Cushing syndrome
Reading File
Finding Sources
Searching PubMed
"Cushing syndrome"[MeSH Terms] AND diagnosis
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Loading Image
Reading File
I now have comprehensive, well-sourced information to write a complete answer. Let me compile the full response.
Cushing Syndrome
Definition
Cushing syndrome is the clinical state resulting from prolonged, pathological exposure to excess glucocorticoids (hypercortisolism), regardless of the source. When hypercortisolism is specifically caused by an ACTH-secreting pituitary adenoma, the condition is called Cushing disease - a subset of Cushing syndrome.
- Campbell-Walsh-Wein Urology, p. 3134
- Henry's Clinical Diagnosis and Management by Laboratory Methods, p. 501
Etiology and Classification
The causes fall into three broad categories:
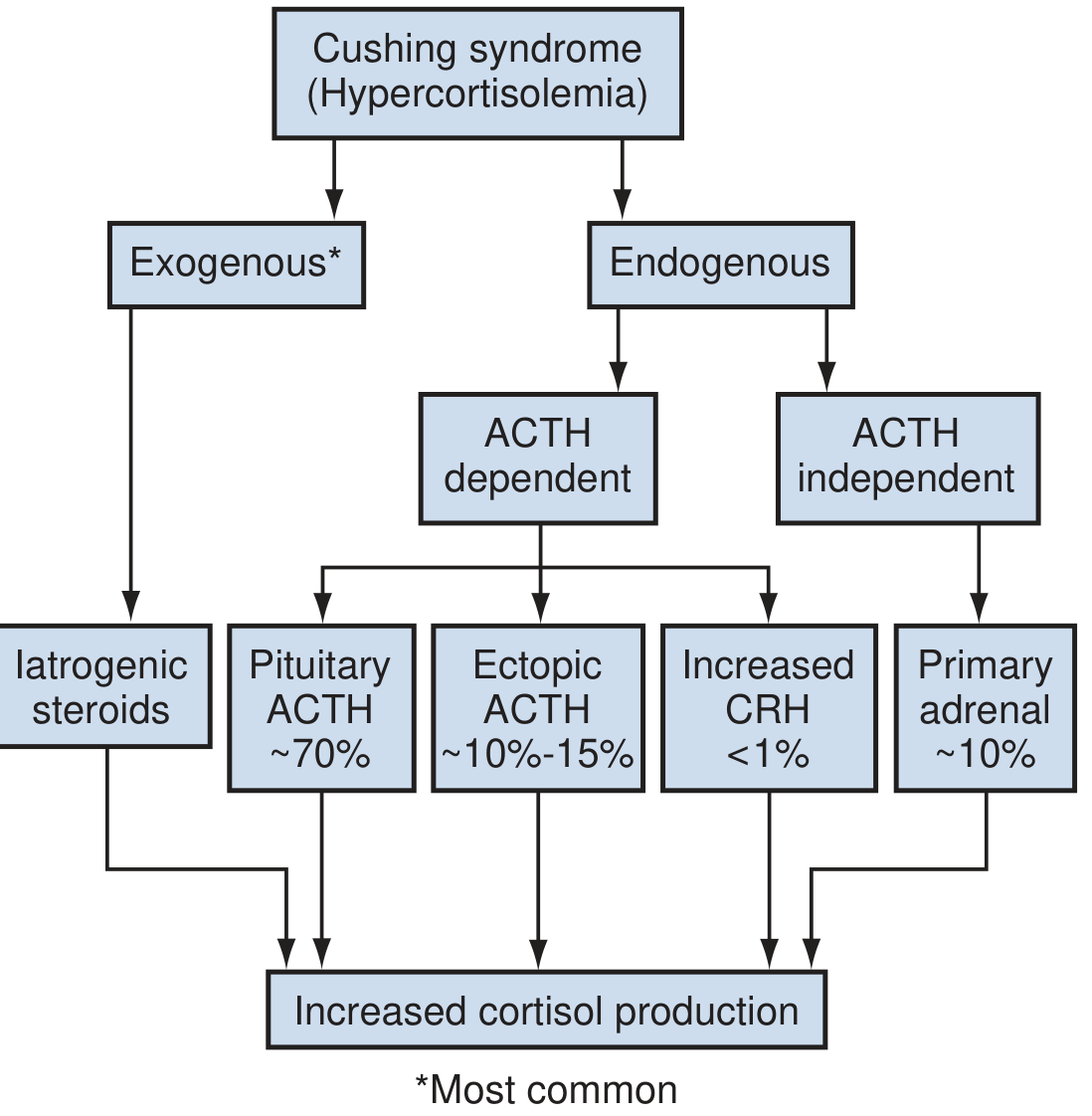
1. Exogenous (Iatrogenic) - Most Common Overall
Administration of synthetic glucocorticoids (oral, topical, inhaled, intranasal) is the most common cause in the Western world. Even low doses can produce the syndrome. A careful history is essential - patients may be unaware of steroid content in herbal preparations or nasal sprays.
2. Endogenous - ACTH-Dependent (80-85% of endogenous cases)
| Cause | Proportion | Notes |
|---|---|---|
| Cushing disease (pituitary ACTH adenoma) | ~70% of endogenous | Usually a microadenoma; F > M 2:1 |
| Ectopic ACTH syndrome | ~10-15% | Nearly always malignant tumors (small cell lung, carcinoid, etc.); higher ACTH → bilateral adrenal hyperplasia + hyperpigmentation |
| Ectopic CRH syndrome | <1% | Extremely rare |
3. Endogenous - ACTH-Independent (~10-20% of endogenous cases)
-
Adrenal adenoma or adrenal carcinoma - autonomous cortisol secretion suppresses the HPA axis; serum ACTH is low
-
Primary Pigmented Nodular Adrenocortical Disease (PPNAD) - occurs in 30% of patients with Carney complex; shows a paradoxical rise in UFC after dexamethasone
-
AIMAH (ACTH-independent macronodular adrenal hyperplasia)
-
Campbell-Walsh-Wein Urology, p. 3135-3137
Pathophysiology
The zona fasciculata of the adrenal cortex normally secretes up to 20 mg cortisol/day under control of the HPA axis:
- Hypothalamus releases CRH (under circadian control by the suprachiasmatic nucleus) → stimulates anterior pituitary corticotrophs
- Anterior pituitary releases ACTH (from POMC cleavage) → stimulates adrenal cortex
- Cortisol feeds back negatively to suppress both CRH and ACTH
Normal cortisol peaks in the early morning (~7-8 AM) and reaches a nadir at ~11 PM. In Cushing syndrome, this circadian rhythm is lost - the inability to suppress late-night cortisol is the earliest detectable abnormality.
- Campbell-Walsh-Wein Urology, p. 3134
Clinical Features
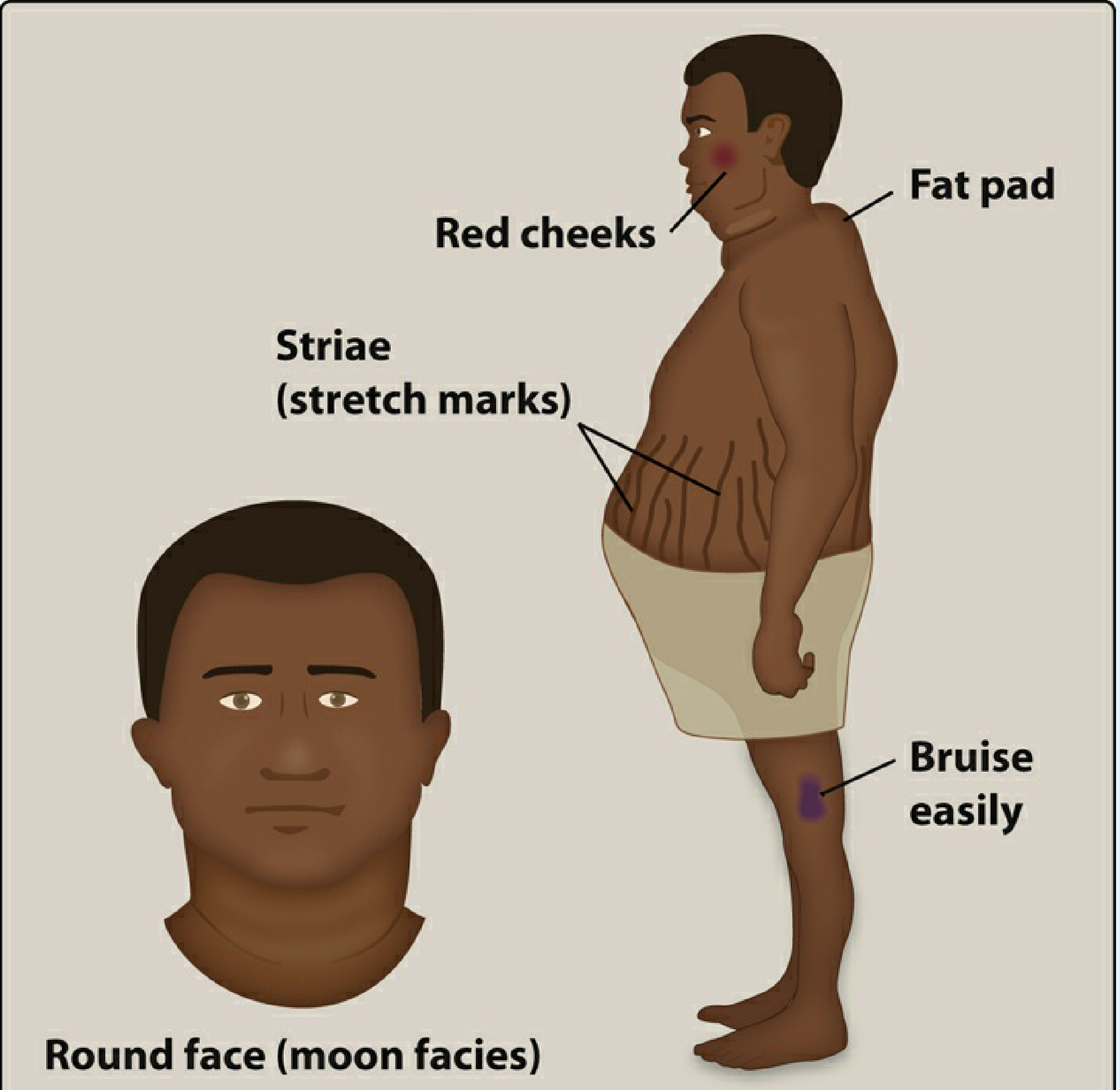
Classic Physical Findings
| System | Features |
|---|---|
| Fat redistribution | Central obesity, moon facies (round face), buffalo hump (dorso-cervical fat), supraclavicular fat pads; limbs spared |
| Skin | Purple/violaceous striae (abdomen, thighs, buttocks, arms); skin thinning and fragility; easy bruising; Liddle sign (skin peeling with tape removal); facial plethora |
| Hair/acne | Hypertrichosis (facial lanugo in women); scalp thinning; acne |
| Infections | Susceptibility to dermatophytes, Pityrosporum; opportunistic fungal infections |
| Musculoskeletal | Proximal muscle weakness; osteoporosis; vertebral fractures; kyphosis |
| Metabolic | Hypertension; hyperglycemia/diabetes mellitus (20% of patients); dyslipidemia |
| Reproductive | Loss of libido; menstrual irregularities in women |
| Neuro/psych | Depression, anxiety, cognitive impairment |
Women are affected 4x more frequently than men in non-iatrogenic cases. Peak onset is in the 20s-30s.
Ectopic ACTH syndrome presents differently: rapid onset, severe hypokalaemic alkalosis, hyperpigmentation (from high ACTH/MSH), and less classic cushingoid features because the disease course is often shorter.
- Andrews' Diseases of the Skin, p. 578
- Campbell-Walsh-Wein Urology, p. 3136
Diagnosis
Step 1: Screening (confirm hypercortisolism)
Three first-line screening tests - at least two abnormal tests are required:
| Test | Method | Notes |
|---|---|---|
| 24-hour urinary free cortisol (UFC) | Reflects unbound circulating cortisol; unaffected by CBG level | Upper normal: 110-138 nmol/24h; values >4x ULN are diagnostic; falsely low if GFR <30 mL/min |
| Overnight 1mg dexamethasone suppression test (DST) | 1 mg dexamethasone at 11 PM → check 8 AM cortisol | Cortisol <50 nmol/L (1.8 mcg/dL) rules out Cushing syndrome; preferred in renal impairment |
| Late-night salivary cortisol (MSC/LNSC) | 11 PM salivary cortisol (2 measurements) | Reflects loss of circadian nadir; convenient outpatient test |
Pseudo-Cushing syndrome (HPA hyperactivity without true Cushing syndrome) occurs in depression, alcoholism, anxiety, poorly controlled DM, and morbid obesity - causing false positives.
- Henry's Clinical Diagnosis, p. 501
- Lippincott Illustrated Reviews: Pharmacology, p. 875-876
Step 2: Confirm and Localize the Cause
Measure plasma ACTH:
- Low/suppressed ACTH → ACTH-independent (adrenal source) → CT/MRI adrenals
- Normal/elevated ACTH → ACTH-dependent → distinguish pituitary vs. ectopic
For ACTH-dependent disease:
-
Pituitary MRI (note: ~50% of Cushing disease patients have no visible adenoma on MRI; 10% of normal people have incidental pituitary abnormalities)
-
High-dose DST (8 mg overnight): suppression suggests pituitary source (Cushing disease); no suppression suggests ectopic - but limited reliability
-
Inferior petrosal sinus sampling (IPSS) after CRH stimulation = gold standard for distinguishing Cushing disease from ectopic ACTH. Central:peripheral ACTH ratio >2 (basal) or >3 (post-CRH) = pituitary source
-
Chest CT/octreotide scan to find ectopic source
-
Campbell-Walsh-Wein Urology, p. 3137-3139
Laboratory Findings Summary
- Elevated serum cortisol, UFC, or late-night salivary cortisol
- Loss of circadian rhythm of ACTH and cortisol
- Failure to suppress cortisol with dexamethasone
Treatment
Treatment depends on the underlying cause, and requires a multidisciplinary team.
Exogenous Cushing Syndrome
- Gradual tapering of exogenous glucocorticoids (never abrupt cessation - risk of adrenal insufficiency and steroid withdrawal syndrome)
- Allow HPA axis recovery over weeks to months
Cushing Disease (Pituitary Adenoma)
- Trans-sphenoidal surgical resection is the first-line treatment; cure rate ~60-80%
- ~25% relapse on long-term follow-up
- Post-op: expect transient adrenal insufficiency requiring glucocorticoid replacement for up to 1 year
- Failed surgery: options include reoperation, stereotactic radiation (risk: delayed response, hypopituitarism), or bilateral adrenalectomy
- Bilateral adrenalectomy: rapid definitive cure, but requires lifelong steroid replacement; risk of Nelson syndrome (progressive ACTH-secreting pituitary tumor growth post-adrenalectomy due to loss of cortisol feedback)
Ectopic ACTH Syndrome
- Resect the primary tumor when possible
- If unresectable: medical adrenal blockade with ketoconazole, metyrapone, mitotane, or etomidate (for acute crisis); bilateral adrenalectomy as last resort
Adrenal Cushing Syndrome (Adenoma/Carcinoma)
- Unilateral or bilateral laparoscopic adrenalectomy
- Adrenal carcinoma: adrenalectomy + mitotane (adjuvant); poor prognosis
Medical Therapy (adjunctive/bridging)
| Drug | Mechanism |
|---|---|
| Ketoconazole | Inhibits 11β-hydroxylase and cholesterol side-chain cleavage |
| Metyrapone | Blocks 11β-hydroxylase |
| Mitotane | Adrenolytic; used in adrenal carcinoma |
| Pasireotide | Somatostatin analogue; reduces ACTH in Cushing disease |
| Mifepristone | Glucocorticoid receptor antagonist; useful when surgery is not possible |
- Campbell-Walsh-Wein Urology, p. 3139-3141
Pseudo-Cushing Syndrome
Mimics Cushing syndrome clinically and biochemically but is not due to a primary HPA axis pathology. Causes: alcoholism (increased cortisol secretion + reduced cortisol metabolism by hepatic damage), severe depression, anxiety disorders, poorly controlled DM, morbid obesity.
The CRH stimulation test (with low-dose DST) helps distinguish: in true Cushing syndrome, CRH raises cortisol despite prior dexamethasone; in pseudo-Cushing, it does not.
- Comprehensive Clinical Nephrology, p. 1504
Key Points Summary
| Feature | Detail |
|---|---|
| Most common cause | Iatrogenic (exogenous steroids) |
| Most common endogenous cause | Cushing disease (pituitary ACTH microadenoma, ~70%) |
| Gold standard to distinguish pituitary vs. ectopic ACTH | Inferior petrosal sinus sampling (IPSS) |
| First-line screening tests | 24h UFC, overnight DST, late-night salivary cortisol |
| Earliest abnormality | Loss of late-night cortisol suppression |
| Most specific skin finding | Wide purple striae + easy bruising + skin thinning |
| Treatment of Cushing disease | Trans-sphenoidal surgery (60-80% cure) |
| Risk after bilateral adrenalectomy for Cushing disease | Nelson syndrome |
Recent evidence note: A 2024 systematic review and meta-analysis (PMID 38888685) highlights that distinguishing true Cushing syndrome from non-neoplastic hypercortisolism (pseudo-Cushing) remains challenging with standard tests - consistent with the textbook guidance above that multiple tests and clinical context are needed.
This is a shared conversation. Sign in to Orris to start your own chat.