Types of dental abscess
Reading File
Finding Sources
Finding Sources
Searching the Web
types of dental abscess periapical periodontal classification
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Searching Images
types of dental abscess periapical periodontal gingival diagram
Loading Image
Types of Dental Abscess
A dental abscess is a localized collection of pus resulting from bacterial infection of the teeth or supporting structures. There are three primary types, distinguished by anatomical location and origin.
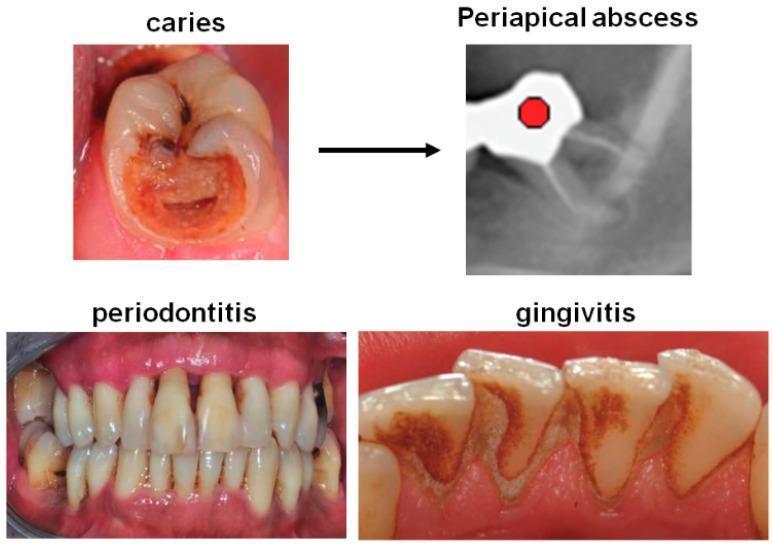
1. Periapical Abscess (= Dentoalveolar Abscess)
Most common type.
| Feature | Detail |
|---|---|
| Origin | Pulpal infection (dental caries → pulpitis → pulpal necrosis) |
| Location | Apex (tip) of the tooth root, within the periapical area of the periodontal ligament |
| Pathogenesis | Caries breaches enamel → infects pulp → irreversible pulpitis → pulpal necrosis → infection travels down root canals into periapical tissues |
Pathological forms at the periapex:
- Acute periapical abscess — acute suppurative inflammation with pus
- Periapical granuloma — chronic non-suppurating inflammation (chronic form)
- Radicular (periapical) cyst — formed when epithelial rests in the periodontal ligament are stimulated within the chronic granuloma
Clinical features:
- Tooth tender to percussion
- Swelling of adjacent gingiva; may develop a parulis (gum boil) — a small swelling with a draining fistula adjacent to the affected tooth
- If pus erodes through cortical bone without draining spontaneously → subperiosteal extension with intraoral or facial swelling/fluctuance
Radiology:
- Periapical radiograph shows periapical radiolucency (widening of periodontal ligament space, thinning of lamina dura, radiolucent area at root apex)
Treatment:
- Root canal therapy or dental extraction (definitive)
- Incision and drainage if fluctuant
- Antibiotics (amoxicillin first-line)
- NSAIDs ± acetaminophen for pain
2. Periodontal Abscess
Second most common type.
| Feature | Detail |
|---|---|
| Origin | Pre-existing periodontal (gum) disease — plaque/debris entrapped in a periodontal pocket |
| Location | In the supporting tissues (periodontal pocket, alveolar bone, periodontal ligament) — lateral to the root, not at the apex |
| Pathogenesis | Chronic periodontal disease → organisms trapped in the periodontal pocket → purulent material may escape via gingival sulcus or invade supporting alveolar bone and periodontal ligament |
Clinical features:
- Localized, painful, fluctuant swelling along the lateral surface of the root
- May have pus draining from the gingival sulcus
- Deep periodontal pocketing on probing
- Tooth may be vital (pulp not primarily involved)
Radiology:
- Vertical or horizontal alveolar bone loss visible on periapical X-ray
- Radiolucency lateral to the root rather than at the apex
Treatment:
- Drainage via the periodontal pocket
- Root planing and scaling
- Antibiotics if systemic involvement
3. Gingival Abscess
| Feature | Detail |
|---|---|
| Origin | Superficial infection confined to the gingival soft tissue only — no involvement of deeper periodontal structures |
| Location | Marginal or interdental gingiva |
| Cause | Foreign body embedded in the gingiva (e.g., toothbrush bristle, food particle), trauma, or poor oral hygiene |
Clinical features:
- Localized, tender, fluctuant swelling of the gingiva
- No involvement of the periodontal ligament or alveolar bone
- Resolves quickly once the cause is removed
Treatment:
- Identify and remove the embedded foreign body
- Irrigation with normal saline
- Continued home irrigation; symptoms resolve rapidly
4. Pericoronal Abscess (Pericoronitis with Suppuration)
Sometimes listed as a fourth type — infection around the crown of a partially erupted tooth (most commonly the mandibular third molar/wisdom tooth).
| Feature | Detail |
|---|---|
| Origin | Food/debris impacted beneath the operculum (gingival flap overlying erupting tooth) |
| Location | Pericoronal tissues |
| Risk | Close proximity to the masticator space → trismus; spread to parapharyngeal spaces → life-threatening airway compromise |
Treatment:
- Local irrigation beneath the operculum
- Oral antibiotics (amoxicillin or metronidazole)
- Saline rinses and analgesics
- Definitive: extraction of the offending tooth
Complications of All Types (if untreated)
Dental abscesses — particularly periapical ones — can spread progressively:
- Osteomyelitis — spread into alveolar bone
- Cellulitis — spread into fascial planes of the head and neck
- Ludwig's angina — bilateral submandibular/sublingual space infection with tongue elevation, trismus, and potential airway obstruction
- Septic thrombophlebitis — ascending spread via venous channels
- Cavernous sinus thrombosis, brain abscess, mediastinitis — rare but life-threatening
The causative organisms are typically a mixed anaerobic infection (Prevotella spp., Fusobacterium spp., peptostreptococci, microaerophilic streptococci), reflecting the normal oral microbiota.
Sources: Tintinalli's Emergency Medicine, p. 1622–1624 | Harrison's Principles of Internal Medicine 22E, p. 1376 | Sherris & Ryan's Medical Microbiology, p. 6211 | Roberts and Hedges' Clinical Procedures in Emergency Medicine, p. 2062
This is a shared conversation. Sign in to Orris to start your own chat.