pistol grip deformity in congenital pseudo arthrosis of tibia
Reading File
Finding Sources
Finding Sources
Searching PubMed
"congenital pseudarthrosis" AND tibia
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Searching the Web
pistol grip deformity congenital pseudarthrosis tibia classification Crawford
Reading File
Reading Web Page
https://www.ncbi.nlm.nih.gov/books/NBK576443
Loading Image
I now have all the information needed for a thorough answer. Here is a comprehensive explanation of the pistol grip deformity in congenital pseudarthrosis of the tibia (CPT):
Pistol Grip Deformity in Congenital Pseudarthrosis of the Tibia (CPT)
What Is It?
The "pistol grip deformity" is the characteristic clinical and radiographic appearance of the lower leg in CPT, where the distal leg and foot angulate anteriorly relative to the proximal tibia - resembling the shape of a pistol when viewed from the side. It arises from the anterolateral bowing of the tibia that is the hallmark of CPT.
Specifically, the term describes the lateral radiograph appearance:
- The tibia is the "barrel" of the pistol
- The foot and ankle form the "grip," angulated sharply anteriorly and laterally at the pseudarthrosis or dysplastic zone in the distal half of the tibia
Pathoanatomy
CPT predominantly affects the distal half of the tibia (and frequently the ipsilateral fibula). The site of deformity is characterized by:
- Hamartomatous fibrous tissue replacing normal bone at the pseudarthrosis site - this abnormal tissue has limited vascular ingrowth and poor healing potential, even after surgical intervention
- Sclerosis and narrowing of the medullary canal at and around the lesion
- Progressive anterolateral angulation through this weakened zone under weight-bearing forces
The resulting angular deformity - anterior bowing with lateral displacement of the distal segment - produces the pistol grip shape. The ankle and foot hang anteriorly, while the proximal tibia remains relatively straight. - Campbell's Operative Orthopaedics 15th Ed 2026
Radiographic Appearance
Campbell's Figure 31.57 - Three examples of congenital pseudarthrosis of tibia showing anterolateral bowing in various stages
The key radiographic features are:
- Anterolateral bowing with apex directed anterolaterally (distinguishes CPT from posteromedial bowing and fibular hemimelia)
- Sclerotic, narrow medullary canal at the apex (Crawford Type I/II)
- Cystic or pre-fracture changes (Crawford Type III)
- Established fracture/pseudarthrosis (Crawford Type IV)
Crawford Classification (Most Used)
| Type | Findings |
|---|---|
| I | Anterior bowing + increased cortical density, narrow medulla |
| II | Anterior bowing + sclerotic bone, narrow medulla (highest risk of fracture) |
| III | Anterior bowing + cystic change / pre-fracture lesion |
| IV | Established fracture and pseudarthrosis (fibula often involved) |
The pistol grip appearance is most pronounced in Crawford Type III and IV, where the fracture/pseudarthrosis has allowed complete angular displacement.
Etiology and Associations
- Incidence: ~1 in 250,000 live births
- NF1 association: 50-90% of cases are associated with stigmata of neurofibromatosis type 1 (NF1) - cafe-au-lait spots, Lisch nodules, etc.
- Exact cause is unknown; the hamartomatous tissue at the pseudarthrosis site is believed to be the primary pathological substrate
- Bailey & Love notes: "the tibial bow has an anterolateral apex" - a key distinguishing feature vs. other tibial bowing conditions
Clinical Features
- Usually unilateral
- The pistol grip deformity may be present at birth (primary/neonatal form) or develop after the child begins walking (secondary form with pathological fracture)
- Leg shortening from tibial bowing and decreased tibial growth
- Progressive valgus deformity of the ankle if the fibula is also involved (proximal migration of lateral malleolus)
- Once fractured, the tibia will NOT heal with casting alone - surgical treatment is mandatory
Treatment Principles
Since the pistol grip deformity progresses once walking begins, management targets:
-
Pre-fracture (intact bowing): Clamshell orthosis/protective bracing until skeletal maturity. Guided growth of the distal lateral tibia (hemi-epiphysiodesis) can gradually correct the bow and potentially prevent fracture.
-
Post-fracture/established pseudarthrosis: Three core principles:
- Complete resection of the pseudarthrosis and surrounding hamartomatous tissue
- Restoration of mechanical alignment (correcting the pistol grip angulation)
- Intramedullary rodding - often crossing the ankle joint for very distal lesions; telescoping rods protect the bone through growth
-
Augmented by: bone grafting, bone morphogenetic protein (BMP), Ilizarov/distraction osteogenesis, or free vascularized fibular graft (for gaps >3 cm)
-
Amputation is rarely first-line but must be discussed early when: anticipated shortening >5-7.5 cm, multiple failed surgeries, or stiff/dysfunctional limb - Campbell's Operative Orthopaedics 15th Ed 2026
Key Distinguishing Points (Exam Focus)
| Feature | CPT |
|---|---|
| Direction of bow | Anterolateral (apex anterolateral) |
| NF1 association | 50-90% |
| Site | Distal 1/3 tibia most common |
| Healing with cast alone | No - never heals after fracture |
| Eponym for deformity | Pistol grip deformity |
| Histology at site | Hamartomatous fibrous tissue, poor vascularity |
A recent CPAM-LRC consensus guideline (2025) (PMID 39764600) provides updated surgical recommendations, noting that intramedullary rodding combined with bone grafting remains the standard, with Ilizarov fixation and vascularized fibular grafts as adjuncts for complex or recurrent cases.
give me cilinical images of CPT
Finding Sources
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
Reading File
Loading Image
Reading File
Here are all the clinical and radiographic images of CPT from Campbell's Operative Orthopaedics and Bailey & Love, organized by what they show:
Clinical Images of CPT
Image 1 - Established Pseudarthrosis: Pre-op, Intraoperative & Post-op Series
(Campbell's Fig. 31.55)
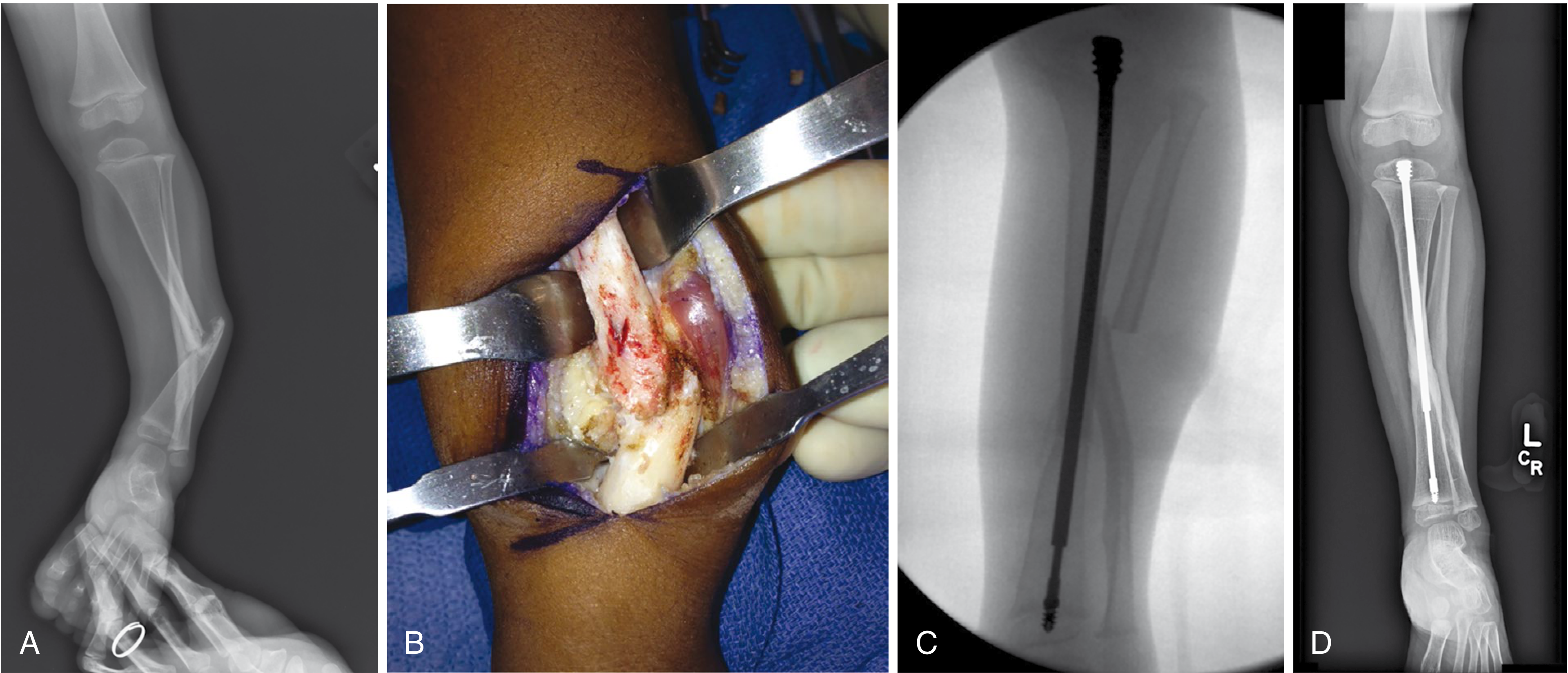
- A - Lateral radiograph of a 3-year-old: classic pistol grip deformity with established nonunion present since birth - the sharp anterior angulation of the distal tibia is clearly visible
- B - Intraoperative photo showing the hamartomatous fibrous tissue at the pseudarthrosis site (white, avascular, glistening tissue between bone ends - the pathological substrate of CPT)
- C - Intraoperative fluoroscopy showing the telescoping intramedullary rod crossing the ankle joint after debridement + bone graft + BMP
- D - Healed nonunion at 10 months postoperatively with the rod in situ
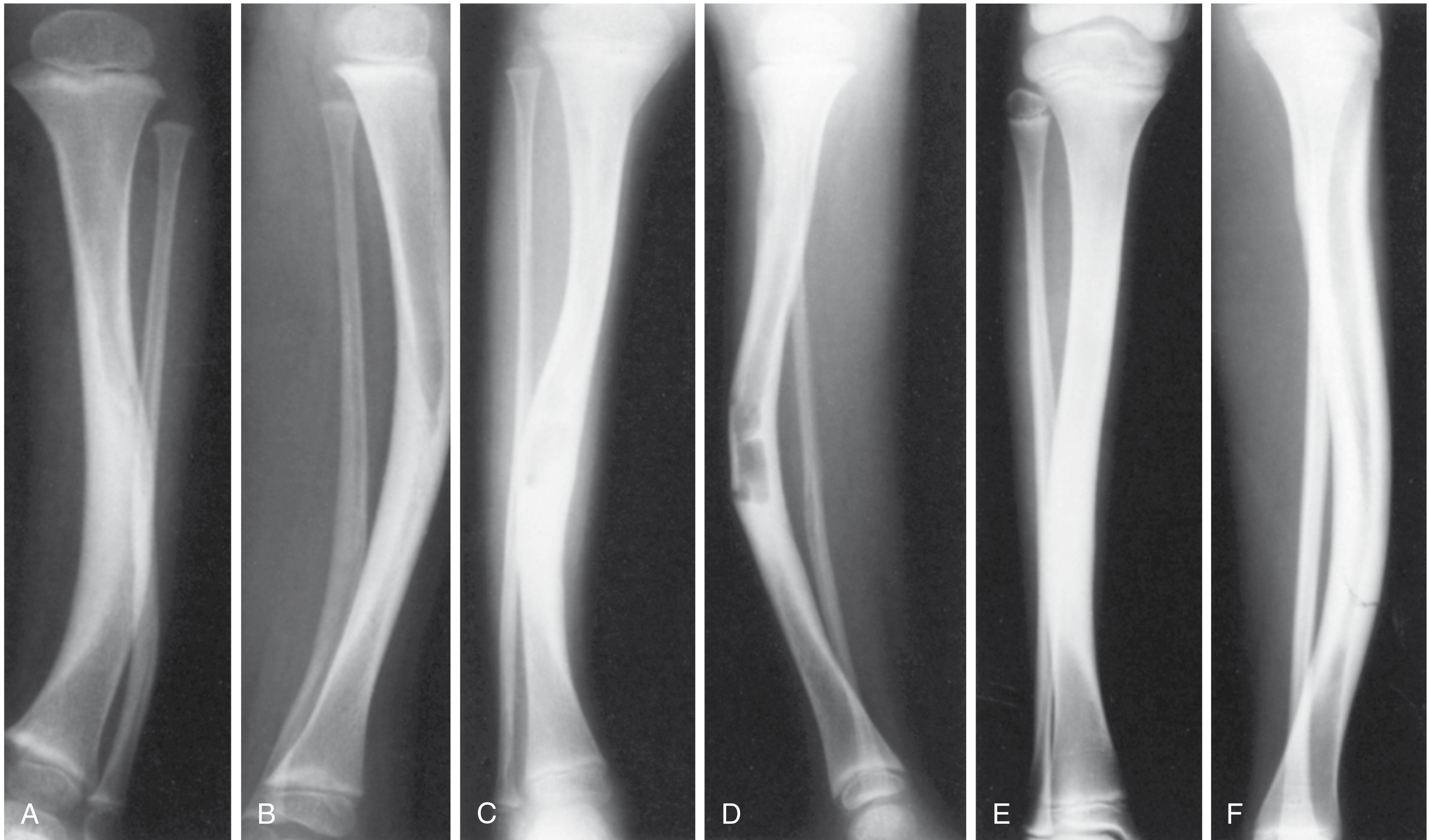
Image 2 - Crawford Classification Spectrum (Types I-IV)
(Campbell's Fig. 31.57)
- A & B - Anterolateral bowing without fracture (Crawford Type I/II) - sclerotic bone, narrow medullary canal
- C & D - Anterolateral bowing with cystic formation (Crawford Type III) - pre-fracture stage
- E & F - Anterolateral bowing with stress fracture progressing to pseudarthrosis (Crawford Type IV)
Image 3 - Guided Growth Treatment for Anterolateral Bowing
(Campbell's Fig. 31.58)
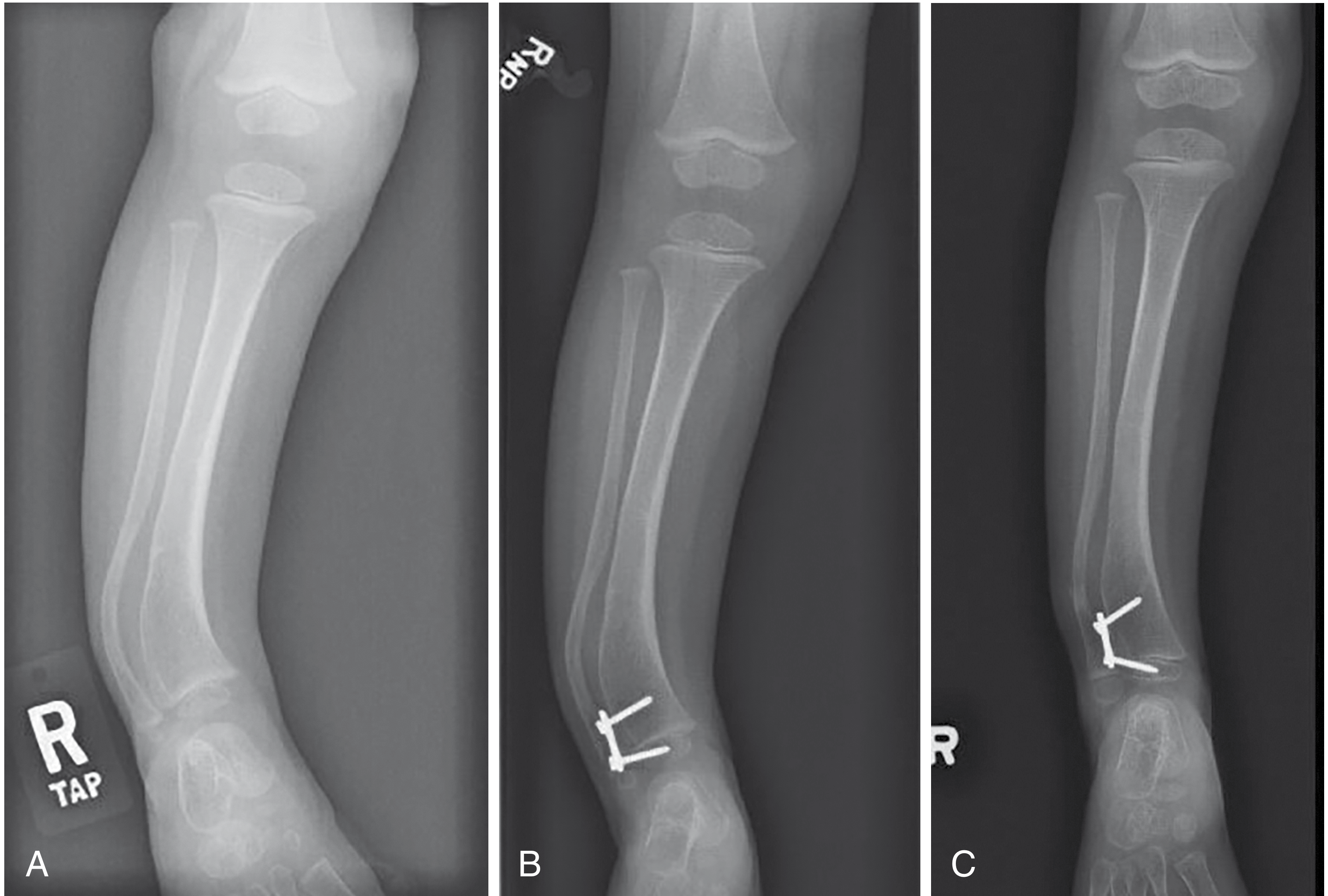
- A - Preoperative AP radiograph showing anterolateral bowing (pre-fracture intact tibia)
- B - Immediate post-op: hemi-epiphysiodesis compression plate applied to the distal lateral tibia to gradually correct the bow via guided growth
- C - 18-month follow-up showing progressive correction of the deformity
Image 4 - CPT with Fibular Involvement (Bailey & Love)
(Bailey & Love Fig. 44.28)

AP radiograph showing congenital tibial pseudarthrosis with fibular involvement. This child was born with a bowed lower leg that subsequently fractured. She has a family history of neurofibromatosis type 1 - demonstrating the common NF1 association.
Image 5 - Severe CPT: Pre-op and Post-op Intramedullary Rodding
(Campbell's Fig. 31.60 - Anderson technique)
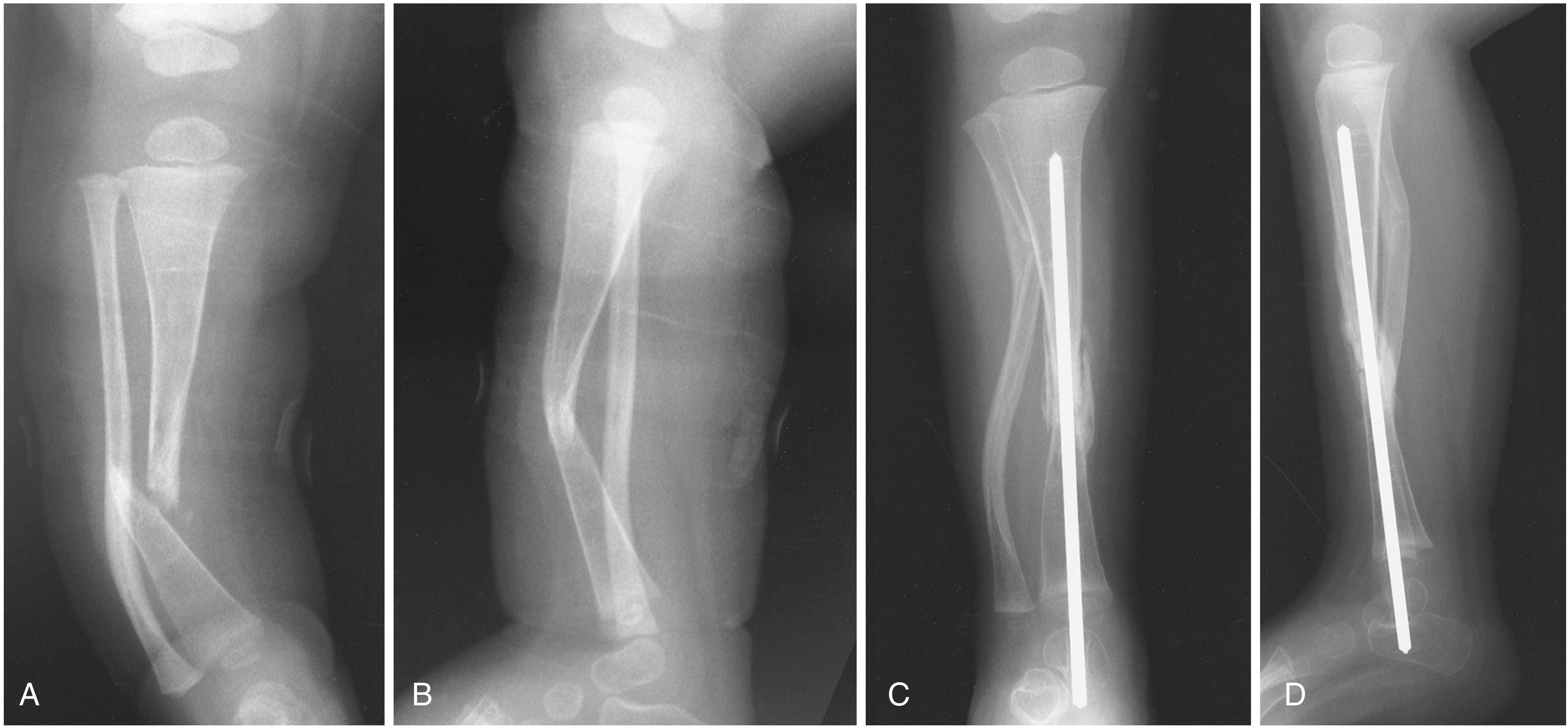
- A - AP view of Crawford Type II CPT in a 16-month-old: sclerotic distal tibia with anterolateral bow and fibular pseudarthrosis
- B - Lateral view showing the pistol grip deformity in full - the sharp anterior apex angulation is the defining feature
- C & D - Post-op AP and lateral: Peter Williams telescoping intramedullary rod crossing the ankle joint after pseudarthrosis excision and bone grafting, with restoration of tibial alignment
Key teaching point from all images: The pistol grip deformity is most dramatically visible on the lateral radiograph (Images 1A and 5B), where the distal tibia angulates sharply anteriorly, and the foot hangs forward like the grip of a pistol. The intraoperative photo (Image 1B) is one of the rare textbook images showing the actual pathological hamartomatous tissue that makes this condition so resistant to healing.
Source: Campbell's Operative Orthopaedics 15th Ed 2026; Bailey and Love's Short Practice of Surgery 28th Ed
This is a shared conversation. Sign in to Orris to start your own chat.