I now have all the textbook content and images needed. Let me compose the comprehensive, fully referenced answer:
Detailed Anatomy of the Retroperitoneum — Fascia, Spaces, Contents, Extensions, Clinical Significance, CT & MRI
Sources: Campbell Walsh Wein Urology 3-Vol Set (9780323546423); NKF Primer on Kidney Diseases 8e (9780323791229); Brenner & Rector's The Kidney (9780323532655); Grainger & Allison's Diagnostic Radiology (9780323760751); Schwartz's Principles of Surgery 11e (9781259835346)
1. OVERVIEW AND DEFINITION
The retroperitoneum is the large extraperitoneal compartment of the abdomen and pelvis, lying:
- Anterior boundary: Posterior parietal peritoneum
- Posterior boundary: Posterior abdominal wall (transversalis fascia + muscles)
- Superior boundary: Diaphragm
- Inferior boundary: Open — communicates with extraperitoneal pelvic structures (pelvic floor, Space of Bogros)
- Lateral boundary: Lateroconal fascia (fusion of Gerota fascia laminae)
2. EMBRYOLOGICAL BASIS OF RETROPERITONEAL FASCIA
The retroperitoneal fasciae arise from mesoderm. In late fetal development, the primitive mesenchyme differentiates into three strata (Tobin 1944, Skandalakis):
| Stratum | Gives Rise To | Clinical Significance |
|---|
| Outer stratum | Transversalis fascia (covers deep surface of transversus abdominis) | Defines posterior pararenal space posteriorly |
| Intermediate stratum | Gerota fascia (anterior + posterior laminae); embeds GU organs | Contains kidney, adrenal, ureter within perirenal space |
| Inner stratum | Fusion fasciae (fascia of Toldt, retroduodenal fascia); associated with GI organs | Forms the anterior boundary of the anterior pararenal space; gives rise to the White Line of Toldt |
3. RETROPERITONEAL FASCIAE — DETAILED ANATOMY
A. Lumbodorsal (Thoracolumbar) Fascia
The lumbodorsal fascia has three distinct layers investing the posterior abdominal wall musculature. They merge laterally into one layer near the tip of the 12th rib, which fuses with the aponeurosis of the transversus abdominis:
| Layer | Position | Muscles Covered |
|---|
| Posterior lamella | Superficial; originates from spinous processes | Covers erector spinae (sacrospinalis) muscles posteriorly |
| Middle lamella | Between erector spinae and quadratus lumborum | Separates the two muscle groups |
| Anterior lamella | Deep; attaches to vertebral transverse processes | Covers the ventral surface of quadratus lumborum; continuous with psoas fascia anteriorly |
All three merge laterally → single layer → fuses with transversus aponeurosis
Dorsal lumbotomy incision: A vertical incision through the lumbodorsal fascia lateral to the erector spinae and quadratus lumborum allows entry into the retroperitoneum without incising muscle - a key surgical approach for the kidney.
B. Transversalis Fascia
- Derived from the outer embryological stratum
- Lines the deep surface of the transversus abdominis muscle
- Crosses the midline anteriorly and fuses with the lumbodorsal fascia posteriorly
- Posterior to the kidney, lies anterior to the fascia investing the quadratus lumborum and psoas
- May fuse medially with the posterior lamina of Gerota fascia - this fusion creates the medial boundary of the posterior pararenal space; this plane must be incised to access the renal hilum during retroperitoneal dissection
C. Gerota Fascia (Renal Fascia / Perirenal Fascia)
Described by Romanian anatomist Dimitrie D. Gerota (1867-1939) in 1895. It is the most clinically critical retroperitoneal fascial structure.
Derived from the intermediate embryological stratum, it has two laminae:
| Lamina | Eponym | Character | CT Visibility |
|---|
| Anterior lamina | Fascia of Toldt / Prerenal fascia | Thinner | Less frequently seen on CT |
| Posterior lamina | Fascia of Zückerkandl / Retrorenal fascia | Thicker | More frequently visualized on CT |
Lateral extent — Lateroconal fascia:
The anterior and posterior laminae of Gerota fascia merge laterally to form the lateroconal fascia, which:
- Separates the anterior pararenal space (APS) from the posterior pararenal space (PPS)
- Continues anterolaterally, deep to the transversalis fascia
- Forms the lateral boundary of the perirenal space
Extent of Gerota fascia:
| Direction | Extent |
|---|
| Superior | Closed - fuses with diaphragmatic fascia; adrenal gland contained within its superior aspect (separated by thin connective tissue septum) |
| Lateral | Closed - merges into lateroconal fascia |
| Medial | Fuses with adventitia of renal vessels, aorta, IVC; may communicate across midline below the renal hilum (cadaveric injection studies) |
| Inferior | OPEN - cone-shaped, open at its inferior extent into the extraperitoneal pelvis |
Key clinical point: The inferior opening of Gerota fascia means perinephric fluid collections (urinoma, hematoma, abscess) track inferiorly into the pelvis through this open cone. This is the basis of urine tracking down to the pelvis in obstructive uropathy with fornical rupture.
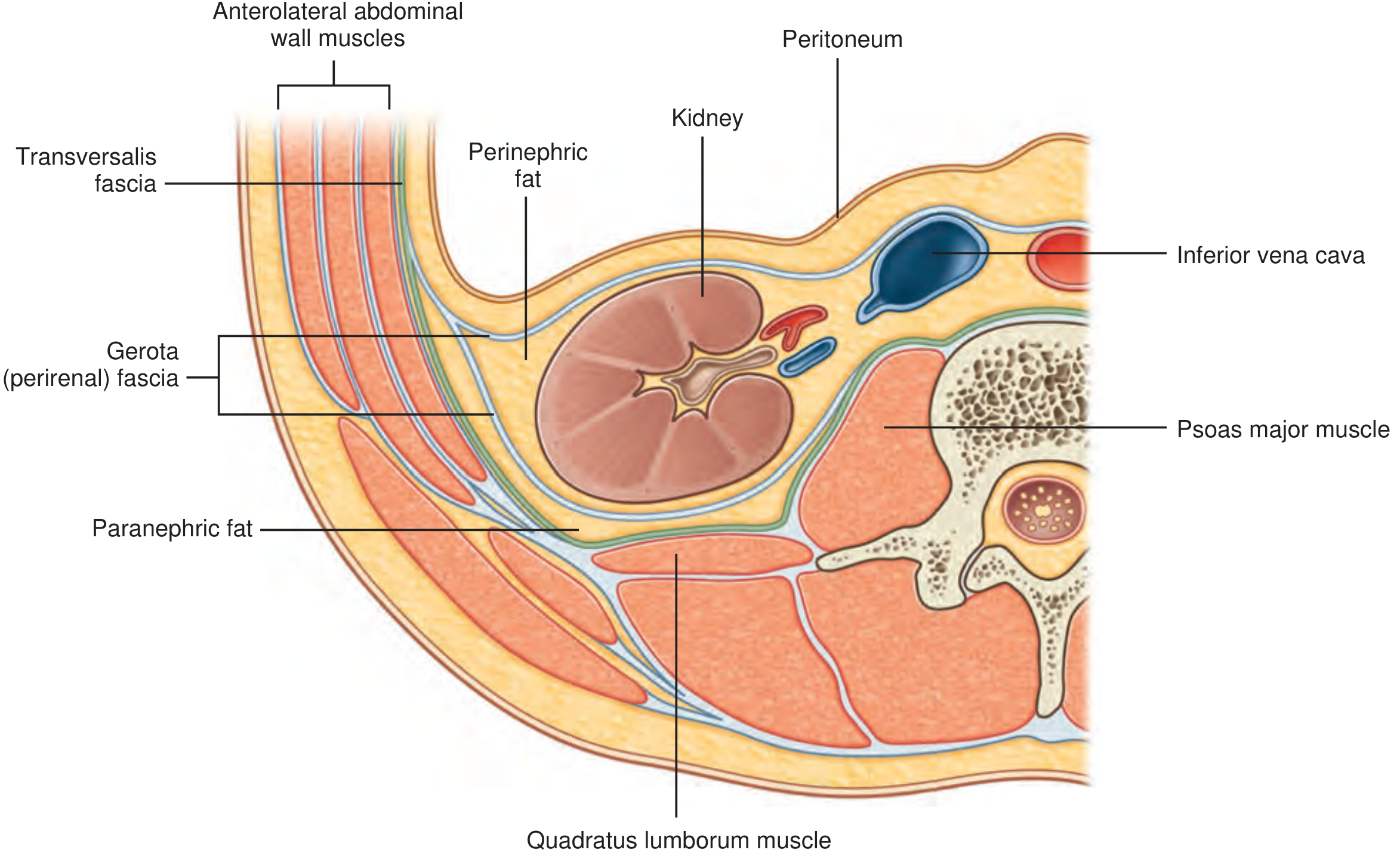
Fig. 75.16 (Campbell Walsh Wein): Organization of the fasciae and fat surrounding the kidney — showing Gerota (perirenal) fascia, transversalis fascia, perinephric fat, paranephric fat, psoas major, quadratus lumborum, IVC, kidney.
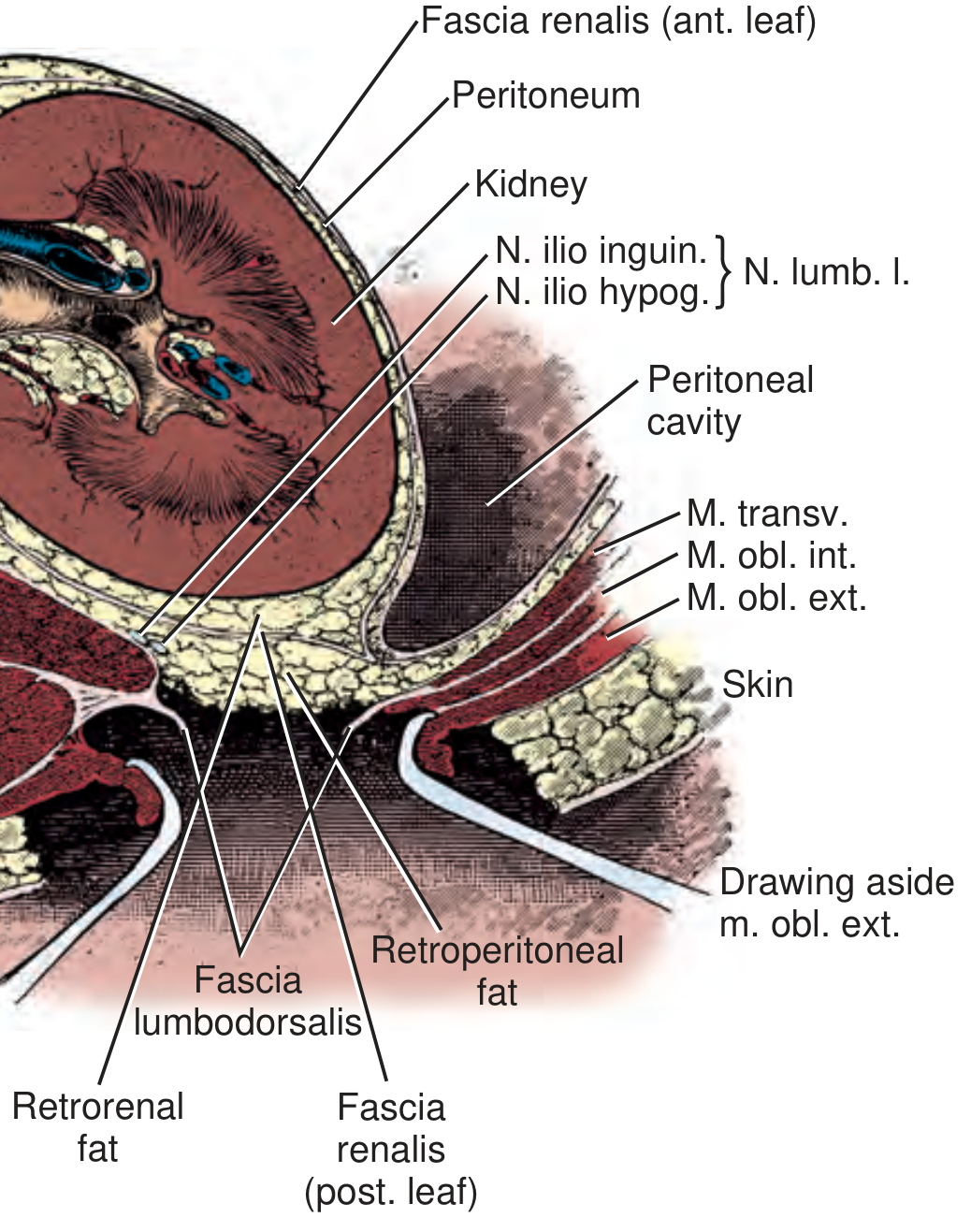
Fig. 75.13 (Campbell Walsh Wein): Transverse section through the kidney. Labels: Fascia renalis (ant. leaf) = anterior lamina of Gerota; Fascia renalis (post. leaf) = posterior lamina (Zückerkandl / fascia lumbodorsalis); Retrorenal fat = pararenal fat posterior to Gerota; Retroperitoneal fat = anterior pararenal fat.
4. THE THREE RETROPERITONEAL SPACES
The retroperitoneal fasciae divide the retroperitoneum into three major spaces:
ANTERIOR → POSTERIOR (from front to back):
Posterior parietal peritoneum
↓
ANTERIOR PARARENAL SPACE (APS)
↓ — Anterior lamina of Gerota (fascia of Toldt)
PERIRENAL SPACE (PR)
↓ — Posterior lamina of Gerota (fascia of Zückerkandl)
POSTERIOR PARARENAL SPACE (PPS)
↓ — Transversalis fascia
Posterior abdominal wall muscles
Space 1: Anterior Pararenal Space (APS)
| Feature | Detail |
|---|
| Anterior boundary | Posterior layer of parietal peritoneum |
| Posterior boundary | Anterior lamina of Gerota fascia |
| Lateral boundary | Lateroconal fascia |
| Medial boundary | Open — communicates with contralateral APS across the midline |
| Contents | Ascending colon, descending colon (secondarily retroperitoneal); pancreas (head, neck, body); duodenum (2nd and 3rd parts); colonic mesenteries |
| Fat character | Relatively sparse mesenteric/colonic peritoneal fat |
| Communication | Bilateral APS communicate across the midline behind the pancreas and duodenum |
Surgical access (White Line of Toldt):
The APS is developed surgically by incising along the White Line of Toldt - the visible lateral border of the fusion of colonic mesentery with the posterior peritoneum, formed during embryogenesis when the inner stratum GI organs fused with the primary dorsal peritoneum. Medial reflection of the colon through this plane enters the APS and exposes the kidney anteriorly.
Clinical significance of APS:
- Acute pancreatitis: Inflammatory exudate and pancreatic enzymes spread within the APS, extend bilaterally across the midline, and track into the adjacent perirenal space
- Colonic perforation / diverticulitis: Gas and fecal material spread within the APS
- Retroperitoneal duodenal injury: Gas and bile track in the APS around the duodenum
Space 2: Perirenal Space (PR) — Most Important Space
| Feature | Detail |
|---|
| Anterior boundary | Anterior lamina of Gerota fascia |
| Posterior boundary | Posterior lamina of Gerota fascia |
| Lateral boundary | Lateroconal fascia (fusion of the two laminae) |
| Medial boundary | Adventitia of renal vessels / aorta / IVC; possible midline communication below hilum |
| Superior boundary | Closed — fuses with diaphragmatic fascia |
| Inferior boundary | OPEN — cone-shaped; communicates with extraperitoneal pelvis |
| Shape | Inverted cone / funnel, open inferiorly |
Contents of the Perirenal Space:
| Structure | Notes |
|---|
| Kidney | Surrounded by perinephric fat |
| Adrenal gland | Superior, separated by thin fascia from kidney |
| Ureter | Descends from renal pelvis through inferior cone |
| Perinephric (perirenal) fat | Finer, lighter yellow than paranephric fat; fills the space between the kidney and Gerota fascia |
| Renal artery and vein (vascular pedicle) | At the renal hilum |
| Gonadal vessels (testicular/ovarian) | Descend inferiorly through the open cone |
| Kumin septa | Fine fibrous trabeculae within perinephric fat; thicken in renal inflammation ("perinephric stranding" on CT) |
| Lymphatics | Follow renal vessels |
Fat character: Perinephric fat is finer and lighter yellow than paranephric fat (coarser yellow-orange). This color distinction helps during colon mobilization for retroperitoneal surgery.
Pathological collections within the perirenal space:
| Type | Cause | Behavior |
|---|
| Urinoma | Fornical rupture (intrapelvic pressure >35 cmH₂O), trauma, iatrogenic | Tracks inferiorly through open cone → pelvis |
| Perinephric hematoma | Renal laceration, trauma, ruptured aneurysm, anticoagulation | Contained by Gerota fascia until volume overwhelms |
| Perinephric abscess | Infected urinoma, ascending UTI, hematogenous seeding | Contained; may rupture through fascia in necrotizing infection |
| Lymphocele | Post-transplant lymphadenectomy | Within perirenal space / pelvic extraperitoneal space |
Renal cell carcinoma TNM staging vis-a-vis Gerota fascia:
- T3a: Perinephric/renal sinus fat invasion, not beyond Gerota fascia
- T3b: Renal vein or IVC involvement below diaphragm
- T4: Tumor invades beyond Gerota fascia → includes ipsilateral adrenal extension
Space 3: Posterior Pararenal Space (PPS)
| Feature | Detail |
|---|
| Anterior boundary | Posterior lamina of Gerota fascia |
| Posterior and lateral boundaries | Transversalis fascia |
| Medial boundary | Fusion of transversalis fascia with posterior lamina of Gerota → medial closed |
| Contents | Fat only — the coarser yellow-orange "pararenal fat body" (no organs) |
| Inferior extension | Communicates with Space of Bogros (between transversalis fascia and iliac fascia, lateral to iliac vessels) |
Clinical significance of PPS:
- Contains no organs - fluid here is rare
- Hemorrhage from aortic aneurysm rupture may track posterolaterally into PPS
- Posterior pararenal fat is seen most prominently posterior to the kidney on cross-sectional imaging
5. RETROPERITONEAL CONTENTS — COMPLETE LIST
Primary Retroperitoneal Organs
Structures that developed retroperitoneally and were never within the peritoneal cavity:
- Kidneys (within perirenal space)
- Ureters (within / descending from perirenal space)
- Adrenal (suprarenal) glands (within perirenal space, superior)
- Abdominal aorta and branches
- Inferior vena cava and tributaries
- Lumbar lymph nodes and cisterna chyli
- Sympathetic trunks and lumbar plexus
Secondarily Retroperitoneal Organs
Organs that began intraperitoneal but fused posteriorly during embryogenesis:
- Duodenum — 2nd (descending) and 3rd (horizontal) portions
- Ascending colon and hepatic flexure
- Descending colon and splenic flexure
- Pancreas — head, neck, body (the tail is intraperitoneal within the splenorenal ligament)
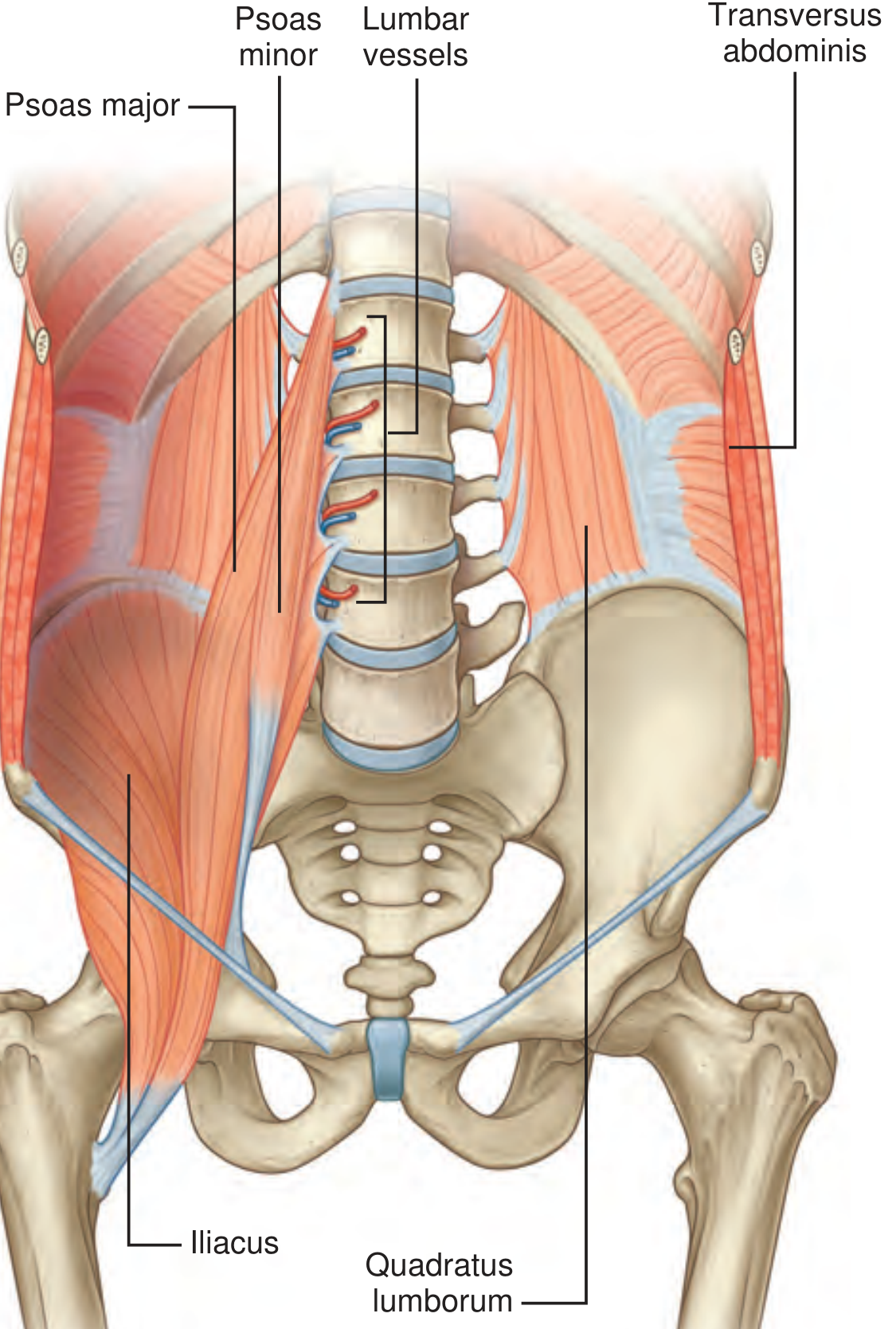
6. POSTERIOR ABDOMINAL WALL — MUSCLE ANATOMY
Fig. 75.8 (Campbell Walsh Wein): Posterior abdominal wall muscles — Psoas major (T12-L5 to lesser trochanter), Psoas minor, Iliacus (iliac fossa to lesser trochanter), Quadratus lumborum (L5 + iliac crest to 12th rib + L1-L4), Transversus abdominis, with lumbar vessels crossing anteriorly.
| Muscle | Origin | Insertion | Function | Retroperitoneal Significance |
|---|
| Psoas major | T12-L5 vertebral bodies | Lesser trochanter | Hip flexion | Kidney lies on its anterior surface; psoas shadow obliteration = retroperitoneal fluid/mass |
| Psoas minor | T12-L1 | Pelvic brim | Weak lumbar flexion | Absent in many individuals |
| Iliacus | Iliac fossa, sacrum | Lesser trochanter | Hip flexion | Iliacus hematoma in anticoagulated patients → femoral nerve compression |
| Quadratus lumborum | L5 vertebra, iliac crest | 12th rib, L1-L4 transverse processes | Depress 12th rib, lateral bending | Posterior to kidney; divides posterior musculature |
| Erector spinae | Sacrum, vertebrae | Lower ribs, vertebrae | Spinal extension | Posterior wall deep to lumbodorsal fascia |
| Transversus abdominis | Lumbodorsal fascia, iliac crest, ribs 7-12 | Linea alba, pubic crest | Compress abdomen | Fuses with lumbodorsal fascia; gives rise to transversalis fascia |
7. VASCULAR ANATOMY OF THE RETROPERITONEUM
Aorta and Branches
The abdominal aorta enters at T12 through the aortic hiatus and bifurcates at L4 into the common iliac arteries.
| Branch | Level | Supply |
|---|
| Inferior phrenic arteries | T12 | Diaphragm; give off superior suprarenal arteries |
| Celiac trunk | T12/L1 | Liver, stomach, spleen, duodenum, pancreas (contains aorticorenal ganglion) |
| Superior mesenteric artery (SMA) | L1 | Small bowel, right colon to splenic flexure |
| Renal arteries | L1-L2 | Kidneys; right renal artery passes posterior to IVC |
| Gonadal (testicular/ovarian) arteries | L2 | Gonads; arise below renal arteries |
| Inferior mesenteric artery (IMA) | L3-L4 | Left colon to upper rectum |
| Lumbar arteries (x4 pairs) | L1-L4 vertebral bodies (posterior) | Posterior body wall and spine |
| Median sacral artery | Posterior aorta just above bifurcation | Sacrum and coccyx |
| Common iliac arteries | L4 | Bifurcate into internal and external iliac |
Inferior Vena Cava and Tributaries
The IVC forms from the confluence of common iliac veins at the level of L5, inferior and to the right of the aortic bifurcation. It ascends to the right of the aorta, anterior to the vertebral bodies, entering the thorax through the central tendon of the diaphragm at T8.
| Key venous asymmetry | Left | Right |
|---|
| Gonadal vein | Enters left renal vein at right angle | Enters IVC directly |
| Adrenal vein | Enters left renal vein | Enters IVC directly (short, no tributaries) |
| Renal vein | Longer (7-8 cm); receives gonadal + adrenal + lumbar | Shorter (3 cm); no tributaries typically |
Clinical note: Left gonadal vein draining into the left renal vein at right angles + its greater length → increased back pressure → left-sided varicocele more common. A sudden right varicocele should prompt retroperitoneal imaging to exclude right RCC with venous thrombus.
8. LYMPHATICS OF THE RETROPERITONEUM
The retroperitoneal lymphatics consist of para-aortic (lumbar) lymph nodes and paracaval nodes running alongside the major vessels.
Drainage levels:
- Testes/ovaries: Follow gonadal vessels → para-aortic nodes at L1-L2 (primary landing zone for testicular tumors)
- Kidneys: Para-aortic nodes (left side) and paracaval nodes (right side); inter-aortocaval nodes
- Bladder, prostate, uterus, cervix: Pelvic nodes (obturator, internal iliac, external iliac) → common iliac → para-aortic
- Distal penis/vulva/anus/lower rectum: Inguinal nodes (exception to the above)
All lumbar lymphatics → lumbar lymphatic trunks → cisterna chyli (at L1-L2, between aorta and right crus of diaphragm) → thoracic duct.
9. NERVOUS STRUCTURES
Autonomic Nervous System
Sympathetic nervous system:
- Preganglionic fibers exit T1-L2 via ventral roots → anterior rami → ipsilateral sympathetic trunk
- The paired sympathetic trunks run medial to the psoas, along the anterolateral aspect of the spine
- Lumbar arteries and veins cross the sympathetic trunk perpendicularly
- Fibers may synapse in the sympathetic chain ganglia or leave as splanchnic nerves to synapse in aortic autonomic plexuses
Major retroperitoneal autonomic plexuses:
- Celiac plexus (paired ganglia lateral to celiac artery): innervation to kidney, adrenal, renal pelvis, proximal ureter, testes
- Renal plexus (adjacent to renal arteries): contains aorticorenal ganglion (inferior extension of celiac ganglion)
- Superior mesenteric plexus
- Superior hypogastric plexus (L4-L5 level; "presacral nerve"): sympathetic innervation to pelvic viscera; injury during aortic / lymph node surgery → retrograde ejaculation
Parasympathetic nervous system:
- Craniosacral outflow
- S2-S4 → pelvic splanchnic nerves (nervi erigentes) → pelvic viscera
- Vagus (CN X) → abdominal and thoracic viscera
Somatic Nervous System — Lumbosacral Plexus
| Nerve | Roots | Course | Clinical |
|---|
| Iliohypogastric | L1 | Exits lateral border of psoas, crosses quadratus lumborum | Sensory to groin; injured in flank incisions |
| Ilioinguinal | L1 | Crosses quadratus lumborum and iliacus, runs through inguinal canal | Sensory to scrotum/labia and medial thigh |
| Genitofemoral | L1-L2 | Pierces psoas anteriorly, descends on its anterior surface | Genital and femoral branches; cremasteric reflex |
| Lateral femoral cutaneous | L2-L3 | Exits lateral border of psoas → below inguinal ligament | Sensory to lateral thigh; meralgia paresthetica |
| Femoral | L2-L4 | Within groove between psoas and iliacus, beneath inguinal ligament | Motor to quadriceps; sensory anterior thigh; injured in iliacus hematoma or large retroperitoneal mass |
| Obturator | L2-L4 | Descends on medial border of psoas → obturator foramen | Motor to adductors; sensory medial thigh |
| Lumbosacral trunk | L4-L5 | Joins sacral plexus | Sciatic nerve precursor |
10. KIDNEY ANATOMY WITHIN THE RETROPERITONEUM
Position and Relations
- Lie retroperitoneally on either side of the vertebral column, resting on the psoas muscles
- Longitudinal axes oblique (~30° anterior rotation): upper poles more medial and posterior, lower poles more lateral and anterior
- Respiratory mobility: ~3 cm inferior descent during inspiration and on standing
- Right kidney: T12-L3; displaced inferiorly by liver
- Left kidney: T11-L3; slightly higher
Vertebral level mnemonic: Right kidney = L1-L3; Left kidney = T12-L3
Anterior Relations
| Side | Anterior Relations (superior to inferior) |
|---|
| Right | Liver (hepatorenal ligament), adrenal (superomedial), duodenum 2nd part (medial - Kocher maneuver for access), hepatic flexure, small intestine |
| Left | Stomach + spleen (superiorly; splenorenal ligament), adrenal (superomedial), tail of pancreas + splenic vessels (medially), splenic flexure, descending colon, jejunum |
Posterior Relations
Both kidneys (posterior relations are symmetric):
- Diaphragm (upper poles)
- 12th rib (right); 11th and 12th ribs (left)
- Subcostal nerve and vessels (T12) cross obliquely
- Iliohypogastric nerve (L1) and ilioinguinal nerve (L1) cross inferiorly
- Psoas major (medially), quadratus lumborum (laterally), aponeurosis of transversus abdominis (lateral)
Renal Hilar Anatomy — Mnemonic VAUA
From anterior to posterior at the renal hilum:
- V = Renal Vein (most anterior)
- A = Renal Artery
- U = Renal pelvis (Ureter)
- A = Posterior segmental Artery (most posterior)
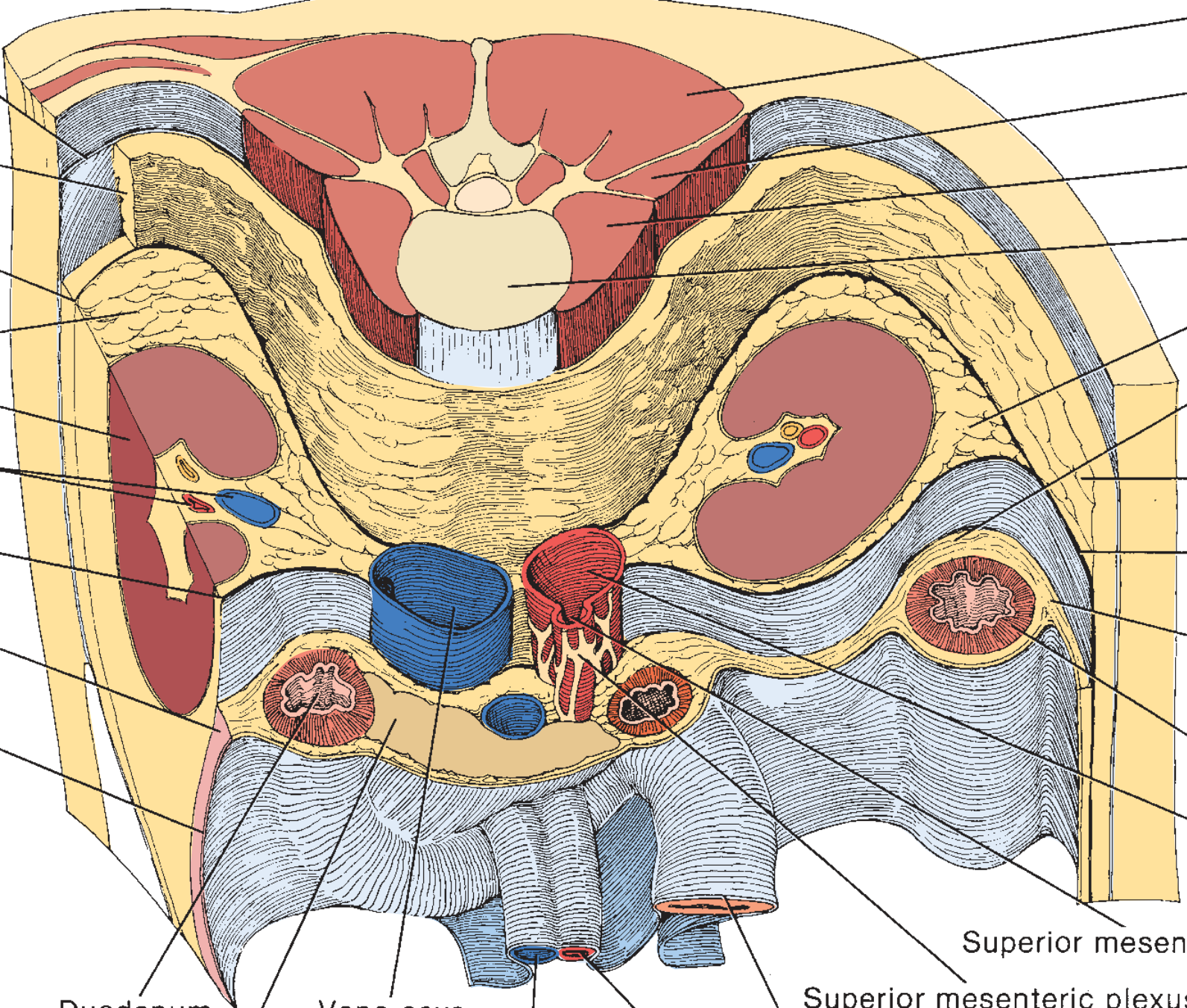
Fig. 75.22 (Campbell Walsh Wein): Retroperitoneal cross-sectional anatomy at the level of the renal pedicles — both kidneys, perinephric fat, duodenum, pancreas, IVC, aorta, and renal vessels.
11. RADIOLOGICAL ANATOMY — CT AND MRI
CT Anatomy of the Retroperitoneum
Technique: MDCT with thin slices (0.625-1.25 mm) in axial plane with coronal and sagittal reformats. Bone and soft-tissue windows. Contrast enhancement for vascular/parenchymal assessment.
CT — Normal Fascial Appearances
| Structure | CT Appearance |
|---|
| Gerota fascia (posterior lamina) | Thin, linear soft-tissue density line posterior to the kidney, separating perinephric fat from paranephric fat — more reliably visualized than the anterior lamina |
| Gerota fascia (anterior lamina) | Thin, often not visible unless thickened by pathology |
| Perinephric fat | Low-density (-100 to -50 HU) fat surrounding the kidney within Gerota fascia; fine, homogeneous |
| Paranephric fat | Low-density fat external to Gerota fascia, most prominent posterior to kidney; coarser, yellow-orange (but on CT both fats are identical density) |
| Lateroconal fascia | Thin line at the lateral margin of the retroperitoneum (lateral to kidney), between the anterior and posterior pararenal spaces |
| Transversalis fascia | Deep to posterior pararenal fat; separates PPS from abdominal wall musculature |
| Psoas muscle | Well-defined, elliptical muscle on either side of lumbar spine; loss of psoas shadow on plain film = retroperitoneal fluid/mass |
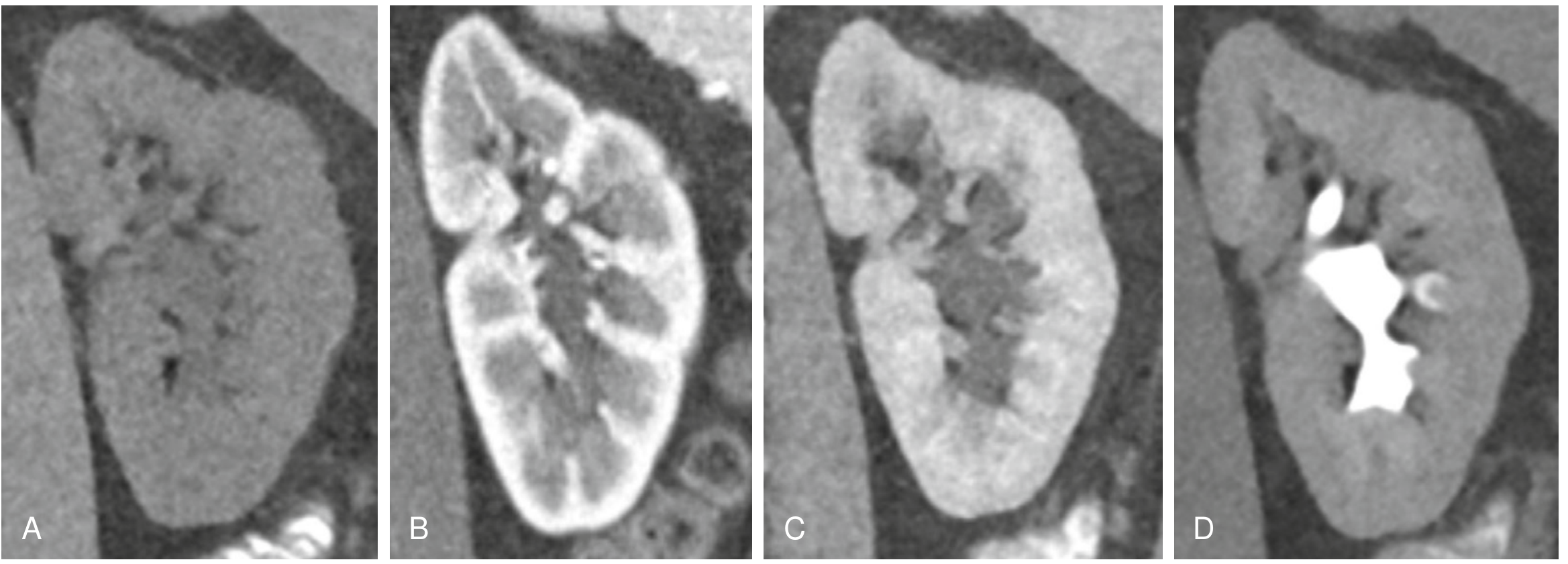
CT — Normal Kidney Appearances at Each Phase
Fig. 6.4 (NKF Primer on Kidney Diseases): Normal kidney CT in four phases - A: Non-contrast, B: Corticomedullary, C: Nephrographic, D: Excretory.
| Phase | Timing Post-Injection | Kidney CT Appearance | Primary Use |
|---|
| Non-contrast (NECT) | Pre-injection | Homogeneous; 30-60 HU; no corticomedullary differentiation | Stones (calc. HU >100), fat (AML, -10 to -50 HU), hemorrhage (60-80 HU), baseline density for mass characterization |
| Arterial phase | 12-25 sec | Renal arteries opacified; cortical blush beginning | Renal artery stenosis, aneurysm evaluation; rarely used alone |
| Corticomedullary phase (CMP) | 30-70 sec | Cortex dramatically enhanced (100-200 HU); medullary pyramids remain low density → maximum corticomedullary differentiation (CMD) | Vascular anatomy; renal artery/vein relationship to tumor; venous anatomy; pre-op partial nephrectomy planning |
| Nephrographic phase (NGP) | 80-120 sec | Cortex and medulla equally and homogeneously enhanced (~100-120 HU) | Best phase for renal mass/neoplasm detection; small masses best seen here; renal infarction; pyelonephritis |
| Excretory (pyelographic) phase | >3-5 min (5-15 min) | Collecting system, ureters, bladder opacified with high-density contrast | Collecting system anatomy; relationship of tumor to pelvis; CT urography (urothelial tumors); pre-op partial nephrectomy |
Normal attenuation values: Pre-contrast renal parenchyma 30-60 HU → increases to 80-200 HU post-contrast depending on phase.
CT identification of retroperitoneal fascial spaces:
| Space | CT Appearance | Pathology |
|---|
| Perirenal space | Fat surrounding kidney between two laminae of Gerota; soft-tissue strands (Kumin septa) = normal | "Perinephric stranding" (increased density) = infection/inflammation/trauma; perinephric fluid = urinoma/hematoma/abscess |
| Anterior pararenal space | Contains pancreas, duodenum, colon; surrounded by fat | Pancreatitis = fat stranding + fluid within APS; "dirty fat" bilaterally; peripancreatic necrosis |
| Posterior pararenal space | Pure fat posterior to Gerota; no organs | Retroperitoneal hemorrhage (AAA rupture can track here posterolaterally) |
CT differentiation of perinephric fluid:
| Content | HU | Appearance |
|---|
| Urinoma | 0-20 HU (water density) | Simple fluid; tracks inferiorly along ureter |
| Hematoma (acute) | 50-80 HU | High-density fluid; sentinel clot sign near laceration |
| Abscess | Variable; +/- gas | Complex fluid with gas bubbles; rim enhancement |
| Lymphocele | 0-20 HU | Simple, well-defined; post-transplant |
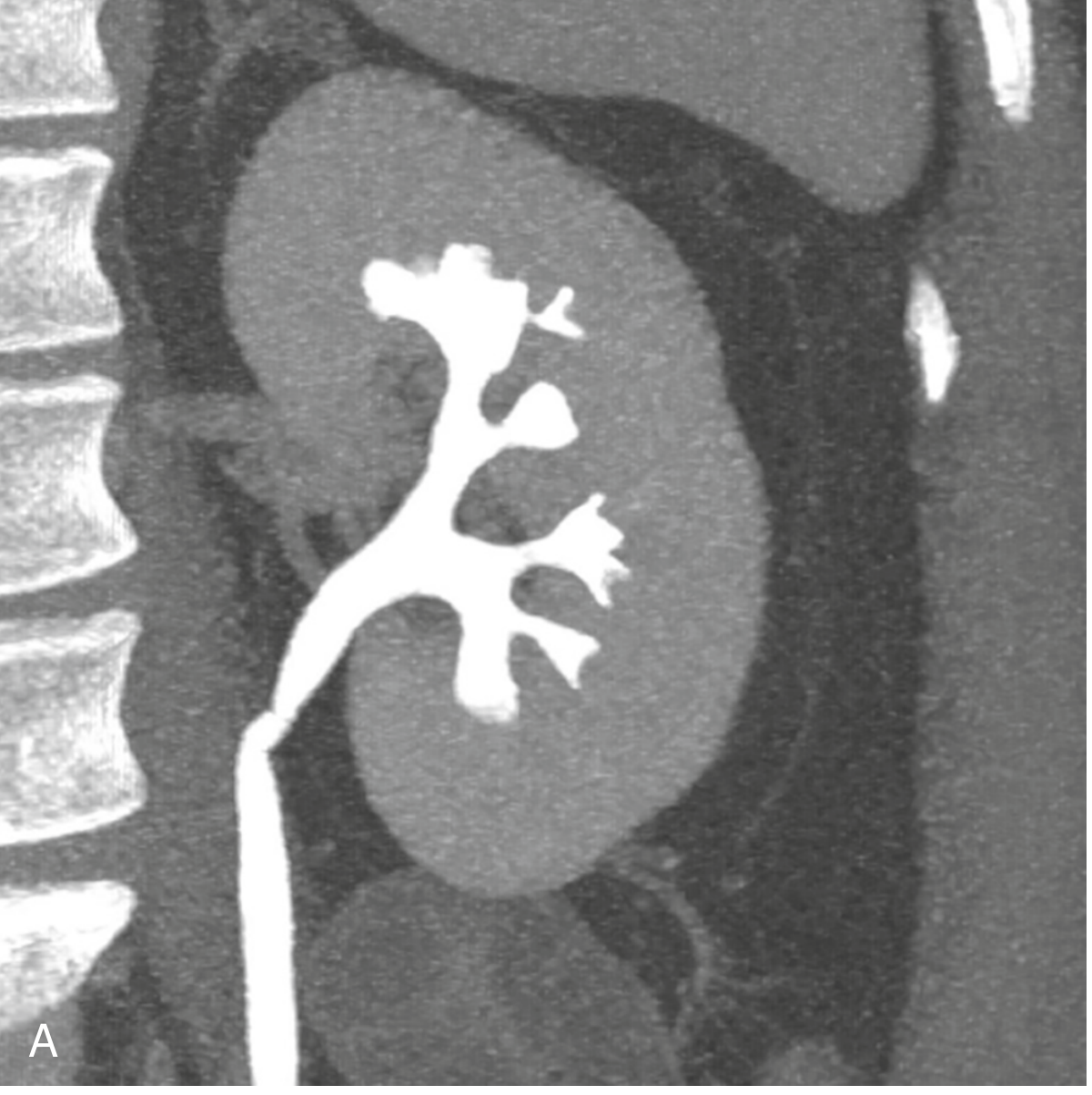
CT Excretory Phase — Normal Collecting System Anatomy
Fig. 6.2 (NKF Primer): Coronal CT urogram in excretory phase — normal kidney with pelvicalyceal system and proximal ureter opacified with contrast. The collecting system has cupped minor calyces, funnel-shaped infundibula, and a smooth renal pelvis.
Normal collecting system on CT excretory phase:
- Minor calyces: concave (cupped), sharp fornical angles, 10-14 per kidney
- Major calyces: formed by union of 2-3 minor calyces
- Renal pelvis: smooth, triangular; extrarenal or intrarenal
- Three normal ureteric constrictions: UPJ, pelvic brim (crossing iliac vessels), UVJ
- Normal ureteric course: along anterior psoas surface, within 1 cm of lateral margin of vertebral transverse processes
MRI Anatomy of the Retroperitoneum
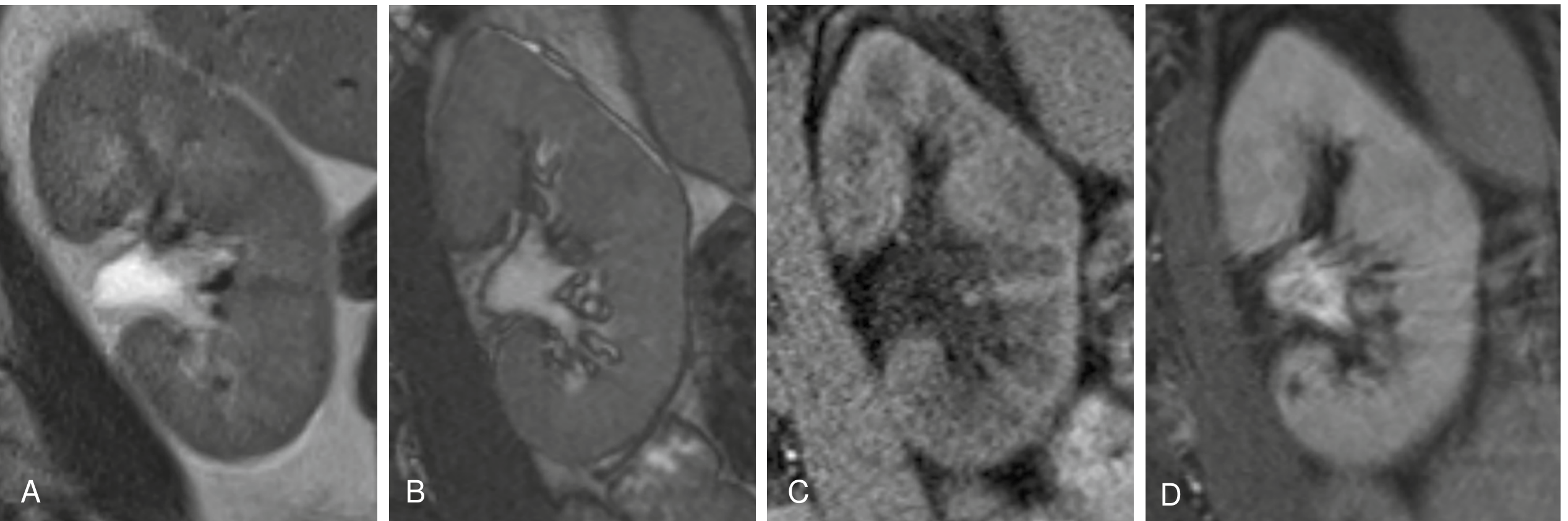
Fig. 6.7 (NKF Primer): Normal kidney MRI sequences - T2 (A), bSSFP (B), T1 (C), post-gadolinium T1 (D). Note: On T1, cortex is brighter than medulla. On T2, medulla becomes slightly brighter.
MRI Signal Characteristics
| Sequence | Renal Cortex | Medullary Pyramids | Renal Sinus | Perirenal Fat |
|---|
| T1-weighted | Brighter (higher SI than medulla) | Lower signal | Hyperintense (fat) | Hyperintense |
| T2-weighted | Intermediate to low | Slightly brighter than cortex | Low (fibrous) / high (fat) | Low (fat signal persists unless fat-sat used) |
| Fat-suppressed T1 | Intermediate | Low | Low (fat suppressed) | Low (fat suppressed) |
| Post-gadolinium T1 | Strong enhancement (CMP); equal enhancement (NGP) | Enhances in NGP | Enhancement of renal vessels | No enhancement |
| DWI | Intermediate ADC | Higher ADC | Low signal (fat) | High ADC |
Gerota fascia on MRI:
- Seen as a thin low-signal line on T1 and T2 separating the higher-signal perinephric fat from the higher-signal paranephric fat (when both fat layers are present)
- Fat-suppressed sequences null both fat compartments, making Gerota fascia less visible unless thickened
Corticomedullary differentiation (CMD) on MRI:
- Visible without contrast on T1 (cortex brighter than medulla)
- CMD disappears in chronic kidney disease (cortical fibrosis/atrophy makes cortex isointense to medulla)
- Contrast-enhanced MRI: CMD at 60 sec; nephrographic phase at 90-120 sec
Perinephric fat MRI:
- T1: Hyperintense (fat)
- T2: Intermediate to hyperintense
- STIR or fat-sat sequences: Fat signal nulled / suppressed → perinephric collections and edema become conspicuous
12. INTERFASCIAL PLANES AND COMMUNICATIONS
| Space/Plane | Location | Communication / Clinical Significance |
|---|
| Space of Bogros | Between transversalis fascia and iliac fascia, lateral to iliac vessels in the pelvis | Posterior pararenal fat communicates inferiorly here; important for laparoscopic preperitoneal hernia repair |
| Space of Retzius (prevesical space) | Between pubic symphysis/anterior abdominal wall and bladder | Pelvic hematomas; laparoscopic prostatectomy access; urine extravasation from bladder rupture tracks here |
| Retrorectal space | Between rectum and sacrum | Pelvic surgery; presacral tumor access |
| Periureteric fascial tunnel | The inferior open cone of Gerota fascia descends around the ureter | Perinephric fluid tracks inferiorly along the ureter |
| Transperitoneal communication (controversial) | Below the renal hilum, perirenal spaces may communicate across midline | Bilateral perinephric collections possible from unilateral disease |
13. ADRENAL GLAND ANATOMY IN THE RETROPERITONEUM
The adrenal (suprarenal) glands are enclosed within the perirenal space (within Gerota fascia), separated from the kidney by a thin connective tissue septum within the same space.
- Right adrenal: posterior to IVC; between IVC and right crus of diaphragm; pyramidal/triangular shape
- Left adrenal: medial to upper pole of left kidney; crescentic/semilunar shape
- CT: inverted Y or V shape on axial; normal limb thickness <10 mm
- MRI: T1 isointense to liver; T2 slightly hyperintense; pheochromocytoma: T2 very bright; adenoma: signal dropout on out-of-phase T1 (intracellular fat)
Vascular supply:
- Three arterial sources: Superior suprarenal (from inferior phrenic); middle suprarenal (from aorta); inferior suprarenal (from renal artery)
- Single vein: Left adrenal vein → left renal vein; Right adrenal vein → IVC directly (short, no tributaries - surgical danger)
14. SPREAD OF DISEASE — RETROPERITONEAL SPACE ANALYSIS
| Disease | Primary Space | Mechanism of Spread |
|---|
| Acute pancreatitis | Anterior pararenal (pancreas in APS) | Enzymes spread bilaterally within APS; extend posteriorly into perirenal space; also spread along Toldt fascia to root of mesentery |
| Retroperitoneal hemorrhage (AAA rupture) | Typically posterior pararenal; also perirenal | May be contained by Gerota fascia initially; massive rupture fills all spaces |
| Renal trauma (Grade III-IV) | Perirenal space | Contained by Gerota fascia; tracks inferiorly → pelvis through open inferior cone |
| Ascending UTI / pyonephrosis | Perirenal space | Perinephric abscess; Gerota acts as barrier |
| Retroperitoneal fibrosis | Perirenal/anterior to IVC and aorta | Encases ureters → medial deviation ("ski-slope deformity" on IVU); must be distinguished from retroperitoneal malignancy |
| Retroperitoneal lymphoma / metastases | Para-aortic nodes | Displaces kidneys/ureters; wraps around vessels |
| Colonic carcinoma perforation | Anterior pararenal | Tracks along colonic mesentery within APS |
| Duodenal perforation (retroperitoneal) | Anterior pararenal | Gas and bile in right APS (Rigler sign absent; need CT) |
SUMMARY DIAGRAM
CROSS-SECTION (Axial view, right side):
PERITONEAL CAVITY
|
Posterior parietal peritoneum
|
══════════════════════════════════
ANTERIOR PARARENAL SPACE (APS)
Contents: Ascending colon,
duodenum 2nd/3rd parts, pancreas
══════════════════════════════════
↑ Ant. lamina of Gerota (Toldt)
══════════════════════════════════
PERIRENAL SPACE
Contents: Kidney, adrenal, ureter,
perinephric fat, renal vessels,
gonadal vessels, lymphatics
(Open inferiorly → pelvis)
══════════════════════════════════
↓ Post. lamina of Gerota (Zückerkandl)
══════════════════════════════════
POSTERIOR PARARENAL SPACE (PPS)
Contents: FAT ONLY (pararenal fat)
══════════════════════════════════
↓ Transversalis fascia
══════════════════════════════════
POSTERIOR ABDOMINAL WALL MUSCLES
(Psoas, Quadratus lumborum, Erector spinae)
+ Lumbodorsal (thoracolumbar) fascia
Sources: Campbell Walsh Wein Urology, Chapter 75 — "Surgical, Radiographic, and Endoscopic Anatomy of the Retroperitoneum" (pp. 2212-2241); NKF Primer on Kidney Diseases 8e, Chapter 6 (pp. 70-75); Brenner & Rector's The Kidney (Chapter on Renal Imaging); Grainger & Allison's Diagnostic Radiology — Pancreas and Retroperitoneum chapters; Schwartz's Principles of Surgery 11e, Chapter 35.