Hepato renal syndrome in details
Reading File
Finding Sources
Searching PubMed
"hepatorenal syndrome" diagnosis treatment
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
I have sufficient information now to write a comprehensive, well-sourced answer. Let me compile everything I've gathered.
Hepatorenal Syndrome (HRS) - A Detailed Overview
Definition
Hepatorenal syndrome is a form of functional acute kidney injury (AKI) that occurs in patients with advanced cirrhosis, acute liver failure, or alcoholic hepatitis. Histologically, the kidneys are entirely normal - the syndrome reflects hemodynamic derangement, not intrinsic renal pathology. This reversibility is key: transplanting a kidney from a patient with HRS into a non-cirrhotic recipient restores normal function.
- Harrison's Principles of Internal Medicine 22E, p. 1378
- Sleisenger and Fordtran's Gastrointestinal and Liver Disease, p. 1489
Epidemiology
- Acute renal dysfunction occurs in 15-25% of hospitalized patients with cirrhosis
- HRS accounts for 10-30% of those cases
- Annual incidence of HRS in cirrhotic patients with ascites: ~8%, and up to 40% in some reports
- HRS develops in approximately:
- 30% of cirrhotic patients admitted with SBP or other infection
- 25% hospitalized with severe alcoholic hepatitis
- 10% requiring serial large-volume paracenteses
Classification
The older Type 1 / Type 2 terminology has been updated by the International Club of Ascites (ICA):
| Old Term | New Term | Description |
|---|---|---|
| Type 1 HRS | HRS-AKI | Rapid, progressive renal failure over 1-2 weeks; high mortality |
| Type 2 HRS | HRS-NAKI / HRS-CKD | Gradual, stable reduction in GFR; associated with refractory ascites; better prognosis than HRS-AKI |
HRS-AKI is characterized by Stage 2 or 3 AKI (serum creatinine >2x baseline). HRS-CKD is a more chronic form where GFR reduction persists but is relatively stable. - Sabiston Textbook of Surgery, p. 943; Harrison's 22E, p. 1379
Pathophysiology
HRS arises from three interacting mechanisms:
1. Splanchnic and Systemic Arterial Vasodilation
Portal hypertension drives intense splanchnic vasodilation via vasoactive mediators including nitric oxide (NO), carbon monoxide (CO), glucagon, prostacyclin, adrenomedullin, and endogenous opiates. This reduces effective circulating blood volume and blood pressure. Initially, compensatory increases in heart rate and cardiac output create a hyperdynamic circulation.
2. Compensatory Renal Vasoconstriction
As splanchnic vasodilation worsens, compensatory responses are activated:
- Renin-angiotensin-aldosterone system (RAAS)
- Sympathetic nervous system (SNS) activation
- Non-osmotic release of arginine vasopressin (ADH)
These mechanisms cause intense renal vasoconstriction, sodium/water retention, reduced GFR, and ultimately decreased renal perfusion. Intradial renal events - involving altered production of endothelins, prostaglandins, kallikreins, and F2-isoprostanes - further amplify vasoconstriction.
3. Cardiac Dysfunction (Cirrhotic Cardiomyopathy - CCM)
Impaired cardiac function exacerbates renal hypoperfusion. Studies show HRS develops in cirrhotic patients with more severe arterial vasodilation and lower cardiac output.
Note: Prolonged intense renal vasoconstriction can lead to tubular damage, causing HRS to evolve from a functional syndrome into organic disease.
The full pathophysiologic cascade is illustrated below:
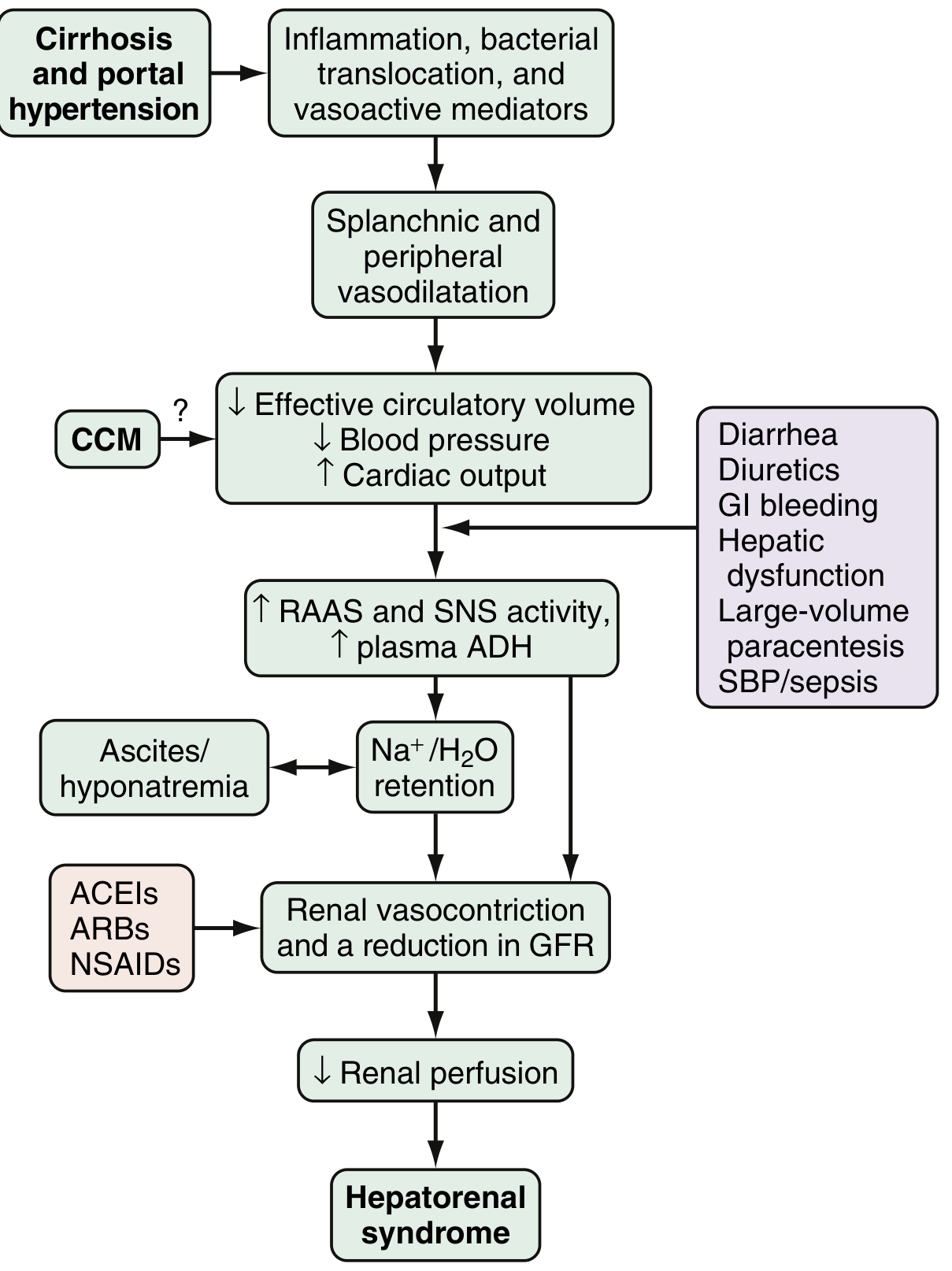
Proposed pathophysiology and triggers of HRS. CCM = cirrhotic cardiomyopathy; RAAS = renin-angiotensin-aldosterone system; SNS = sympathetic nervous system; ACEIs/ARBs/NSAIDs = aggravating nephrotoxic/hemodynamic agents.
- Sleisenger and Fordtran, pp. 1489-1491
Clinical Features
- Most patients with HRS are asymptomatic regarding renal symptoms
- Decreased urine output may be noted
- Typical presentation: advanced cirrhosis with large ascites, often triggered by SBP, GI bleed, or large-volume paracentesis
- Hyponatremia is very common
- AKI reduces GFR, raises BUN/creatinine, and may present as hepatic encephalopathy
- Urine studies (when present) typically show:
- Urine sodium <10 mmol/L
- Urine osmolality > plasma osmolality (tubular function preserved)
AKI Staging (ICA Criteria)
| Stage | Creatinine Rise |
|---|---|
| Stage 1 | 0.3 mg/dL rise OR 1.5-2x baseline |
| Stage 2 | >2-3x baseline |
| Stage 3 | >3x baseline OR creatinine ≥4 mg/dL with acute rise ≥0.3 mg/dL, OR renal replacement therapy needed |
- Sleisenger and Fordtran, Table 94.2
Diagnostic Criteria (ICA 2015 Revised Consensus)
HRS is a diagnosis of exclusion. All of the following must be met (Box 94.2):
- Cirrhosis with ascites
- Diagnosis of AKI according to ICA-AKI criteria (50% creatinine rise from baseline within 7 days, OR 0.3 mg/dL rise within 48 hours)
- No response after ≥48 hours of diuretic withdrawal and IV albumin (1 g/kg/day, max 100 g/day)
- Absence of shock
- No recent nephrotoxic agents (ACEIs, ARBs, NSAIDs, aminoglycosides)
- No intrinsic renal disease (proteinuria >500 mg/day, microhematuria >50 RBC/HPF, or abnormal renal ultrasound)
Important: Reduced urine output is NOT a criterion in cirrhotic patients because ascites/sodium retention causes oliguria even with normal GFR.
Urinary biomarkers (IL-18, NGAL) may help distinguish HRS from acute tubular necrosis but are not yet standard practice.
- Sleisenger and Fordtran, pp. 1489-1491; Goldman-Cecil Medicine
Differential Diagnosis of AKI in Cirrhosis
| Category | Examples |
|---|---|
| Worsening vasodilation | Sepsis, vasodilator drugs, large-volume paracentesis without albumin |
| Decreased effective arterial volume | GI hemorrhage, overdiuresis, lactulose-induced diarrhea |
| Renal vasoconstriction | NSAIDs |
| Nephrotoxic injury | Aminoglycosides, contrast agents |
| Intrinsic renal disease | Acute tubular necrosis (ATN), glomerulonephritis, interstitial nephritis |
| Obstructive | Urinary obstruction |
Prevention
The high mortality of HRS makes prevention the priority:
- Avoid intravascular volume depletion: judicious use of diuretics, avoid lactulose overdose, always give albumin (6-8 g/L removed) with large-volume paracentesis
- Avoid/minimize nephrotoxins: NSAIDs, ACEIs, ARBs, aminoglycosides
- Prompt diagnosis and treatment of infections (SBP, bacteremia)
- SBP prophylaxis in at-risk patients (ascites protein <1 g/L + advanced liver dysfunction)
- In SBP: IV albumin (1.5 g/kg at diagnosis, 1 g/kg on day 3) reduces risk of HRS and improves survival
- Pentoxifylline for severe alcohol-associated hepatitis (reduces TNF-mediated vasodilation)
- Prevention of variceal bleeding (beta-blockers, endoscopic band ligation)
Treatment
Treatment has two goals: (1) bridge the patient to liver transplantation, and (2) reverse hemodynamic derangement.
Step 1: General Measures
- Discontinue all nephrotoxic agents (diuretics, NSAIDs, ACEIs, ARBs)
- Treat any precipitating infection with antibiotics
- IV albumin bolus: 1 g/kg/day (max 100 g/day) for 48 hours; continue at 20-60 g/day to maintain CVP 10-15 cm H₂O
Step 2: Vasopressor Therapy (added to albumin)
First-line:
Terlipressin (vasopressin V1 receptor analogue) - now FDA-approved in the US (confirmed by CONFIRM trial, Phase III RCT):
- Start at 1 mg IV every 4 hours
- Increase to 2 mg IV every 4 hours if creatinine does not fall by 25% by day 3
- Continue up to 14 days or until HRS reversal / LT
- Risk: respiratory failure - monitor oxygen saturation closely
- Evidence: higher HRS reversal rate vs. placebo; 2025 meta-analysis (PMID: 40207491) confirms superiority over placebo
Alternatives (if terlipressin unavailable or contraindicated):
- Norepinephrine: 0.1-0.7 mcg/kg/min IV infusion, titrate to MAP increase ≥10 mmHg; requires ICU monitoring; comparable efficacy to terlipressin (PMID: 38460713)
- Midodrine + Octreotide + Albumin (used widely in US prior to terlipressin approval):
- Midodrine: 2.5-5 mg oral TID, up to 15 mg TID (target MAP increase ≥15 mmHg)
- Octreotide: 100-200 mcg SC TID, or 25 mcg IV bolus then 25 mcg/hr infusion
- Now considered third-line per updated guidelines
Step 3: Bridging / Salvage Therapies
- TIPS (Transjugular Intrahepatic Portosystemic Shunt): reduces portal hypertension; can improve renal function in HRS-CKD/Type 2 but its role in HRS-AKI is less defined
- Renal replacement therapy: initiated if vasopressor treatment fails, as a bridge to LT
- Extracorporeal albumin dialysis (MARS): experimental; reduces blood ammonia and improves hemodynamics
Step 4: Definitive Treatment
-
Liver transplantation - the only definitive cure; renal function typically recovers after LT in both HRS-AKI and HRS-CKD; HRS is therefore a priority indication for transplantation
-
Sleisenger and Fordtran, Box 94.3 (Treatment of HRS); Harrison's 22E, p. 1380; Goldman-Cecil; Sabiston
Prognosis
- Without treatment, median survival of HRS-AKI is ~2 weeks
- HRS-CKD has a somewhat better prognosis but remains poor without transplantation
- With terlipressin + albumin, HRS reversal rates of ~35-45% have been reported in RCTs
- After successful liver transplantation, renal function recovery is typical
Recent Evidence Updates (2024-2026)
- PMID 38460713 (2024, Meta-Analysis): Terlipressin + albumin vs. norepinephrine + albumin - both are effective; terlipressin may have a marginal advantage in HRS reversal but carries higher respiratory adverse event risk.
- PMID 40207491 (2025, Meta-Analysis, Eur J Gastroenterol Hepatol): Terlipressin significantly improves HRS reversal rates in HRS-AKI across multiple RCTs, confirming its place as first-line therapy.
Summary Table
| Feature | HRS-AKI (Type 1) | HRS-CKD (Type 2) |
|---|---|---|
| Onset | Rapid (1-2 weeks) | Gradual |
| Trigger | SBP, sepsis, GI bleed | Refractory ascites |
| Creatinine | Rapidly rising | Stable, elevated |
| Prognosis | Very poor (~weeks untreated) | Moderate |
| Treatment | Terlipressin + albumin; LT | LT; TIPS |
Sources: Sleisenger and Fordtran's Gastrointestinal and Liver Disease; Harrison's Principles of Internal Medicine 22E; Goldman-Cecil Medicine; Sabiston Textbook of Surgery 14e; Recent meta-analyses PMID 38460713 & 40207491
This is a shared conversation. Sign in to Orris to start your own chat.