Humoral immunity
Reading File
Finding Sources
Searching the Web
humoral immunity overview B cells antibodies mechanism
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Reading File
I now have comprehensive content. Let me compile the full answer.
Humoral Immunity
Humoral immunity is the arm of adaptive immunity mediated by B lymphocytes and their secreted products - antibodies (immunoglobulins). It defends against extracellular microbes and their toxins, and is the basis for most vaccine-induced protection.
Overview
B cells recognize antigens via their surface immunoglobulin (IgM and IgD) receptors. Upon activation, they proliferate and differentiate into plasma cells that secrete antibodies. A single B cell can give rise to ~5,000 antibody-secreting cells within a week, each secreting ~2,000 antibody molecules per second - this remarkable rate is necessary to match the pace of rapidly dividing microbes. (Cellular and Molecular Immunology, p. 751)
B Cell Development and Maturation
- B cells originate in the bone marrow, where they undergo V(D)J recombination to generate a diverse BCR repertoire
- Mature naive B cells enter the circulation and home to secondary lymphoid organs (lymph nodes, spleen, MALT)
- Each B cell expresses a BCR with unique antigen specificity - the same specificity as the antibodies it will eventually secrete
Antigen Recognition and B Cell Activation
Antigen Delivery to B Cells
Antigens reach follicular B cells by multiple routes (Cellular and Molecular Immunology, p. 757):
- Small soluble antigens (<70 kD): travel via conduits from the subcapsular sinus directly to follicles
- Large particulate antigens: captured by subcapsular sinus macrophages and delivered to follicles
- Immune complexes: bind CR2 (CD21) on marginal zone B cells or follicular dendritic cells (FDCs) for sustained presentation
T-Dependent vs. T-Independent Responses
| Feature | T-Dependent | T-Independent |
|---|---|---|
| Antigen type | Proteins | Polysaccharides, lipids, repeated epitopes |
| Helper T cell required | Yes (CD4+ Tfh cells) | No |
| Isotype switching | Yes (IgG, IgA, IgE) | Minimal (mainly IgM) |
| Affinity maturation | Yes | Minimal |
| Memory generation | Robust | Limited |
T-dependent responses require B cells to internalize antigen, process it, and present peptide-MHC II complexes to CD4+ T follicular helper (Tfh) cells. The Tfh cells then provide help through:
- CD40L - CD40 interaction (essential costimulatory signal)
- Cytokines (IL-4, IL-5, IL-21) that drive proliferation, isotype switching, and differentiation
T-independent responses are triggered by antigens with repetitive epitopes (e.g., bacterial capsular polysaccharides) that crosslink multiple BCRs simultaneously.
The Germinal Center Reaction
After T-dependent activation, B cells and Tfh cells migrate into lymphoid follicles to form germinal centers (GCs) - specialized microenvironments critical for humoral immunity quality:
- Somatic hypermutation: activation-induced cytidine deaminase (AID) introduces point mutations in V region genes, generating B cell variants with subtly different BCR affinities
- Affinity maturation: B cell clones with higher-affinity BCRs outcompete lower-affinity clones for binding to antigen displayed on follicular dendritic cells - the result is progressive improvement in antibody quality
- Isotype (class) switching: AID also mediates DNA recombination to replace the IgM heavy chain constant region with IgG, IgA, or IgE constant regions, without changing antigen specificity
- Differentiation: GC B cells become either long-lived plasma cells or memory B cells
Antibody Classes and Their Functions
| Isotype | Key Effector Functions |
|---|---|
| IgG | Opsonization (via FcγR on phagocytes), complement activation, ADCC (NK cells), neonatal immunity (placental transfer), neutralization |
| IgM | Complement activation (most potent classical pathway activator), neutralization; first antibody produced in primary response |
| IgA | Mucosal immunity - secreted across epithelia into gut/respiratory/urogenital lumens; neutralization at mucosal surfaces |
| IgE | Mast cell/basophil degranulation; defense against helminths (ADCC via eosinophils) |
(Cellular and Molecular Immunology, Table 13.2, p. 824)
Antibody Effector Mechanisms
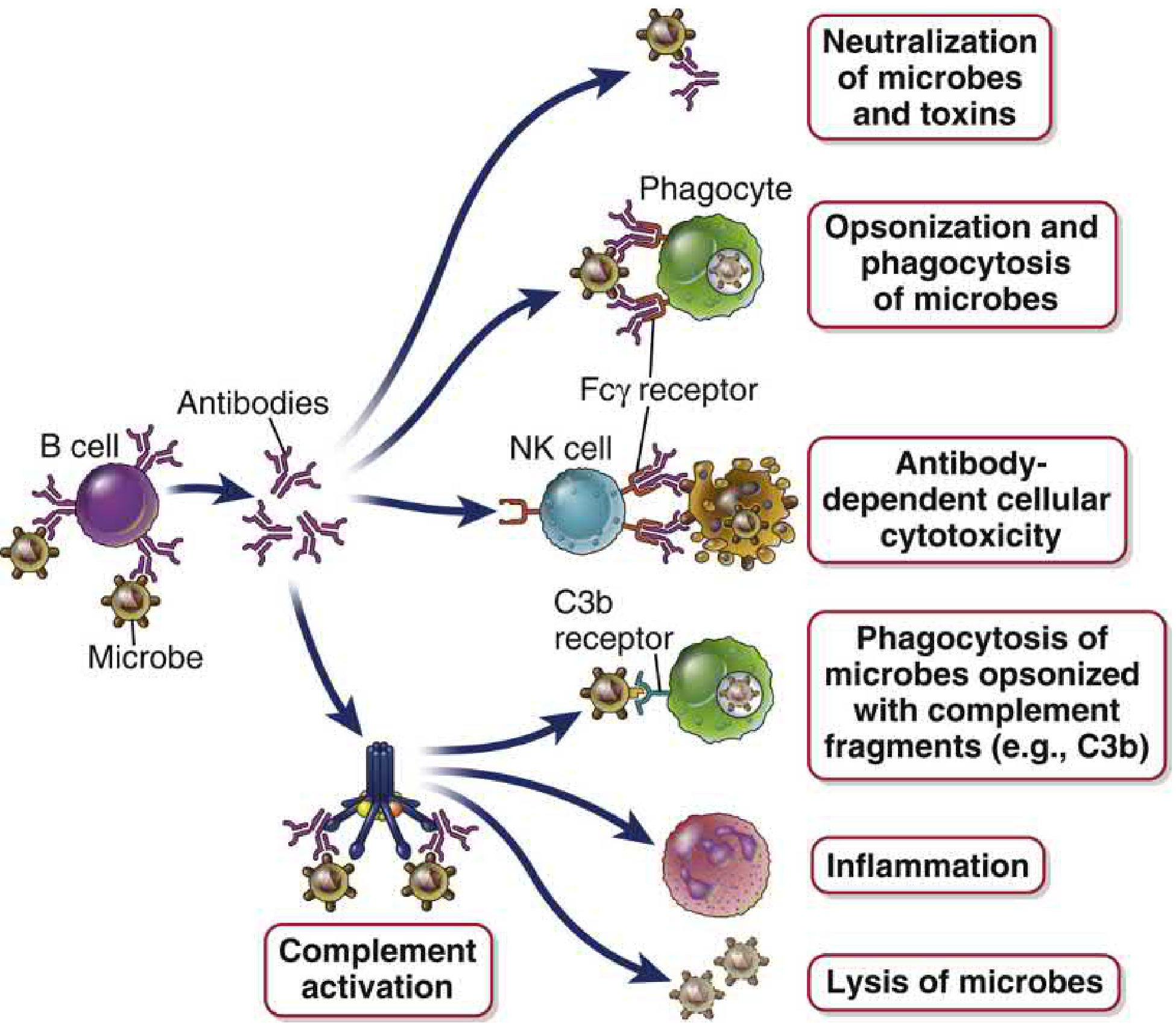
FIGURE 13.1 - Effector functions of antibodies. Cellular and Molecular Immunology
1. Neutralization
Antibodies bind to surface structures of pathogens or toxins, physically blocking their interaction with host cell receptors. This is the only effector mechanism that can prevent infection before it is established - hence the focus of most vaccines on generating neutralizing antibodies. Mediated entirely by Fab (variable) regions, no Fc required. (Cellular and Molecular Immunology, p. 823)
2. Opsonization and Enhanced Phagocytosis
IgG coats microbes; phagocytes (neutrophils, macrophages) bear FcγRs that bind the Fc regions, dramatically enhancing phagocytosis. Complement fragments (C3b, C4b) deposited on microbes similarly promote uptake via CR1.
3. Complement Activation (Classical Pathway)
IgM and IgG (IgG1, IgG2, IgG3) activate C1q when clustered on antigen surfaces. This initiates the classical complement cascade, generating:
- C3b (opsonin)
- C3a/C5a (anaphylatoxins - recruit inflammatory cells)
- Membrane attack complex (C5b-9) - directly lyses microbes
4. Antibody-Dependent Cellular Cytotoxicity (ADCC)
IgG antibodies coat target cells (e.g., virus-infected cells); NK cells bearing FcγRIII (CD16) recognize the Fc and release cytotoxic granules (perforin, granzymes), killing the target.
5. Mucosal Immunity (IgA)
Dimeric IgA is transported by the polymeric immunoglobulin receptor (pIgR) across mucosal epithelium into secretions. Secretory IgA neutralizes pathogens in the gut and respiratory tracts before systemic invasion occurs.
6. Neonatal Protection
Maternal IgG is actively transported across the placenta via FcRn (neonatal Fc receptor) and provides passive immunity to the newborn until their own immune system matures.
Primary vs. Secondary Antibody Responses
| Feature | Primary Response | Secondary Response |
|---|---|---|
| Lag phase | 5-10 days | 1-3 days |
| Peak antibody level | Lower | Much higher |
| Dominant isotype | IgM (then IgG) | IgG (also IgA, IgE) |
| Antibody affinity | Lower | Higher (affinity-matured) |
| Duration | Shorter | Longer |
The secondary (anamnestic) response is driven by memory B cells - long-lived cells generated during the primary response that circulate and rapidly differentiate into plasma cells upon re-exposure to the same antigen.
Long-Lived Humoral Memory
- Long-lived plasma cells: migrate to bone marrow niches after GC reactions; continue secreting antibodies for years to decades, providing baseline serum antibody levels
- Memory B cells: quiescent, antigen-experienced cells with high-affinity BCRs; reactivated rapidly upon antigen re-encounter, providing accelerated and amplified secondary responses
Clinical Relevance
Vaccine-induced humoral immunity (examples from Cellular and Molecular Immunology, Table 13.1):
| Disease | Vaccine | Protective Mechanism |
|---|---|---|
| Polio | Salk/Sabin | IgG/IgA neutralization of virus |
| Tetanus, Diphtheria | Toxoids | IgG neutralization of toxin |
| Hepatitis B | Recombinant HBsAg | IgG/IgA neutralization |
| Pneumococcal/H. influenzae | Conjugate vaccines | IgG/IgM opsonization + complement |
Humoral immunodeficiencies: Defects in B cell development or activation result in susceptibility to extracellular pyogenic bacteria (e.g., S. pneumoniae, H. influenzae). Examples include X-linked agammaglobulinemia (BTK deficiency), common variable immunodeficiency (CVID), and selective IgA deficiency.
Sources: Cellular and Molecular Immunology (Abbas et al.), pp. 48-49, 751-824; Roitt's Essential Immunology; Henry's Clinical Diagnosis and Management by Laboratory Methods
This is a shared conversation. Sign in to Orris to start your own chat.