I now have comprehensive content, textbook data, and multiple high-quality labeled images to compose a thorough educational response. Let me compile the full answer.
CT Neck Angiography & Venography: Complete Arterial and Venous Anatomy
OVERVIEW IMAGE: Aortic Arch to Intracranial Vessels
This CTA MIP reconstruction shows the full vascular anatomy from the aortic arch through the intracranial circulation - the foundational overview image for neck CTA interpretation:
PART 1: CT NECK ANGIOGRAPHY (ARTERIAL ANATOMY)
1. AORTIC ARCH
The aortic arch gives rise to three major branches in the normal configuration (present in ~70% of individuals):
| Branch | Side | Origin |
|---|
| Brachiocephalic trunk (Innominate artery) | Right | First branch, gives right CCA + right subclavian |
| Left common carotid artery | Left | Second branch, directly from arch |
| Left subclavian artery | Left | Third branch |
On CTA: The arch sweeps from the ascending to descending aorta. Begin axial review at the level of the arch. The brachiocephalic trunk is the most anterior/right-sided vessel at this level.
Key variants to know:
- Bovine arch: left CCA arises from the brachiocephalic trunk (~13-15%) - most common variant
- Aberrant right subclavian artery (arteria lusoria): retroesophageal course (~0.5-2%)
- Left vertebral artery arising directly from arch (~2-5%)
2. COMMON CAROTID ARTERIES (CCA)
Right CCA: Arises from the brachiocephalic trunk, behind the right sternoclavicular joint.
Left CCA: Arises directly from the aortic arch; has a short mediastinal segment before entering the neck.
Course: Both CCAs ascend in the carotid sheath, medial to the internal jugular vein, with the vagus nerve posteriorly. They give no branches in the neck.
Wall assessment on CTA:
- Normal wall thickness: 1-2 mm, smooth internal and external contour
- Atheroma: calcified or soft plaque causing luminal irregularity
- Dissection: intimal flap, double lumen, or mural hematoma (crescentic hypodensity in wall on non-contrast; false lumen often slightly smaller caliber)
Bifurcation level: Normally at the upper border of thyroid cartilage, corresponding to the C3-C4 intervertebral disc level (range C2-C5). - Fischer's Mastery of Surgery, p. 1113
3. CAROTID BIFURCATION
The bifurcation is the most critical segment to assess on neck CTA. The ICA and ECA diverge here:
| Feature | ICA | ECA |
|---|
| Initial position | Posterolateral | Anteromedial |
| Size | Larger | Smaller |
| Branches in neck | None | Multiple |
| Carotid bulb | Present at origin | Absent |
Carotid bulb (sinus): A normal focal dilation at the proximal ICA. Contains baroreceptors. This is the most common site for atherosclerotic plaque. On CTA, the bulb appears as smooth luminal widening - not to be confused with pathological aneurysm.
Carotid body: Ovoid paraganglioma-prone tissue at the bifurcation; splays the ICA and ECA (lyre sign) when enlarged.
4. INTERNAL CAROTID ARTERY (ICA)
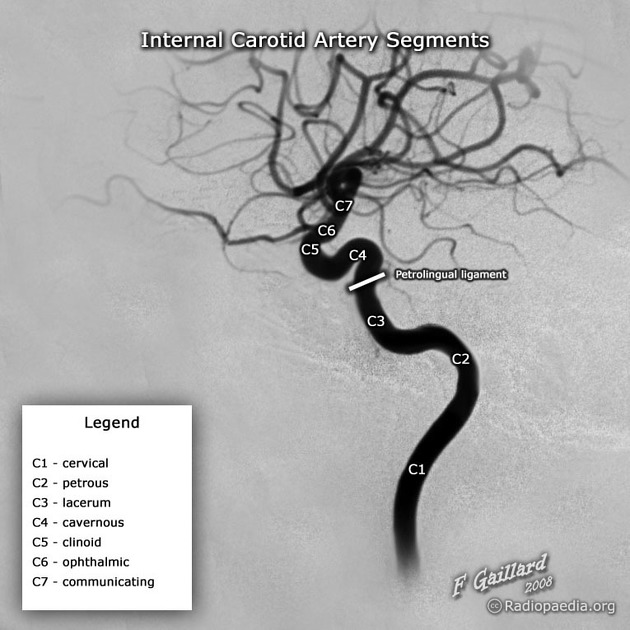
The ICA has no branches in the neck. The most widely used segmental classification is Bouthillier (1996) with 7 segments (C1-C7):
ICA Segment Diagram (DSA, labeled):
Source: Radiopaedia.org (F. Gaillard)
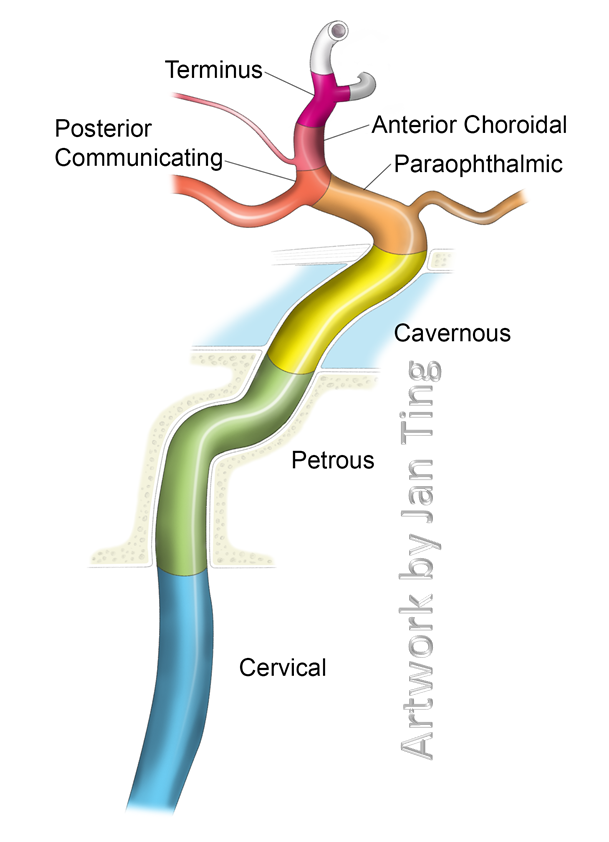
ICA Segment Illustration (color-coded):
Source: neuroangio.org (artwork by Jan Ting)
ICA Segments - Detail:
| Segment | Code | Location | Key Points |
|---|
| Cervical | C1 | From carotid bulb to skull base (carotid canal) | Longest, most accessible; no branches; course is straight in normal |
| Petrous | C2 | Within petrous bone carotid canal | Vertical then horizontal turn; caroticotympanic artery (small branch) |
| Lacerum | C3 | Above foramen lacerum, within fibrocartilage | Very short; no branches; connects petrous to cavernous |
| Cavernous | C4 | Within cavernous sinus | S-shaped (carotid siphon); branches: meningohypophyseal trunk, inferolateral trunk |
| Clinoid | C5 | Between proximal and distal dural rings | Very short |
| Ophthalmic (Supraclinoid) | C6 | Intradural, above dural ring | Gives ophthalmic artery and superior hypophyseal artery |
| Communicating (Terminal) | C7 | To ICA bifurcation | Gives posterior communicating and anterior choroidal arteries; terminates as MCA + ACA |
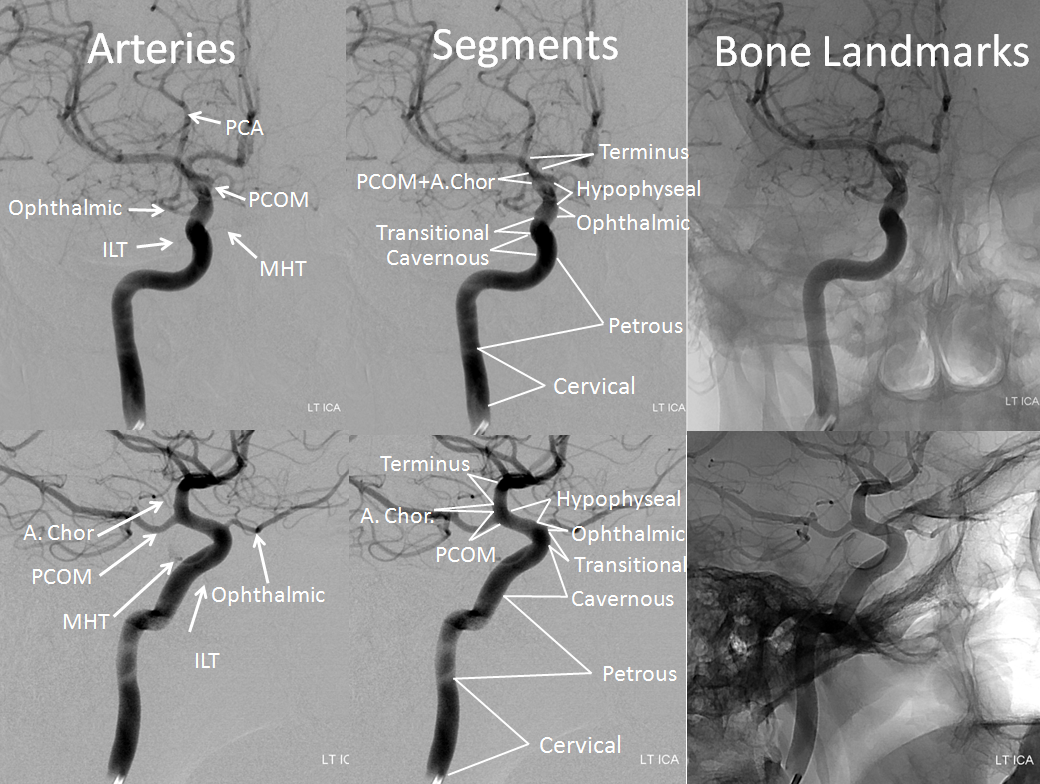
DSA/Angiographic image showing ICA segments with branches and bone landmarks:
Source: neuroangio.org
What to Assess on CTA:
- Stenosis: NASCET method (compare residual lumen to ICA above bulb). Hemodynamically significant at >50%, surgical threshold at >70%
- Occlusion: Absent enhancement; compare to contralateral side
- Dissection: Mural hematoma (crescent sign), intimal flap, pseudolumen, pearl-and-string pattern; may extend from C1 into petrous segment
- Pseudoaneurysm: Focal saccular outpouching, often at prior dissection site or trauma
- Fibromuscular dysplasia (FMD): String-of-beads appearance, most common in C1-C2; young women; bilateral in 60%; non-atherosclerotic
5. EXTERNAL CAROTID ARTERY (ECA)
The ECA initially lies anteromedial to the ICA, then rotates anterolateral superiorly. It terminates at the neck of the mandible (within the parotid gland) as the superficial temporal artery and maxillary artery. - Fischer's Mastery of Surgery, p. 1113
ECA Branches (mnemonic: Some Angry Ladies Fight Over PMS):
| Group | Branch | Territory |
|---|
| Anterior | Superior thyroid artery | Thyroid gland, superior larynx |
| Anterior | Lingual artery | Tongue, floor of mouth |
| Anterior | Facial artery | Face (labial, nasal branches) |
| Medial | Ascending pharyngeal artery | Pharynx, dura, tympanic cavity |
| Posterior | Occipital artery | Posterior scalp, SCM muscle |
| Posterior | Posterior auricular artery | Ear, scalp behind auricle |
| Terminal | Maxillary artery | Deep face, meninges (middle meningeal) |
| Terminal | Superficial temporal artery | Temple, scalp, parotid |
Superior thyroid artery arises at the level of the hyoid bone as the first anterior branch. - Color Atlas of Human Anatomy Vol 2, p. 834
On CTA: ECA branches are identified by their small caliber and branching pattern. The superior thyroid artery is the lowest visible branch, coursing inferiorly toward the thyroid. The lingual artery dips medially toward the tongue. The facial artery takes a tortuous course over the mandible. The maxillary and superficial temporal arteries are the dominant terminal branches seen in the upper neck/parotid region.
6. VERTEBRAL ARTERIES (VA)
The vertebral artery arises from the first part of the subclavian artery bilaterally. It is divided into four segments:
| Segment | Course | Key Landmarks |
|---|
| V1 (Pre-foraminal) | Origin (subclavian) → C6 transverse foramen | Posterior to common carotid; passes behind anterior scalene muscle |
| V2 (Foraminal) | C6 transverse foramen → C2 transverse foramen | Protected in bony foramina; accompanied by venous plexus and sympathetic fibers |
| V3 (Atlantoaxial / Extra-dural) | C2 → dura at foramen magnum | Makes two S-curves around atlas; most mobile, most vulnerable to trauma and dissection |
| V4 (Intradural) | Foramen magnum → basilar artery junction | Gives PICA; two VAs join to form basilar artery at pontomedullary junction |
- Harrison's Principles of Internal Medicine 22E; Adams and Victor's Principles of Neurology, 12th Ed.
On CTA:
- V1: Look for origin stenosis; the right VA arises from the subclavian distal to the thyrocervical trunk
- V2: Seen within the transverse foramina - compare caliber bilaterally (left VA dominant in ~50%)
- V3: The "exit loop" at C2 is visible just posterior to the C1-C2 joint
- V4: Visible entering the foramen magnum, converging toward the basilar artery
Key variants:
- Left VA arises directly from aortic arch (~2-5%)
- VA hypoplasia (diameter <2 mm): usually right side; important before posterior fossa surgery
- Fenestration of VA (uncommon; associated with aneurysm)
7. SUBCLAVIAN ARTERIES
- Right subclavian: Arises from the brachiocephalic trunk, behind the right sternoclavicular joint
- Left subclavian: Arises directly from the aortic arch (third branch)
- Both pass posterior to the anterior scalene muscle
Branches (proximal to distal):
- Vertebral artery (first branch)
- Internal thoracic (mammary) artery
- Thyrocervical trunk (gives inferior thyroid, suprascapular, transverse cervical arteries)
- Costocervical trunk (gives supreme intercostal, deep cervical)
CTA assessment:
- Subclavian steal syndrome: >70% stenosis of proximal subclavian (pre-vertebral origin) causes retrograde flow in ipsilateral VA (best shown on CTA + Doppler or DSA)
- Aneurysm: Fusiform dilation, often post-stenotic or in thoracic outlet syndrome
- Aberrant right subclavian (arteria lusoria): Arises as fourth aortic arch branch, courses behind the esophagus; can cause dysphagia lusoria
PART 2: CT NECK VENOGRAPHY (VENOUS ANATOMY)
VENOUS ANATOMY DIAGRAM (Lateral View):
Source: Radiopaedia.org
SUPERFICIAL VEINS
External Jugular Vein (EJV)
- Formed by the posterior auricular vein and the posterior division of the retromandibular vein behind the ear
- Descends obliquely across the sternocleidomastoid muscle (SCM), superficial to it
- Pierces the deep cervical fascia and drains into the subclavian vein
- Receives: posterior external jugular, transverse cervical, suprascapular veins
- On CTA/CTV: Visible as a thin vessel crossing SCM; larger and more prominent when the patient performs Valsalva
Anterior Jugular Vein (AJV)
- Arises near the chin (mental region), descends near the midline
- Connects to the opposite side via the jugular venous arch (suprasternal)
- Drains into the external jugular vein or directly into the subclavian vein
- Highly variable; may be paired or a single midline vessel
DEEP VEINS
Internal Jugular Vein (IJV)
The IJV is the dominant venous drainage pathway of the brain, face, and neck.
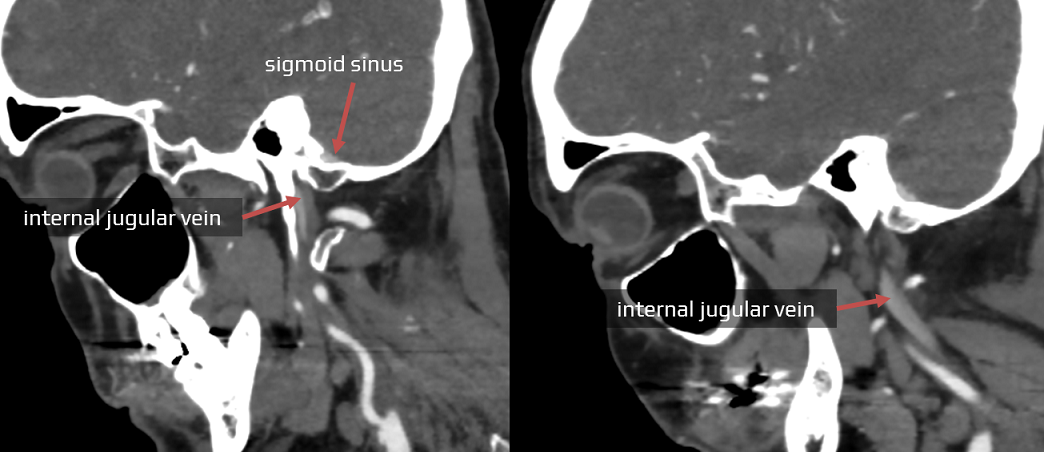
Origin: Continuous with the sigmoid sinus at the jugular foramen (posterior compartment - pars vascularis). The dilation at this point is the superior bulb of the IJV (jugular bulb), occupying the jugular fossa of the temporal bone.
Course: Descends vertically in the carotid sheath, lateral to the CCA and ICA, with the vagus nerve posteriorly. Ends behind the sternal end of the clavicle where it joins the subclavian vein to form the brachiocephalic vein. A second dilation just proximal to this junction is the inferior bulb of the IJV.
On CT: The IJVs are frequently asymmetric in caliber - this is normal (right side often larger, due to right-sided dominance of transverse sinus drainage). Valves visible in the IJV should not be mistaken for thrombus. Heterogeneous enhancement from mixing of opacified and non-opacified blood is also normal.
CT image showing IJV - sigmoid sinus relationship:
Axial CT showing jugular foramen anatomy:
Major Tributaries of the IJV:
| Tributary | Drains |
|---|
| Facial vein (common facial vein) | Face, formed by union of anterior facial vein + anterior branch of retromandibular vein |
| Lingual vein | Tongue, sublingual glands |
| Superior thyroid vein | Upper thyroid lobe, larynx |
| Middle thyroid vein | Mid-thyroid (drains directly into IJV, no valve) |
| Pharyngeal veins | Pharyngeal venous plexus |
| Occipital vein | Posterior scalp (variable; may drain to vertebral vein instead) |
Vertebral Vein
- Begins in the suboccipital triangle, descends through the transverse foramina of C1-C6 alongside the vertebral artery
- Drains into the brachiocephalic vein (not the IJV)
- The vertebral venous plexus is a rich paravertebral network; a pathway for metastatic spread (Batson's plexus)
Deep Cervical Vein
- Runs in the posterior neck alongside the deep cervical artery
- Drains the posterior neck muscles
- Drains into the vertebral or brachiocephalic vein
CENTRAL VEINS
Brachiocephalic Veins (Innominate Veins)
- Formed by the union of the IJV + subclavian vein at the venous angle (Pirogoff angle), behind the sternoclavicular joint
- Right brachiocephalic vein: Short (~2.5 cm), nearly vertical
- Left brachiocephalic vein: Longer (~6 cm), horizontal course across the superior mediastinum, anterior to the aortic arch branches
- Both join to form the SVC
Superior Vena Cava (SVC)
- Formed behind the right first costal cartilage
- Receives the azygos vein posteriorly before entering the right atrium
- On CTA: Look for opacification defects suggesting SVC thrombosis; extrinsic compression (mass, lymph nodes); SVC syndrome
DURAL VENOUS OUTFLOW
The pathway from intracranial venous drainage to the IJV:
Superior sagittal sinus + Inferior sagittal sinus
↓
Straight sinus (via great vein of Galen)
↓
Confluence of sinuses (Torcular Herophili)
↓
Transverse sinuses (bilateral, within tentorium)
↓
Sigmoid sinuses (S-shaped, posterior fossa)
↓
Jugular bulb (at jugular foramen)
↓
Internal jugular vein (cervical course)
↓
Brachiocephalic vein → SVC → Right atrium
Dural sinus diagram (axial view from above):
Source: Radiopaedia.org
VENOUS PATHOLOGY - WHAT TO ASSESS
| Finding | CTV Appearance |
|---|
| Thrombosis | Filling defect (hypodense on contrast CT); empty delta sign (rim enhancement around thrombus) |
| Compression | Extrinsic narrowing by adjacent mass, lymph node, or hematoma |
| Stenosis | Focal luminal narrowing - check for collateral formation |
| Collateral veins | Engorgement of external jugular, anterior jugular, vertebral veins; perivertebral plexus |
| Congenital variants | High-riding jugular bulb (extends above lower margin of IAC), jugular bulb diverticulum, duplicated IJV, IJV hypoplasia |
CONGENITAL VASCULAR VARIANTS (Summary)
| Variant | Vessel | Frequency | Clinical Significance |
|---|
| Bovine arch | Aortic arch | ~15% | Left CCA shares brachiocephalic trunk origin |
| Aberrant right subclavian | Subclavian | ~0.5% | Dysphagia lusoria; retroesophageal |
| Left VA from aortic arch | Vertebral | ~2-5% | Between left CCA and left subclavian |
| Hypoplastic VA | Vertebral | ~5-10% | Usually right; vertebrobasilar insufficiency risk |
| Fenestrated VA | Vertebral | Rare | Associated with aneurysm |
| Persistent hypoglossal artery | ICA-basilar | <0.1% | Primitive carotid-basilar anastomosis |
| High-riding jugular bulb | Jugular bulb | ~5% | May mimic middle ear mass; pulsatile tinnitus |
| IJV hypoplasia | IJV | Variable | Compensatory contralateral enlargement |
| Duplicated IJV | IJV | Rare | Usually right-sided |
CTA READING APPROACH (Search Pattern)
- Non-vascular structures first: Thyroid, lymph nodes, soft tissues, lungs, brain, bones
- Neck arteries (anterior, right to left):
- Right CCA → bifurcation → ICA (to skull base) → ECA
- Left CCA → bifurcation → ICA → ECA
- Neck arteries (posterior):
- Right VA: subclavian origin → V1 → V2 → V3 → skull base
- Left VA: same pattern
- Head arteries (if included): ICA siphon → MCA → ACA → posterior circulation → basilar → PCA
- Venous phase / CTV (if obtained): Sigmoid sinuses → jugular bulbs → IJVs → brachiocephalic veins → SVC
CTA technique note: Scan from aortic arch to vertex (caudocranial direction preferred to minimize venous contamination). Bolus tracking at the aortic arch. Delay ~15-20 seconds from bolus arrival for arterial phase. CTV uses a 45-50 second delay to ensure venous opacification. -
Radiopaedia CTA protocol
Sources: Fischer's Mastery of Surgery 8th ed.; Grainger & Allison's Diagnostic Radiology; Harrison's Principles of Internal Medicine 22E; Adams and Victor's Principles of Neurology 12th ed.; Radiopaedia.org; neuroangio.org; learnneuroradiology.com