I now have comprehensive content from all sources. Let me compose the full Crohn disease answer.
Crohn Disease (Regional Enteritis)
Sources: Nelson Textbook of Pediatrics 2024, Chapter 382 (attached); Goldman-Cecil Medicine; Sleisenger & Fordtran's Gastrointestinal and Liver Disease
Definition & Overview
Crohn disease is an idiopathic, chronic inflammatory disorder that can affect any region of the alimentary tract from mouth to anus. Unlike ulcerative colitis, which is confined to the colon and is continuous, Crohn disease is:
- Transmural (full-thickness bowel wall inflammation)
- Segmental/discontinuous (skip lesions — normal bowel between diseased segments)
- Capable of fistula, stricture, and abscess formation
- Not curable by medical or surgical therapy
The most common site of involvement is the ileocecal region.
Epidemiology
| Feature | Detail |
|---|
| Peak age of onset | 15–30 yr (1st peak); 2nd peak in 7th decade |
| Sex | F:M = 1.2:1 |
| Pediatric incidence | 4.56/100,000; prevalence 43/100,000 children |
| Increasing incidence | Rising globally; linked to industrialized/Western lifestyle |
| Family risk | 7–30%; risk higher than UC for first-degree relatives |
| Monozygotic twin concordance | 36% (vs. 16% for UC) |
| ASCA positive | 40–70% (vs. <15% in UC) |
| pANCA | <20% positive (helps differentiate from UC) |
Pathogenesis
- Dysregulated immune response to environmental/microbial factors in a genetically susceptible host
- NOD2 gene (on chromosome 16): first identified IBD gene; involved in bacterial recognition, NF-κB activation, autophagy
- Other key genes: IL10, IL10RA, IL10RB, IRGM, ATG16L1, IL23R
- Cigarette smoking increases risk (opposite of UC)
- Gut microbiota play a central role; alterations linked to increasing IBD incidence
- Activated cytokines (especially TNF-α, IL-12, IL-23) drive the inflammatory cascade — these are therapeutic targets
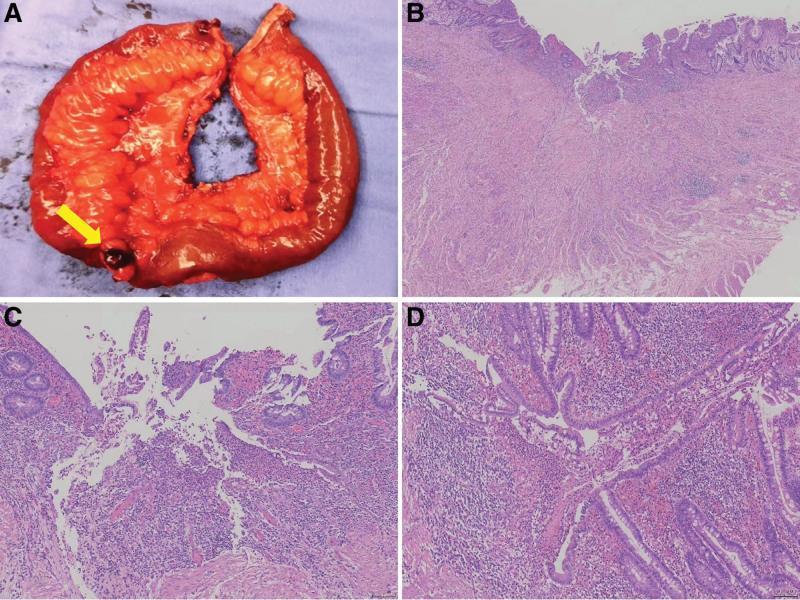
Gross & Microscopic Pathology
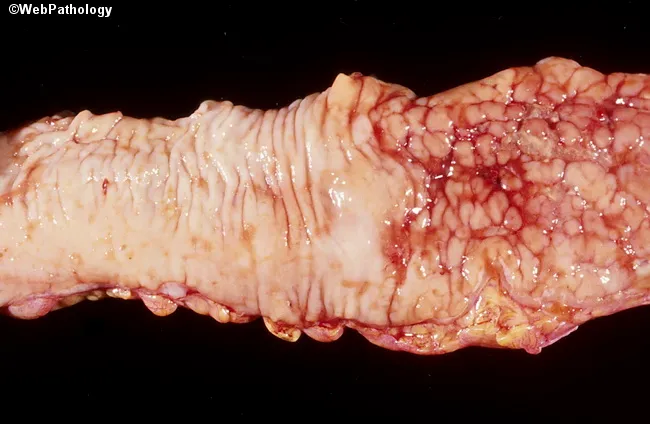
Gross:
- Aphthous ulcers (earliest lesion) → progress to deep, discrete, serpiginous ulcers
- Cobblestone appearance: longitudinal ulcers crossed by transverse fissures create a "cobblestone" mucosa
- Skip lesions: diseased segments separated by normal bowel
- Transmural inflammation: extends through all wall layers — enables fistula and abscess formation
- Fat creeping/wrapping on the serosal surface (mesenteric fat encircles the bowel)
- Chronic disease: fibrotic strictures (~30% develop fistulas over their disease course)
- Can occur mouth to anus; most common site = ileocecal region
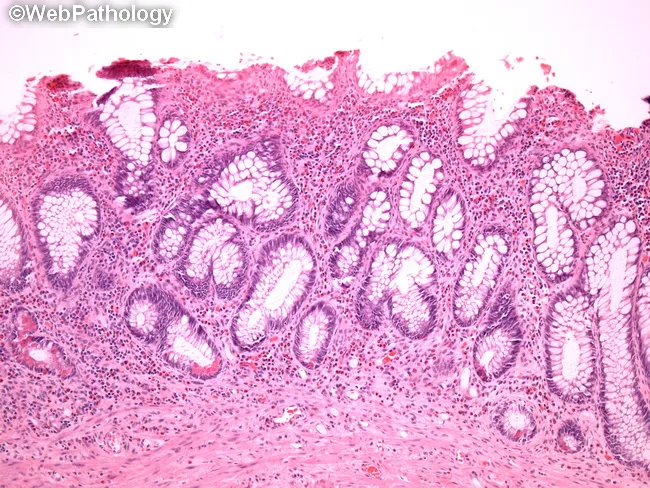
Microscopic (histopathology):
- Early: acute inflammatory infiltrate, cryptitis, crypt abscesses (similar to UC early on)
- Later: lymphocytic infiltrate, crypt architectural distortion (branching and shortening)
- Noncaseating granulomas — the hallmark; found in:
- Up to 15% of endoscopic biopsy specimens
- Up to 70% of surgical specimens
- Not unique to Crohn but strongly supportive when present
- Transmural inflammation — identified only in surgical specimens (not endoscopic biopsies)
Montreal Classification
Location (L):
| Class | Location |
|---|
| L1 | Terminal ileum (± limited cecal disease) |
| L2 | Colonic |
| L3 | Ileocolonic |
| L4 | Upper GI (modifier added to L1–L3) |
Behavior (B):
| Class | Behavior |
|---|
| B1 | Inflammatory (non-stricturing, non-penetrating) |
| B2 | Stricturing |
| B3 | Penetrating (fistulizing) |
| p | Perianal modifier (added to any B category) |
Disease phenotypes evolve over time: inflammatory → stricturing and/or penetrating as disease duration increases.
Clinical Manifestations
Presentation Patterns
Crohn disease can be characterized as inflammatory, stricturing, or penetrating:
Inflammatory pattern (B1):
- Diarrhea (often without blood — only 25% have GI bleeding)
- Abdominal pain (especially right lower quadrant — classic)
- Low-grade fever, malaise, fatigue
- Weight loss, anorexia
- Only 25% initially have the classic triad of diarrhea + weight loss + abdominal pain
Stricturing pattern (B2):
- Cramping postprandial abdominal pain, borborygmus
- Intermittent abdominal distention
- Partial small bowel obstruction
- Gurgling sensation when intestinal contents pass through a narrowed segment
Penetrating pattern (B3):
| Fistula Type | Manifestations |
|---|
| Enteroenteric/Enterocolonic | Often asymptomatic; may cause malabsorption or bacterial overgrowth |
| Enterovesical (to bladder) | Pneumaturia, fecaluria, recurrent UTI |
| Enterovaginal | Feculent vaginal discharge, dyspareunia |
| Enterocutaneous | Feculent discharge through skin; often at prior surgical sites |
| Perianal | Perianal abscess (painful), perianal fistulas (purulent drainage), large skin tags (1–3 cm), deep fissures |
Psoas abscess: secondary to intestinal fistula → hip pain, decreased hip extension (psoas sign), fever.
Systemic Features (more common than in UC)
- Growth failure in pediatric patients: height velocity decreased in ~88% of prepubertal patients — often precedes GI symptoms by 1–2 years
- Weight loss and malnutrition
- Delayed bone maturation and delayed sexual development/puberty
- Primary or secondary amenorrhea
- Digital clubbing
- Fever and malaise
Extraintestinal Manifestations
More common in Crohn disease than UC (especially with colonic involvement):
| Manifestation | Notes |
|---|
| Peripheral arthritis | Most common EIM; nondeforming; correlates with bowel activity |
| Oral aphthous ulcers | Crohn-specific; not seen in UC |
| Erythema nodosum | Correlates with bowel activity |
| Pyoderma gangrenosum | Both; correlates less with bowel activity |
| Episcleritis/uveitis | 5–15% |
| Ankylosing spondylitis | HLA-B27 associated; does NOT correlate with bowel activity |
| Primary sclerosing cholangitis | Also associated with UC |
| Nephrolithiasis | Calcium oxalate (fat malabsorption → increased oxalate absorption); uric acid (volume depletion) |
| Cholelithiasis | Bile acid depletion from terminal ileal disease/resection |
| Vitamin B12 deficiency | Terminal ileal disease or resection (>100 cm) |
| Osteoporosis/osteomalacia | Chronic malnutrition + corticosteroids |
| Thromboembolic disease | DVT, PE, cerebrovascular events |
| Metastatic Crohn disease | Noncaseating granulomas in skin, not contiguous with active bowel disease |
Diagnosis
Diagnosis requires: typical clinical features + ruling out infectious mimics + demonstrating chronicity (endoscopic + radiologic + histologic).
Laboratory Findings
- CBC: anemia (iron deficiency most common), thrombocytosis (marker of active inflammation)
- ESR and CRP: often elevated but can be normal
- Fecal calprotectin and lactoferrin: more sensitive/specific than serum markers; reflect mucosal neutrophil activity
- Serum albumin: low with active disease or protein-losing enteropathy
- Vitamin B12: low with terminal ileal involvement
- ASCA (anti-Saccharomyces cerevisiae antibodies): positive in 40–70% of Crohn patients (IgA + IgG ASCA highly specific for Crohn: 89–100% specificity)
- pANCA: negative (positive in UC)
ASCA+/pANCA− combination: sensitivity 55%, specificity 93% for Crohn disease
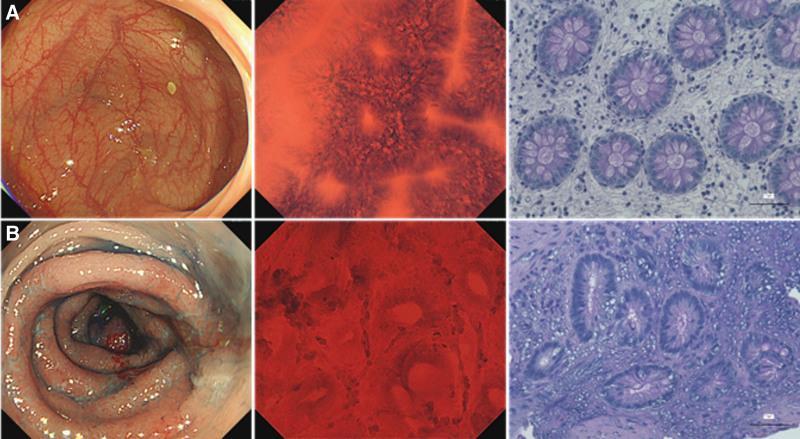
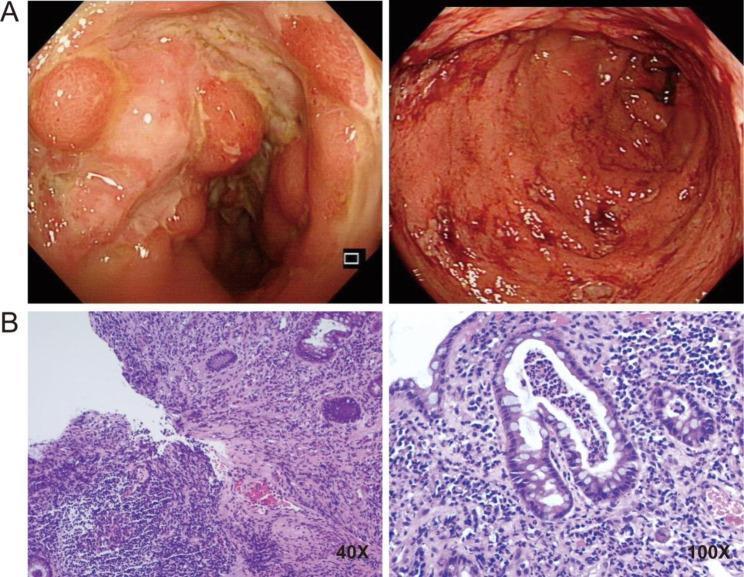
Endoscopy
Colonoscopy with terminal ileal intubation + esophagogastroduodenoscopy:
- Patchy erythema, friability, aphthous ulcers, linear ulcers, cobblestone pattern, nodularity, strictures
- Biopsies: noncaseating granulomas (pathognomonic if present), chronic inflammatory changes
- Transmural inflammation only visible in surgical specimens
Video capsule endoscopy (VCE):
- Evaluates small bowel mucosa not accessible by standard endoscopy
- CONTRAINDICATED in stricturing disease (risk of capsule retention)
- Patency capsule should be used first if stricture is suspected
Radiology
Plain abdominal X-ray:
- Normal, or shows partial small bowel obstruction, thumbprinting of the colon wall (submucosal edema)
Upper GI with small bowel follow-through (SBFT):
- Aphthous ulcers, thickened/nodular folds, luminal narrowing/strictures
- Linear ulcers → cobblestone appearance
- Separation of bowel loops (mesenteric thickening/fat)
CT Enterography / MR Enterography (preferred):
- Mural hyperenhancement, mural thickening, "comb sign" (engorged peri-enteric vessels resembling comb teeth — from hypervascularity adjacent to inflamed loop)
- Detects extraluminal complications: intraabdominal abscess, fistulas, perianal involvement
- MRI is preferred (no ionizing radiation) especially in children; MR pelvis for perianal disease
- Bowel ultrasound: can show mural thickening and hyperemia; no radiation
PET/MRI: identifies areas of active intestinal and extraintestinal inflammation (discontinuous FDG uptake, bowel wall thickening, edema, adjacent fibrofatty proliferation)
Disease Activity Scoring
Crohn Disease Activity Index (CDAI):
- Composite of subjective symptoms + objective findings
- Remission: CDAI < 150
- Response: decrease in CDAI ≥ 100 points
- Used primarily in clinical trials; symptoms alone do not always correlate with endoscopic activity
Lémann Score: quantifies cumulative intestinal damage (strictures, fistulas, resections) over time — tracks disease progression.
Differential Diagnosis
| Presenting Feature | Consider |
|---|
| RLQ pain ± mass | Appendicitis, Yersinia infection, lymphoma, intussusception, mesenteric adenitis, Meckel diverticulum |
| Chronic periumbilical pain | IBS, lactose intolerance, peptic disease, constipation |
| Bloody diarrhea | Infectious colitis (Campylobacter, Salmonella, Shigella, E. coli O157:H7), HUS, C. difficile |
| Growth failure | Growth hormone deficiency, celiac disease, Turner syndrome, anorexia nervosa |
| Perianal disease | Streptococcal infection, fissure, hemorrhoid, condyloma |
| Arthritis preceding GI sx | Juvenile idiopathic arthritis |
| Small bowel disease mimics | Yersinia enterocolitis (very similar!), GI tuberculosis, bowel lymphoma, Celiac + Giardia, foreign body perforation |
Treatment
Goals: relieve symptoms, prevent complications (anemia, growth failure, stricture, fistula), prevent relapse, minimize corticosteroid exposure, achieve mucosal healing ("deep remission").
Step-up vs. Top-down Approach
- Step-up (traditional): start with 5-ASA/steroids; escalate if needed
- Top-down (increasingly preferred, especially in pediatrics): start with biologic therapy early to achieve mucosal healing, improve remission rates, reduce cumulative steroid exposure and long-term complications
5-Aminosalicylates (5-ASA)
For mild terminal ileal or mild colonic Crohn disease only:
- Mesalamine: 50–100 mg/kg/day (max 3–4 g/day); pH-dependent release
- Less effective in Crohn than in UC; not useful for maintenance in moderate-severe disease
Antibiotics
- Metronidazole: 5 mg/kg/dose TID (up to 250 mg TID) — infectious complications and first-line for perianal disease
- Perianal disease usually recurs when stopped
- Low-dose may treat mild-moderate Crohn disease
- Ciprofloxacin: used for perianal and colonic disease
- Note: antibiotics effective for perianal fistulas; disease usually recurs on stopping
Corticosteroids
- Oral prednisone: 1–2 mg/kg/day (max 40–60 mg); once or twice daily for acute exacerbations
- Taper as soon as disease is quiescent (clinicians vary in schedules)
- No role for maintenance corticosteroids — tolerance develops; no mucosal healing; significant side effects (growth failure, adrenal suppression, cataracts, osteopenia, avascular necrosis, glucose intolerance)
- Enteric-release budesonide: 9 mg/day — for mild-moderate ileal/ileocecal Crohn; lower systemic bioavailability (10%); more effective than mesalamine but less effective than prednisone; fewer steroid side effects
Immunomodulators
~70% of pediatric patients require escalation within the first year:
| Drug | Dose | Notes |
|---|
| Azathioprine | 2.0–2.5 mg/kg/day | Onset 3–4 months; TPMT genotyping guides dosing |
| 6-Mercaptopurine (6-MP) | 1.0–1.5 mg/kg/day | Same mechanism; prodrug of azathioprine |
| Methotrexate (MTX) | 15 mg/m² IM/SC weekly (adult 25 mg/week) | Faster onset (6–8 weeks) than thiopurines; improves height velocity in pediatric CD; folic acid given concurrently; most common toxicity = hepatitis; give ondansetron before dose to reduce nausea |
Thiopurine risks: lymphoproliferative disorders (especially hepatosplenic T-cell lymphoma), hepatitis, pancreatitis, skin cancer, increased infection risk.
TPMT (thiopurine S-methyltransferase): genetic variants affect response rates and toxicity — testing guides dosing.
Biologic Therapy
Anti-TNF-α Agents
| Drug | Route | Notes |
|---|
| Infliximab (chimeric IgG1) | IV: 5 mg/kg at weeks 0, 2, 6 → q8 weeks | Induction + maintenance; mucosal healing; perianal fistula healing; steroid sparing; improved growth in children; trough levels guide dose escalation; TB screen required before starting |
| Adalimumab (fully humanized) | SC: loading dose → q2 weeks | Adults + children; dose escalation sometimes needed; risk of anti-drug antibodies |
| Certolizumab pegol | SC: q4 weeks | Adults only; PEGylated Fab fragment; minimal placental transfer |
Anti-TNF side effects: infusion/injection reactions, increased infections (especially TB reactivation — screen with PPD/IGRA first), lymphoma/leukemia, autoantibody development. Regular scheduled dosing (vs. episodic) → fewer antibodies, better durability.
Anti-Integrins
| Drug | Mechanism | Notes |
|---|
| Vedolizumab | Anti-α4β7 integrin; gut-selective | IV: 3 infusions over 6 weeks → q8 weeks maintenance; slower onset than infliximab/adalimumab; concurrent therapy often needed initially; approved adults; off-label children |
Anti-IL-12/23 and Anti-IL-23
| Drug | Mechanism | Notes |
|---|
| Ustekinumab | Anti-IL-12/IL-23 (anti-p40) | IV loading dose → SC q8 weeks maintenance; approved adults with moderate-severe Crohn; off-label children |
| Risankizumab | Anti-IL-23 (anti-p19) | Approved adults; induction + remission maintenance |
Enteral Nutritional Therapy (Exclusive Enteral Nutrition / EEN)
A major treatment option — especially in pediatric Crohn disease:
- All calories delivered via formula (elemental, semi-elemental, or polymeric)
- Equivalent in onset/efficacy to prednisone for clinical symptoms
- Superior to steroids for mucosal healing
- Side-effect free; avoids corticosteroid complications; simultaneously addresses nutritional rehabilitation
- Often given via nasogastric tube overnight (formulas are unpalatable)
- Patients cannot eat a regular diet during treatment
- A partial EEN approach (80–90% formula + some food) has shown success and is better tolerated
- High-calorie oral supplements: less effective but useful for inadequate weight gain
Total Parenteral Nutrition (TPN)
- No primary therapeutic benefit for Crohn (unlike short bowel syndrome where it's necessary)
- Used pre-operatively to optimize nutritional status if oral/enteral intake is insufficient
- Consider octreotide adjunctively for high-output fistulas (reduces GI secretions, decreases fistula output)
Complications & Their Management
Abscesses
- Occur in 15–20% of patients (especially terminal ileum)
- Intra-abdominal abscess: fever, abdominal pain, tenderness, leukocytosis; diagnose by CT scan
- Treatment: broad-spectrum antibiotics (include anaerobic coverage) + percutaneous CT/US-guided drainage
- Surgical resection of involved bowel usually required for definitive treatment (persistent communication between abscess and intestinal lumen)
- Hepatic/splenic abscess: may occur with or without local fistula
- Psoas abscess: hip pain, decreased hip extension (psoas sign), fever
Obstruction
- Common in small intestine; leading indication for surgery
- Causes: mucosal thickening (acute inflammation), muscular hyperplasia and scarring, food impaction in stricture, adhesions
- Treatment:
- Acute inflammatory obstruction: corticosteroids (IV methylprednisolone 40–60 mg/day, or hydrocortisone 200–300 mg/day × 5–14 days) + nasogastric decompression
- Fibrotic/fixed stricture: surgery (resection or strictureplasty)
- ⚠️ Common error: treating fixed fibrotic obstruction with prolonged steroids (ineffective, delays surgery)
Perianal Disease
A disabling complication:
- Assessment: examination under anesthesia; cross-sectional CT or MRI for extent of perianal abscesses
- Perianal abscess: painful; requires drainage (often surgical); local redness, tenderness, fluctuation
- Perianal fistula: seton placement by surgeon (keeps tract open while medical therapy works) → fistulotomy only if sphincter not at risk
- Medical therapy: metronidazole, infliximab, adalimumab, certolizumab, ustekinumab, vedolizumab, azathioprine/6-MP; disease often recurs when stopped
- Diversion of fecal stream can reduce perianal disease activity
Fistulas
| Fistula Type | Symptoms | Management |
|---|
| Enteroenteric | Often asymptomatic; may cause malabsorption | Medical (anti-TNF); surgery if refractory |
| Enterovesical | Pneumaturia, fecaluria, recurrent UTI | Surgery |
| Enterovaginal | Feculent vaginal discharge | Surgery |
| Enterocutaneous | Feculent skin drainage | Anti-TNF ± TPN; surgery |
| Perianal | Purulent drainage, pain | Seton, anti-TNF, antibiotics |
Anti-TNF (infliximab) is first-line medical therapy for fistulizing Crohn disease; Cochrane review supports its use.
Short Bowel Syndrome
- Rare in children; risk increases with each intestinal resection
- Consequences of terminal ileal resection (>100 cm): vitamin B12 malabsorption, bile acid malabsorption (diarrhea), fat malabsorption → oxaluria → calcium oxalate renal stones
- Increased calcium intake paradoxically decreases oxalate stone risk (binds oxalate in gut)
- Increased cholelithiasis risk: bile acid depletion from terminal ileal disease/resection
Surgical Management
Surgery cannot cure Crohn disease — recurrence rate after bowel resection is >50% by 5 years; risk of additional surgery increases with each operation.
Indications for Surgery
- Localized small bowel or colonic disease unresponsive to medical treatment
- Fibrosed stricture with symptomatic partial small bowel obstruction
- Bowel perforation
- Intractable bleeding
- Intraabdominal abscess refractory to drainage
Surgical Principles
- Remove as limited a length of bowel as possible — conservative resection (no benefit to removing histologically involved margins; reduces risk of short bowel syndrome)
- Laparoscopic approach preferred — reduced postoperative recovery
- Strictureplasty (rather than resection): for short strictures without active disease — longitudinal incision closed transversely; preserves bowel length; reoperation rate equivalent to resection
- Diversion of fecal stream: temporary for severe perianal disease (disease recurs on reconnection)
- Postoperative prophylaxis: mesalamine, metronidazole, azathioprine, or infliximab to reduce postoperative recurrence
Prognosis
- Chronic, high-morbidity but low-mortality disease
- Symptoms recur despite treatment, often without apparent explanation
- Growth failure: up to 15% of patients with early growth retardation have permanent decrease in linear growth
- Osteopenia: especially with chronic malnutrition + frequent corticosteroid exposure; DEXA scan to identify at-risk patients; treat with vitamin D, calcium, weight-bearing exercise
- Region of bowel involved and complications tend to increase over time
- Most patients eventually require surgery; reoperation rate is high
- Colon cancer risk: long-standing Crohn colitis → risk approaches that of UC; surveillance colonoscopy every 1–2 years after 8–10 years of colonic disease
- Most children lead active, full lives with intermittent flare-ups
Crohn vs. Ulcerative Colitis — Key Distinctions
| Feature | Crohn Disease | Ulcerative Colitis |
|---|
| GI extent | Mouth to anus | Colon only |
| Pattern | Discontinuous (skip lesions) | Continuous from rectum |
| Inflammation depth | Transmural | Mucosal (except toxic megacolon) |
| Ulceration | Discrete, serpiginous | Continuous |
| Fistula | Yes | No |
| Stricture | Yes | No |
| Perianal disease | Yes | No (except mild fissures) |
| Granulomas | Yes (noncaseating) | No |
| Oral ulcers | Yes | No |
| Cobblestoning | Yes | No |
| B12 deficiency | Yes | No |
| Bone disease | Yes | No |
| Smoking effect | Increases risk | Protects |
| Curative surgery? | No | Yes (total colectomy) |
| ASCA | 40–70% positive | <15% positive |
| pANCA | <20% positive | ~70% positive |
| Concordance in MZ twins | 36% | 16% |
Recent Evidence (2024–2026)
- A 2024 network meta-analysis (PMID 38185396) compared advanced therapies for endoscopic outcomes in Crohn disease — ustekinumab and combination anti-TNF + immunomodulator therapy showed superior mucosal healing in network comparisons.
- A 2025 Lancet Gastroenterology consensus (PMID 40315877) proposed novel diagnostic criteria and management guidance specifically for isolated perianal Crohn disease — an historically underrecognized phenotype.
Sources: Nelson Textbook of Pediatrics 2024, Chapter 382.2 (pp. 2317–2322); Goldman-Cecil Medicine, Chapter 127; Sleisenger & Fordtran's Gastrointestinal and Liver Disease, Chapters 115–116