Disscus endometrial biopsy in health and disease
Reading File
Finding Sources
Finding Sources
Searching PubMed
"endometrial biopsy" AND "endometrial cancer"
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Finding Sources
I now have comprehensive information from multiple authoritative textbooks. Let me compile the full response.
Endometrial Biopsy: In Health and Disease
1. Overview and Clinical Significance
Endometrial biopsy (EMB) is an office-based procedure that samples the uterine lining to evaluate abnormal uterine bleeding, screen for endometrial pathology, and confirm normal cyclical endometrial function. Office aspiration biopsy is the accepted first step in evaluating a patient with abnormal uterine bleeding or suspected endometrial pathology, with a diagnostic accuracy of 90-98% compared with findings at dilation and curettage (D&C) or hysterectomy. - Berek & Novak's Gynecology, p. 2152
2. Indications
Diagnostic Indications
EMB should be considered in:
- Women with suspected endometrial pathology
- All women >45 years with abnormal uterine bleeding in whom medical treatment has been unsuccessful
- Women with persistent intermenstrual bleeding
- Postmenopausal women with endometrial thickness >4 mm on transvaginal ultrasound (TVUS), or any postmenopausal vaginal bleeding
- Premenopausal women with endometrial thickness >7 mm in known polycystic ovarian syndrome (PCOS)
- Irregular or unscheduled bleeding on hormone replacement therapy (HRT) after the first 3 months
- Younger women with major risk factors for endometrial hyperplasia/cancer
- Bailey and Love's Short Practice of Surgery, 28th Ed., p. 1602
Risk Factors Prompting Biopsy (Box 143-1)
| Risk Factor | Comment |
|---|---|
| Age >50 years | Post-menopausal state |
| Obesity | 21-50 lbs overweight = 3x less risk than >50 lbs overweight |
| Atypical endometrial hyperplasia | Premalignant |
| Chronic anovulation / PCOS | Unopposed estrogen |
| Nulliparity | Prolonged estrogen exposure |
| Diabetes | Insulin resistance / obesity link |
| Tamoxifen therapy | Estrogen agonist effect on endometrium |
| Unopposed estrogen therapy | No progestogen |
| Menopause after age 55 | Prolonged estrogen exposure |
| Family history of HNPCC / Lynch syndrome | Up to 60% lifetime risk of endometrial cancer; screen annually from age 35 with TVUS and EMB |
- Pfenninger and Fowler's Procedures for Primary Care, 3rd Ed., p. 996
Lynch Syndrome / HNPCC - Special Population
Unlike sporadic endometrial cancers (typically diagnosed in the 6th-7th decade), Lynch syndrome-associated endometrial cancer presents in the 5th decade. International guidelines recommend annual screening from age 35 with transvaginal ultrasound and endometrial biopsy. - Bailey and Love's, p. 1604
3. Contraindications
Absolute
- Pregnancy
- Bleeding diathesis / coagulopathy
Relative
- Use of anticoagulant therapy
- Active vaginal, cervical, uterine, or pelvic infection
- Cervical stenosis
- Morbid obesity
- Significant pelvic relaxation / uterine prolapse
- Pfenninger and Fowler's, p. 995
4. Equipment
A variety of instruments are available. Commonly used options include:
- Disposable flexible plastic aspirator (Pipelle, Piper Curet, Endocell) - most commonly used; narrow cannulas cause less cramping, are inexpensive, and obtain adequate samples in >95% of cases
- Reusable stainless steel curettes (Novak or Randall) with 20-mL syringe
- Disposable aspirators with syringe suction (Cannula Curette, Uterine Explora)
- Tao Brush - a brush sampler within a protective sheath that allows endometrium-only sampling without vaginal/cervical contamination; used with liquid-based cytology
- Vabra aspirator with external suction pump
Common equipment needed regardless of method: large Graves vaginal speculum, povidone-iodine, ring forceps, uterine sound, single-tooth tenaculum, Kevorkian endocervical curette (without basket), buffered formalin specimen containers.
- Pfenninger and Fowler's, pp. 995-997
5. Pre-procedure Preparation
- Review recent Pap smear; obtain one before EMB if indicated
- Perform bimanual examination to assess uterine size, position, and any significant anteversion/retroflexion (increases perforation risk)
- Pain management: NSAID premedication (ibuprofen 600-800 mg orally 30-60 minutes before) effectively decreases uterine cramping
- Anxious patients may be premedicated with oral diazepam 10 mg 1 hour before
- Antibiotic prophylaxis is NOT recommended by the American Heart Association (unlikely to cause bacteremia)
- Timing in reproductive-age women: Optimally performed on day 22-23 of the cycle - secretory glands confirm ovulation has occurred; avoid biopsy during menses (stromal breakdown can mimic malignancy)
- Confirm the patient is not pregnant before beginning
- Pfenninger and Fowler's, pp. 995-996
6. Procedure Steps
- Place patient in dorsal lithotomy position; perform bimanual examination
- Insert large Graves speculum; visualize cervix; clean any mucus/debris
- Change to sterile gloves
- Prepare cervix and vagina with povidone-iodine
- Perform endocervical curettage if neoplasm is suspected (Kevorkian curette inserted 2-3 cm into endocervical canal and scraped outward)
- Apply tenaculum to anterior cervical lip if needed to stabilize and straighten the uterine axis
- Insert uterine sound to determine depth (normal: up to 10 cm); if stenosis is present, dilate with small cervical dilators
- Insert the chosen aspirator/cannula to fundal depth; create suction (withdraw inner plunger or apply syringe suction); rotate 360° and move in and out along the uterine cavity 3-4 times
- Remove instrument; expel tissue into formalin (or CytoRich Red for Tao Brush)
- Remove speculum
Cervical Stenosis Management
A paracervical block can be performed and cervix gradually dilated. Premedication with antiprostaglandin agents reduces cramping. - Berek & Novak's, p. 2152
7. Interpretation of Results
When submitting EMB, the pathologist requires: patient's age, clinical indication, menopausal status, and date/length of last menstrual period. Interpretation is based on the functionalis layer (upper two-thirds of endometrium); the basalis layer shows minimal cyclical change.
Normal Biopsy Findings
| Result | Significance |
|---|---|
| Proliferative endometrium | Normal; follicular phase |
| Secretory endometrium | Confirms ovulation has occurred |
| Atrophic endometrium | Normal postmenopausal state |
Pregnancy-Related Findings
- Retained products of conception
- Decidua - suggests ectopic or missed abortion
Infectious Etiology
- Endometritis - treat as indicated (plasma cell infiltrate on histology is diagnostic)
Inadequate Samples
May occur with: biopsy immediately after menses, hypoestrogenism, prolonged bleeding, intrauterine adhesions (Asherman syndrome), atrophic endometrium. Menopausal status has a greater effect on specimen adequacy than the type of instrument used.
8. Endometrial Hyperplasia: Classification and Cancer Risk
Hyperplasia reflects a chronic unopposed hyperestrogenic state (relative absence of progesterone), characterized by proliferation of endometrial glands and an increased gland-to-stroma ratio.
WHO/International Society of Gynecological Pathologists Classification
| Type of Hyperplasia | Risk of Progression to Cancer |
|---|---|
| Simple (cystic, without atypia) | ~1% |
| Complex (adenomatous, without atypia) | ~3% |
| Simple with atypia | ~8% |
| Complex with atypia | ~29% |
From the landmark study by Kurman et al. (Cancer 1985), following 170 untreated patients for a mean of 13.4 years; 74% regressed, 18% remained stable. - Berek & Novak's Gynecology, p. 2145
Importantly, 25-43% of patients with atypical hyperplasia detected on biopsy will have concurrent, usually well-differentiated endometrial carcinoma at hysterectomy. A more modern prospective study noted that 42.5% of complex atypical hyperplasia cases on biopsy had cancer at the time of hysterectomy. - Schwartz's Principles of Surgery, 11th Ed., p. 1823
2014 WHO Binary Classification (EIN System)
The WHO 2014 classification replaced the older 4-tier system with a binary system:
- Hyperplasia without atypia - may be managed conservatively with hormonal therapy
- Endometrial Intraepithelial Neoplasia (EIN) - considered a premalignant lesion; emphasis on glandular crowding/complexity, not just cytologic atypia; a D-score <1 (accounting for % stroma, glandular complexity, gland pleomorphism) connotes high progression risk
Important distinction: EIN differs from Endometrial Intraepithelial Carcinoma (EIC), which is a precursor of serous endometrial cancer and always requires hysterectomy with surgical staging. - Schwartz's, pp. 1823-1824
9. Management After Biopsy
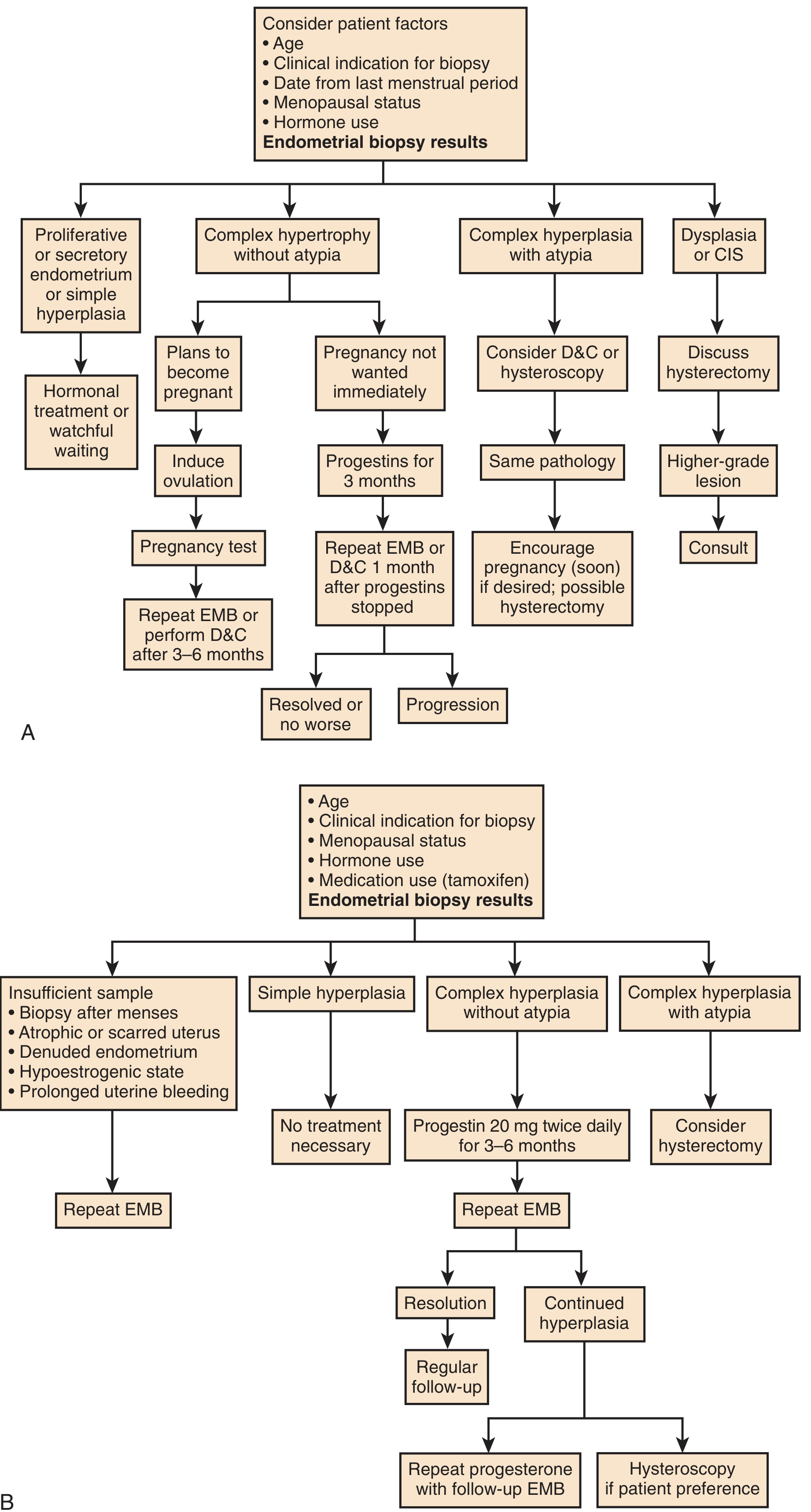
Figure: Management options after EMB. (Pfenninger and Fowler's Procedures for Primary Care, 3rd Ed., p. 1001)
By Biopsy Result
Proliferative/Secretory/Simple hyperplasia: Hormonal treatment or watchful waiting.
Complex hyperplasia without atypia:
- Progestins (medroxyprogesterone acetate 20 mg twice daily) for 3-6 months
- Repeat EMB after therapy; complete reversal is often noted
- If hyperplasia persists: repeat progestin course with follow-up EMB or hysteroscopy
- Some patients may opt for hysterectomy at this point
Complex hyperplasia with atypia:
- Hysterectomy is the preferred treatment due to 29% risk of cancer progression and 25-43% risk of concurrent carcinoma
- If fertility preservation desired: high-dose progestins (megestrol acetate 40-160 mg/day or progesterone IUD) with close follow-up and repeated sampling; progestins achieve 76% overall response rate with median regression at 12 weeks, but 24% recurrence rate
- If pregnancy not desired immediately: progestins for 3 months, then repeat EMB
Adenocarcinoma: Referral for appropriate staging and treatment (hysterectomy with bilateral salpingo-oophorectomy and lymph node assessment).
Insufficient sample: Repeat EMB; if still inadequate, proceed to hysteroscopy and D&C. - Pfenninger and Fowler's, pp. 1000-1001
10. Hysteroscopy and D&C vs. EMB
| Feature | Office EMB (Pipelle) | Hysteroscopy + D&C |
|---|---|---|
| Setting | Office/clinic | Operating room |
| Accuracy | 90-98% overall | Higher for focal lesions |
| Polyps/submucous myomas | Missed more often | Superior detection |
| Patient tolerance | Better | Requires anesthesia |
| Cost | Lower | Higher |
Hysteroscopy and D&C should be reserved for:
- Cervical stenosis preventing adequate aspiration biopsy
- Bleeding recurs after a negative EMB
- Inadequate specimen on EMB
- Suspicion of focal pathology (polyps, submucous fibroids)
Hysteroscopy is more accurate than EMB or D&C alone for identifying polyps and submucous myomas. - Berek & Novak's, p. 2152
11. Hysteroscopic View of Endometrial Cancer
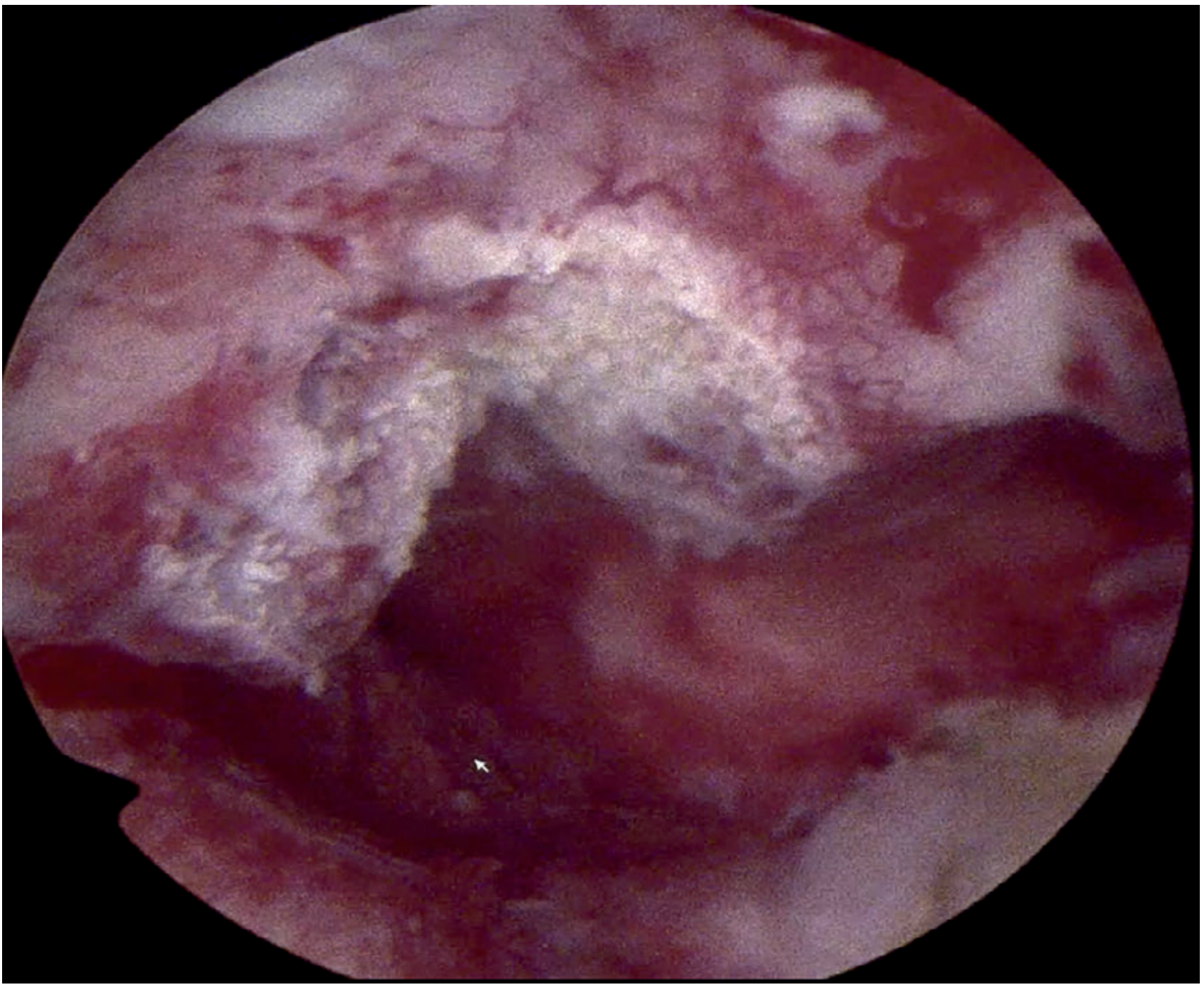
Figure 87.18: Hysteroscopic biopsy of endometrial cancer (cystic endometrium visible). - Bailey and Love's Short Practice of Surgery, 28th Ed.
12. Complications
| Complication | Incidence | Management |
|---|---|---|
| Uterine perforation | 0.1-1.3% | Stop procedure; observe; repeat biopsy in 6-8 weeks if stable |
| Vasovagal reaction | Variable | Position change; reassurance |
| Infection / endometritis | Rare | Antibiotics |
| Cervical laceration (from tenaculum) | Uncommon | Direct pressure |
| Bleeding | Rare | Usually self-limited |
Perforation most commonly occurs with rigid devices, during uterine sounding, or with cervical stenosis. If the sound passes >12 cm without expected resistance, suspect perforation. - Pfenninger and Fowler's, p. 1000
13. Role of Transvaginal Ultrasound (TVUS) Alongside EMB
TVUS is a useful adjunct but NOT a substitute for histologic assessment in symptomatic women:
-
Endometrial thickness <4 mm in postmenopausal women: may not need EMB in the absence of additional bleeding episodes
-
Thickness >4 mm (postmenopausal) or polypoid mass or intracavitary fluid: requires further evaluation including EMB
-
Sonohysterography (saline infusion) helps distinguish between atrophic endometrium and significant endometrial tissue or polyps
-
The finding of an endometrial thickness <5 mm in postmenopausal women is consistent with atrophy, but TVUS cannot alone eliminate the need for biopsy in symptomatic patients
-
Washington Manual of Medical Therapeutics, Berek & Novak's
14. EMB in Specific Clinical Scenarios
Abnormal Uterine Bleeding (AUB)
EMB is the cornerstone of evaluating AUB, especially in women ≥45 years. In premenopausal women with obesity, chronic anovulation, or persistent/recurrent bleeding, endometrial cancer must be excluded. The amount of bleeding does not correlate with severity of pathology - histology must be obtained. - Schwartz's, Tintinalli's Emergency Medicine
Tamoxifen Therapy
Tamoxifen users require EMB evaluation for irregular or unscheduled bleeding, as tamoxifen acts as an estrogen agonist on the endometrium, increasing risk of hyperplasia and cancer. - Bailey and Love's
Endometrial Biopsy for Luteal Phase Defect
Previously used to confirm ovulation and assess luteal adequacy by dating secretory endometrium - now considered a test of unproven utility and no longer recommended for this indication. - Berek & Novak's, p. 1483
Summary
Endometrial biopsy is a safe, accurate, and cost-effective office procedure. Its primary roles are:
- Evaluate abnormal uterine bleeding at any age, particularly ≥45 years
- Screen high-risk populations (Lynch syndrome, chronic anovulation, tamoxifen users)
- Classify endometrial hyperplasia to guide management (from watchful waiting/progestins to hysterectomy)
- Diagnose endometrial cancer with 90-98% accuracy, enabling prompt referral
- Monitor treatment response after progestin therapy in hyperplasia
Histopathology always determines management - clinical features, bleeding patterns, and ultrasound measurements alone are never sufficient substitutes for tissue diagnosis in symptomatic women.
Sources: Pfenninger and Fowler's Procedures for Primary Care (3rd Ed.); Berek & Novak's Gynecology; Bailey and Love's Short Practice of Surgery (28th Ed.); Schwartz's Principles of Surgery (11th Ed.); Washington Manual of Medical Therapeutics.
This is a shared conversation. Sign in to Orris to start your own chat.