifacts in HRCT — In Detail
6.1 Motion Artifacts
Respiratory motion:
- Cause: patient breathes during acquisition
- Appearance: blurring, doubling of structures, loss of sharp margins (especially in lower lobes near diaphragm)
- Effect on HRCT: mimics or obscures ground-glass opacity, interstitial changes
- Prevention: proper breath-hold instructions; shorter acquisition time (MSCT advantage)
Cardiac pulsation:
- Cause: transmitted cardiac motion to adjacent lung
- Appearance: linear streaks, pseudo-nodules, and blurring in the left lower lobe (lingula and medial left lower lobe)
- Can simulate: GGO, fine reticulation, or consolidation adjacent to the heart
- Prevention: ECG-gating (not routine for lung HRCT); faster gantry rotation
6.2 Beam Hardening Artifact
- Cause: The x-ray beam is polychromatic. Lower-energy photons are preferentially absorbed (beam is "hardened") as it passes through dense structures
- Appearance: dark bands or streaks between two high-density objects (e.g., sternum and spine, metallic implants)
- Effect on lung imaging: can cause false low-attenuation areas or streak artefacts
- Solutions: iterative reconstruction; dual-energy CT (DECT); metal artefact reduction algorithms
6.3 Streak Artifact (Metal Artifact)
- Cause: metallic objects (pacemakers, prosthetic valves, sternal wires, chemotherapy ports) cause two mechanisms: (1) photon starvation (insufficient photons penetrating metal → noise) and (2) beam hardening
- Appearance: high and low density streaks radiating from metallic object, severely degrading adjacent images
- Effect on lung HRCT: obscures pulmonary/mediastinal/pleural detail
- Solutions: Metal Artefact Reduction (MAR) algorithms; DECT; increased kVp (to reduce beam hardening)
6.4 Partial Volume Averaging
- Cause: When a structure is smaller than the voxel size, the CT number recorded is an average of the structure and surrounding tissue
- Effect on HRCT: Small nodules, ground-glass opacities, and fine interstitial lines may be under- or over-estimated
- Example: A small vessel crossing a section plane may appear as a pseudo-nodule; a fine interlobular septum may be invisible
- Relevance: This was a major problem with old non-contiguous HRCT where adjacent images were not available for comparison
- Solution: Thin sections (1 mm) minimize partial volume averaging; MSCT's contiguous imaging resolves the pseudo-nodule problem
6.5 Dependent Opacity / Dependent Atelectasis
- Cause: In supine position, gravity causes dependent posterior lung to compress → dependent atelectasis → increased posterior-basal opacification
- Appearance: Posterior subpleural ground-glass opacity or subtle reticulation in the posterobasal regions
- Problem: Mimics early pulmonary fibrosis (IPF/UIP pattern)
- Solution: Prone HRCT — dependent atelectasis resolves in prone position; true fibrosis persists
"HRCT is often performed in the prone position to prevent confusion with the increased opacification often seen in the dependent posterobasal segments in the usual supine position." — Grainger & Allison's Diagnostic Radiology
6.6 Ring Artifact (Detector Calibration Artifact)
- Cause: Faulty or miscalibrated CT detector element generating a fixed incorrect signal
- Appearance: Concentric ring or arc centered on the axis of rotation
- Solution: Regular detector calibration; detector replacement; software correction
6.7 Noise (Quantum Noise / Photon Starvation Noise)
- Cause: Insufficient photons reaching the detector → statistical variation in pixel values
- Appearance: Grainy, speckled appearance — especially marked with high-spatial-frequency (sharp) reconstruction kernels used in HRCT
- Effect: Can simulate fine reticulation or GGO; reduces confidence in subtle HRCT findings
- Trade-off: High-frequency kernel increases noise but is required for spatial resolution
- Management: Low-dose CT is feasible for lung parenchyma due to inherent high contrast between air and tissue (limiting the impact of quantum noise on diagnostic accuracy)
- Iterative reconstruction (IR) and AI-based reconstruction algorithms significantly reduce noise without sacrificing spatial resolution
6.8 Staircase / Windmill Artifact (Cone Beam Artifact)
- Cause: In MSCT with wide detector arrays (particularly 64+ rows), the cone-shaped x-ray beam creates reconstruction inconsistencies at the periphery of the detector
- Appearance: Staircase-like margins on coronal/sagittal reformats with step-like edges parallel to the scan plane
- Effect on HRCT: Degrades quality of sagittal/coronal reformatted images, particularly at lung bases
- Solution: Cone-beam correction algorithms; overlapping reconstruction
6.9 Pseudoenhancement Artifact
- Cause: Beam hardening in the presence of high-density contrast in adjacent structures creates spuriously elevated HU in areas of soft tissue or lung
- Effect: Can inflate nodule attenuation measurements; relevant in contrast-enhanced CT used for nodule evaluation
6.10 Summary of Artifacts Table
| Artifact | Cause | Appearance | Solution |
|---|---|---|---|
| Respiratory motion | Breathing during scan | Blurring, doubling of structures | Breath-hold; faster MSCT |
| Cardiac pulsation | Heart motion | Streaks/pseudo-GGO in left lower lobe | ECG gating; faster gantry |
| Beam hardening | Polychromatic x-ray beam | Dark bands between dense structures | Iterative reconstruction; DECT |
| Metal streak | Metallic implants | Radiating dark/bright streaks | MAR algorithms; increase kVp |
| Partial volume | Voxel averaging | Pseudo-nodules; missed fine detail | Thin collimation (1 mm) |
| Dependent atelectasis | Gravity + supine position | Posterior GGO mimicking fibrosis | Prone HRCT |
| Ring artifact | Detector malfunction | Concentric rings in image | Detector calibration |
| Quantum noise | Insufficient photons | Grainy texture | IR/AI reconstruction; optimise mAs |
| Staircase (cone beam) | Wide MSCT beam periphery | Staircase edges on reformats | Cone-beam correction |
7. Secondary Pulmonary Lobule — The Basis of HRCT Interpretation
HRCT interpretation is anchored on the anatomy of the secondary pulmonary lobule (SPL), which is visible on HRCT:
- Polyhedral unit, ~1–2 cm diameter
- Core: centrilobular artery + bronchiole
- Periphery: interlobular septa (contain pulmonary veins + lymphatics)
- Recognizing which compartment of the SPL is involved determines disease category:
- Perilymphatic (septa + subpleural): sarcoidosis, lymphangitic carcinomatosis
- Centrilobular: hypersensitivity pneumonitis, RB-ILD, smoking-related
- Random: haematogenous metastases, miliary TB
8. HRCT Findings — Broad Classification
| Category | Finding | Key Diseases |
|---|---|---|
| Increased opacity | Ground-glass opacity (GGO) | NSIP, AIP, pneumonia, oedema |
| Consolidation | Organising pneumonia, pneumonia | |
| Reticular / interstitial thickening | UIP/IPF, NSIP, lymphangitic spread | |
| Nodules (perilymphatic) | Sarcoidosis, silicosis | |
| Nodules (centrilobular) | HP, RB-ILD, endobronchial spread | |
| Nodules (random) | Miliary TB, haematogenous mets | |
| Decreased opacity | Emphysema (centrilobular) | Smoking, COPD |
| Emphysema (panlobular) | α1-antitrypsin deficiency | |
| Cysts | LAM, BHD, LIP | |
| Honeycombing | UIP/IPF (diagnostic feature) | |
| Air trapping | Small airway disease, BOS, asthma | |
| Mosaic attenuation | Small airway disease, vascular occlusion |
Sources:
- Murray & Nadel's Textbook of Respiratory Medicine
- Grainger & Allison's Diagnostic Radiology
- Fishman's Pulmonary Diseases and Disorders
- Washington Manual of Medical Therapeutics
- Sabiston Textbook of Surgery
Patient radiation dose consideration in helical ct in detail
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
I now have comprehensive textbook data from all major sources. Let me compose the full, detailed answer.
Patient Radiation Dose Considerations in Helical CT — Comprehensive Guide
1. Why Radiation Dose Matters in Helical CT
CT represents approximately 10% of all studies using ionising radiation, yet is responsible for approximately two-thirds of the collective radiation dose to the population from medical imaging. The rise of helical/spiral and multislice CT has dramatically increased scan speed and quality — but also the volume of patients scanned. This makes understanding, measuring, and minimising CT radiation dose a critical responsibility of every radiologist.
"CT examinations represent approximately 10% of all studies that use ionising radiation, yet they are responsible for two-thirds of the radiation dose." — Grainger & Allison's Diagnostic Radiology
Every human is exposed to approximately 3 mSv/year of background radiation from natural and man-made sources.
| Examination | Approximate Effective Dose |
|---|---|
| Chest X-ray | 0.1–0.2 mSv |
| CT chest (standard protocol) | 5–20 mSv |
| CT abdomen/pelvis | 10–20 mSv |
| Low-dose CT chest (screening) | ≤3 mGy (CTDIvol) / ~0.9–1.5 mSv |
| CT urinary stone (low dose) | 0.5–0.7 mSv |
| CT urinary stone (standard) | ~3.63 mSv |
| PET-CT | ~25 mSv |
| Whole-body CT | ~3× average background radiation |
2. Radiation Dose Terminology — Definitions
2.1 Absorbed Dose
- Definition: Energy absorbed per unit mass of a specific organ
- Unit: Gray (Gy) (= Joules/kg)
- Accounts for malignancy risk at the irradiated organ site
- Represents the actual physical energy deposition
2.2 Effective Dose
- Definition: An overall estimate of total-body radiation exposure — the dose that, if delivered uniformly to the whole body, would yield the same biological consequences (specifically cancer induction) as the actual organ-specific doses
- Unit: Sievert (Sv) or millisievert (mSv)
- Calculated by: summing individual absorbed doses to each organ × tissue weighting factor (Wt) for that organ's radiosensitivity
- Useful for gross comparisons between modalities and techniques
⚠️ Critical point: Effective dose is NOT a measure of the actual radiation imparted to an individual patient during CT. The actual patient dose depends on patient size, shape, and body composition — not just scanner output. It must not be used to estimate individual cancer risk.
2.3 CT Dose Index (CTDI)
- The primary scanner output metric for CT
- Represents the absorbed dose averaged over a standard phantom (16 cm diameter for head; 32 cm for body)
- Expressed as CTDIvol (volumetric CTDI) in mGy (milligray) — the most commonly quoted
- CTDIvol ≠ patient dose — it is a measure of scanner radiation output, not what the patient actually receives
2.4 Dose-Length Product (DLP)
- DLP = CTDIvol × scan length (cm)
- Unit: mGy·cm
- Reflects total radiation output for the entire scan
- Can be converted to an approximate effective dose in mSv using conversion factors (k-factors, in mSv/mGy·cm) that vary by body region
- Lung cancer screening mandate: CTDIvol ≤ 3 mGy
"The CT dose index (expressed as CTDIvol) and the dose-length product are measures of scanner radiation output, not patient dose. These parameters should not be used to estimate potential cancer risk for individual patients." — Murray & Nadel's Textbook of Respiratory Medicine
2.5 Size-Specific Dose Estimate (SSDE)
- Corrects CTDIvol for patient size using conversion factors based on measured body diameter from the CT scout image
- More representative of actual patient dose than CTDIvol alone
- Used in paediatric dosimetry
3. Biological Effects of Radiation — Stochastic vs. Deterministic
3.1 Deterministic Effects (Tissue Reactions)
- Threshold-dependent — occur only above a specific dose; severity worsens with increasing dose above threshold
- Examples: skin erythema, cataract, bone marrow suppression, radiation sickness
- Threshold for deterministic effects: > 2,000 mSv (2 Sv) of acute exposure
- Rarely occur from diagnostic CT — essentially no concern in standard CT protocols
- Of historical relevance to fluoroscopy and cardiac catheterisation, not routine CT
3.2 Stochastic Effects
- No threshold — probability of occurrence increases with dose, but severity does not
- Carcinogenesis is the primary stochastic effect of diagnostic CT
- May occur years to decades after exposure
- Cannot be distinguished from spontaneous cancer
- Risk increases with:
- Younger age (more dividing cells, longer life expectancy)
- Female sex
- Higher cumulative dose
- Repeated imaging over a lifetime
"Carcinogenesis is a proven stochastic effect. A stochastic effect occurs randomly and no lower threshold of ionising radiation exposure exists where cancer induction does not occur." — Grainger & Allison's Diagnostic Radiology
3.3 ICRP Risk Estimate
- The International Commission on Radiological Protection (ICRP) estimates the risk coefficient as:
- ~0.00005 per mSv = 5% per 1,000 mSv = 1 additional cancer per 20,000 mSv total population dose
- For a standard chest CT (~10 mSv): attributable risk ≈ 0.05% (1 in 2,000)
3.4 The Linear No-Threshold (LNT) Model
- LNT hypothesis: A linear, proportional relationship between radiation dose and cancer risk exists, with no safe threshold dose
- Used to establish radiation protection standards
- Controversy: Most evidence for carcinogenesis comes from exposures >100 mSv (atomic bomb survivors); extrapolation to CT dose levels (5–20 mSv) using LNT is disputed
- Critics argue LNT overestimates risk at low diagnostic radiation doses
- The ICRP and NCRP (National Council on Radiation Protection and Measurements) advise against projecting individual cancer risk from medical imaging using LNT
- Key principle: Radiation exposures from separate imaging examinations are not cumulative — each adds its own incremental risk independently
"Radiation is a relatively weak carcinogen, and excess radiogenic cancer risk, if any, is considerably less than spontaneous cancer risk." — Murray & Nadel's Textbook of Respiratory Medicine
4. CT Parameters That Affect Radiation Dose in Helical CT
4.1 Tube Current (mA) and mAs
- Most practical dose-reduction parameter
- Dose is directly proportional to mAs (milliampere-seconds = mA × rotation time)
- 50% reduction in mA → 50% reduction in dose
- Low-dose chest CT: 40–70 mAs is sufficient due to inherent high contrast between air and lung tissue
- Trade-off: lower mAs → increased image noise (quantum noise)
- Effective mAs = mAs/pitch (used on some MSCT systems to maintain constant dose regardless of pitch)
4.2 Tube Voltage (kVp)
- Determines x-ray beam energy
- Dose ∝ kVp² (approximately) — a small reduction in kVp yields a disproportionately large dose reduction
- Standard chest CT: 120 kVp
- Thin/small patients (<50 kg) and paediatrics: 100 kVp recommended
- 80 kVp is associated with unacceptable beam hardening, even in small patients
- Some modern scanners automatically suggest optimal kVp from the scout radiograph
4.3 Pitch
- Pitch = table distance travelled per rotation ÷ total beam collimation width
- In single-slice helical CT: Dose ∝ 1/pitch — higher pitch = faster scanning = lower dose
- In MSCT with effective mAs setting: dose is maintained constant regardless of pitch (automatic tube current compensates)
- Caution: dose strategies from single-slice systems cannot be extrapolated to MSCT systems
4.4 Scan Length / Coverage
- Dose ∝ scan length — longer coverage = higher DLP
- Dose reduction strategy: restrict scan range to only the anatomically relevant region
- Avoid unnecessary extension beyond the area of clinical interest
4.5 Collimation and Slice Thickness
- Narrower collimation (thin sections) → each section receives more radiation for equivalent image quality
- MSCT allows retrospective reconstruction of thin-section data — thin sections acquired once, reconstructed at any desired thickness, eliminating repeat scanning
- Wider sections (3–5 mm) used for routine display; thin sections (1 mm) available for HRCT review without additional radiation
4.6 Gantry Rotation Time
- Shorter rotation time → faster scan → less time per slice → reduced dose per unit length
- Modern systems: rotation times as fast as 0.33 seconds/rotation
- Particularly relevant in cardiac and paediatric imaging (also reduces motion artefact)
4.7 Geometric Efficiency (MSCT-specific)
- In 4–16 row MSCT: overbeaming (extra-focal radiation beyond the active detector width) reduces efficiency → increases dose
- 64-channel MSCT: beam width remains constant → geometric efficiency is high with minimal dose penalty
- Detector gaps (non-sensing inter-element spaces): photons hitting gaps are wasted dose; more gaps with more rows
4.8 Over-ranging (z-overscanning)
- In helical CT: the scanner must start and stop the spiral before and after the prescribed scan range to allow adequate data interpolation at the edges
- This results in irradiating tissue beyond the intended scan range at the start and end of acquisition — called over-ranging or z-overscanning
- More pronounced with:
- Higher pitch
- Wider detector collimation (wider beam = more over-ranging)
- Particularly significant in short scan ranges (paediatric imaging, limited coverage)
- Solution: Modern CT systems use dynamic collimators (flying z-collimators) at the start and end of helical acquisitions to block the excess radiation and reduce dose
5. Dose Reduction Strategies in Helical CT
5.1 Automatic Tube Current Modulation (ATCM) / Automatic Exposure Control (AEC)
The most impactful hardware dose-reduction innovation:
| Type | Mechanism | Effect |
|---|---|---|
| Patient-size AEC | Tube current selected based on patient size from scout | Appropriate mA for body habitus |
| z-axis AEC | Tube current adjusted in real-time along the scan length to maintain target noise | Higher mA at shoulders; lower at lung apices |
| Angular (x-y) AEC | Tube current adjusted per gantry rotation angle | Reduces mA in projections with less diagnostic importance |
| Combined | Most modern systems use all three | Mean dose reduction of 30% reported in children |
Key benefits:
- Thicker body regions (abdomen) receive higher mA; thinner regions (pelvis) receive less
- Mean tube current-time product reduced by average 32% while maintaining image quality
- Dose reductions achieved in almost 90% of examinations
Limitation in paediatrics: Children are rounder in cross-section → angular ATCM has limited effectiveness (less variation between AP and lateral projections)
"Automatic tube current modulation tailors the output of the CT tube to the patient's size and shape based on the patient's diameter and x-ray attenuation. Early clinical trials demonstrated dose reductions in almost 90% of examinations with a 32% reduction in tube current time product." — Grainger & Allison's Diagnostic Radiology
5.2 Iterative Reconstruction (IR)
Traditional CT image reconstruction used Filtered Back Projection (FBP) — computationally simple but amplifies noise at low doses.
Iterative Reconstruction (IR) works by:
- Generating an initial estimated image from acquired projection data
- Comparing the estimated projections with actual measured projections
- Iteratively updating the image estimate to minimise the difference
- Incorporating statistical models of photon noise and system physics
| IR Generation | Method | Dose Reduction |
|---|---|---|
| Hybrid IR | Combines IR with FBP | ~30–50% vs FBP |
| Statistical IR | Full statistical model of noise | ~50–60% |
| Model-based IR (MBIR) | Full physics model + statistical model | Up to 75% or greater |
- IR substantially reduces noise at equivalent or lower doses → diagnostically comparable images from low-dose acquisitions
- CT lung cancer screening uses MBIR with CTDIvol ≤ 3 mGy
- Noise reduction of ~50% (in standard deviation) demonstrated with model-based IR vs FBP
"The widespread dissemination of technologies such as iterative reconstruction is likely to result in CT dose reductions on the order of 75% and greater in future years." — Grainger & Allison's Diagnostic Radiology
5.3 Low-Dose CT Protocols
- Chest LDCT (lung cancer screening): CTDIvol ≤ 3 mGy mandated (CMS requirement)
- Tube current-time products as low as 20 mAs still provide acceptable pulmonary nodule detection
- Feasible due to high inherent air-tissue contrast in the lungs limiting the effect of quantum noise
- Low-dose CT for urinary stones: effective dose 0.5–0.7 mSv (vs ~3.63 mSv standard dose)
5.4 Tube Voltage Reduction
- Reducing kVp from 120 to 100 kVp → significant dose reduction
- Appropriate for: thin patients (<50 kg), paediatrics, CT angiography (higher contrast at lower kVp)
- Modern scanners automatically suggest optimal kVp from the scout view
5.5 Beam-Shaping Filters (Bowtie Filters)
- X-ray beam intensity is shaped by a bowtie-shaped filter — thicker at the edges, thinner in the centre
- Reduces peripheral over-irradiation (patient periphery receives lower dose)
- Reduces dose and improves image uniformity
- Different bowtie filter sizes used for head vs. body vs. paediatric imaging
5.6 Bismuth Shielding and Organ-Based Tube Current Modulation
- Bismuth shields placed over radiosensitive organs (thyroid, eye lens, breast)
- Limitation: increases scatter, which can increase tube current if ATCM is active → partially counterproductive
- Organ-based modulation (integrated into ATCM): reduces x-ray output when tube is in the AP position (over anterior structures — breast, thyroid) → eliminates need for bismuth shielding while achieving same benefit
5.7 Dynamic Collimators (Z-Collimation) for Over-Ranging
- Deployed at the start and end of helical acquisition
- Gradually open/close to block radiation during the over-ranging portion
- Reduces dose from z-overscanning, particularly important in short or paediatric scan ranges
5.8 Summary Table: Dose Reduction Strategies
| Strategy | Mechanism | Dose Reduction | Trade-off |
|---|---|---|---|
| ↓ mAs (tube current) | Less photon flux | Direct (50% mAs = 50% dose) | ↑ Noise |
| ↓ kVp | Lower beam energy | Disproportionate dose reduction | ↑ Noise, beam hardening risk |
| ↑ Pitch (helical) | Faster table movement | Linear with pitch | May affect z-resolution |
| ATCM (z-axis + angular) | Real-time mA adaptation | ~30–50% | Minimal |
| Iterative reconstruction | Statistical noise modelling | Up to 75% | Longer processing time |
| Model-based IR (MBIR) | Full physics + stats model | >75% | Computationally intensive |
| Restrict scan length | Shorter z-coverage | Proportional to length saved | Clinical information may be missed |
| Bowtie filter | Peripheral beam shaping | 20–50% peripheral dose | Standard feature |
| Dynamic z-collimators | Block over-ranging | Significant for short ranges | Hardware dependent |
| Organ-based modulation | ↓ mA in AP position | Thyroid/breast dose ↓ | ATCM integration required |
| 100 kVp (thin patients) | Lower photon energy | Substantial | Not for all body types |
6. Special Populations at High Radiation Risk
6.1 Paediatric Patients
- Young, rapidly dividing cells are more radiosensitive
- Longer life expectancy → longer time for radiation-induced cancers to develop
- Dose-response relationship between CT radiation and brain cancer in children
- ALARA (As Low As Reasonably Achievable) principle is mandatory
- Campaigns: ImageGently (paediatric), ImageWisely (adult)
- Paediatric-specific strategies: weight-based mAs, 100 kVp, smallest FOV, limited scan range, minimal phase acquisitions, avoid pan-scan
6.2 Patients with Chronic Diseases (High Cumulative Dose Groups)
At-risk groups from repeated CT exposure:
| Patient Group | Reason |
|---|---|
| Crohn's disease | Repeated flares and post-surgical follow-up |
| Cystic fibrosis | Lifelong respiratory monitoring |
| Testicular cancer survivors | Curable malignancy requiring long-term follow-up |
| Hodgkin's lymphoma | Young patients, curable but repeated staging |
| Renal colic / urolithiasis | Recurrent presentations requiring CT each time |
- Dose registries are emerging to track cumulative lifetime radiation doses per patient
- However, the LNT model and ICRP state that separate CT exposures are not additive in cancer risk prediction — each adds only its own incremental risk
6.3 Pregnancy
- Fetal dose: primary concern
- CT chest for PE: fetal radiation dose is negligible at any stage of pregnancy
- Abdominal/pelvic CT: significantly higher fetal dose → indicate only when clearly necessary
- Consider MRI as alternative for non-thoracic indications
6.4 Women
- Risk of radiation-induced malignancy is relatively higher in women compared with men
- Breast tissue (anterior chest wall) is radiosensitive → organ-based tube modulation and bowtie filters are important
7. Low-Dose CT for Lung Cancer Screening — Dose Standards
- National Lung Screening Trial (NLST) established CT screening for lung cancer
- Mandatory requirement: CTDIvol ≤ 3 mGy
- Effective dose: approximately 0.9–1.5 mSv with MBIR reconstruction
- Low-dose feasible because: inherently high contrast between air and soft tissue in lungs limits noise impact
- As few as 20 mAs still adequate for nodule detection
8. Justification, Referral, and the "3As" Framework
Effective radiation protection operates on three levels:
8.1 Justification
- Every CT scan must be clinically justified — expected benefit must outweigh radiation risk
- Radiologists must refuse or modify unjustified requests
8.2 Optimisation (ALARA)
- Achieve the diagnostic objective with the lowest reasonably achievable dose
- Uses all technical strategies listed above
- Radiographers/technologists must be trained in dose optimisation as active participants
8.3 Dose Limitation
- Applicable to occupational workers and the general public, not individual patients (where justification and optimisation govern)
- Diagnostic reference levels (DRLs) set by national/international bodies define typical dose values for standard examinations — institutions should not routinely exceed them
8.4 Clinical Practice Framework
"Our responsibility is to first counsel patients accurately regarding the risks of ionising radiation exposure; second, to limit the use of CT to clinical situations where they are likely to change management; and third, to ensure a diagnostic quality examination is acquired with the lowest possible radiation exposure whenever an ionising radiation investigation is deemed necessary." — Grainger & Allison's Diagnostic Radiology
Five Ways to Reduce Radiation Exposure in Practice:
- Ensure proper clinical indication before ordering CT
- Consider non-ionising alternatives (ultrasound, MRI) when equivalent
- Use low-dose protocols: ATCM, iterative reconstruction, reduced kVp/mAs
- Track cumulative dose in patients with chronic conditions (Crohn's, CF, urolithiasis)
- Adhere to international radiation monitoring guidelines (ICRP, NCRP, ACR, AAPM)
9. Specific Helical CT Dose Considerations by Region
| Region | Standard Dose | Key Consideration |
|---|---|---|
| Chest (helical HRCT) | ~5–10 mSv | Low-dose feasible (high air-tissue contrast) |
| Chest (PE protocol - CTA) | ~10–15 mSv | Narrower sections → relatively higher dose per unit length |
| Abdomen/pelvis | ~10–20 mSv | Multi-phase protocols increase total dose; minimize phases |
| Head | ~2–5 mSv | ECG gating not needed; sequential mode reduces dose vs helical |
| Paediatric chest | <2 mSv (target) | Weight-based mAs; 100 kVp; ALARA strictly applied |
| Lung cancer screening | ≤1.5 mSv | CTDIvol ≤ 3 mGy; MBIR mandatory |
10. Key Summary Points for Exam
| Concept | Key Fact |
|---|---|
| Primary dose metric from scanner | CTDIvol (mGy) — NOT patient dose |
| Total scan output | DLP = CTDIvol × scan length (mGy·cm) |
| Most practical dose reduction | ↓ mAs (50% reduction → 50% dose reduction) |
| Stochastic effect | Cancer; no threshold; probability ∝ dose |
| Deterministic effect | Threshold >2,000 mSv; virtually never from diagnostic CT |
| LNT model | Linear, no-threshold; debated for diagnostic CT doses |
| ICRP risk estimate | ~0.00005 per mSv (5% per 1,000 mSv) |
| Background radiation | ~3 mSv/year |
| Chest CT | 5–20 mSv effective dose |
| LDCT screening | ≤3 mGy CTDIvol; ~0.9–1.5 mSv effective dose |
| Best dose reduction technology | Model-based iterative reconstruction (MBIR) — up to 75%+ dose reduction |
| Over-ranging in helical CT | Extra-boundary irradiation at scan start/end; prevented by dynamic z-collimators |
| Geometric efficiency problem | Detector element gaps; wasted photons; more gaps with more rows |
| High-risk populations | Children, women, chronic disease patients (Crohn's, CF), pregnancy |
| ALARA | "As Low As Reasonably Achievable" — mandatory for paediatrics, universal best practice |
Sources:
- Murray & Nadel's Textbook of Respiratory Medicine (dedicated Radiation Exposure and Cancer Risk section)
- Grainger & Allison's Diagnostic Radiology (CT Dose Considerations, Iterative Reconstruction, ATCM sections)
- Fishman's Pulmonary Diseases and Disorders (stochastic/deterministic effects, ICRP estimates)
- Sabiston Textbook of Surgery (paediatric radiation considerations)
This is a shared conversation. Sign in to Orris to start your own chat.