Asom and csom and otoscope all parts with images easy to understand
ASOM CSOM otoscope parts diagram labeled easy understand medical student
ASOM, CSOM & Otoscope - Complete Guide
🔬 THE OTOSCOPE - Parts & How It Works
Otoscope with Ear Anatomy

Parts of the Otoscope
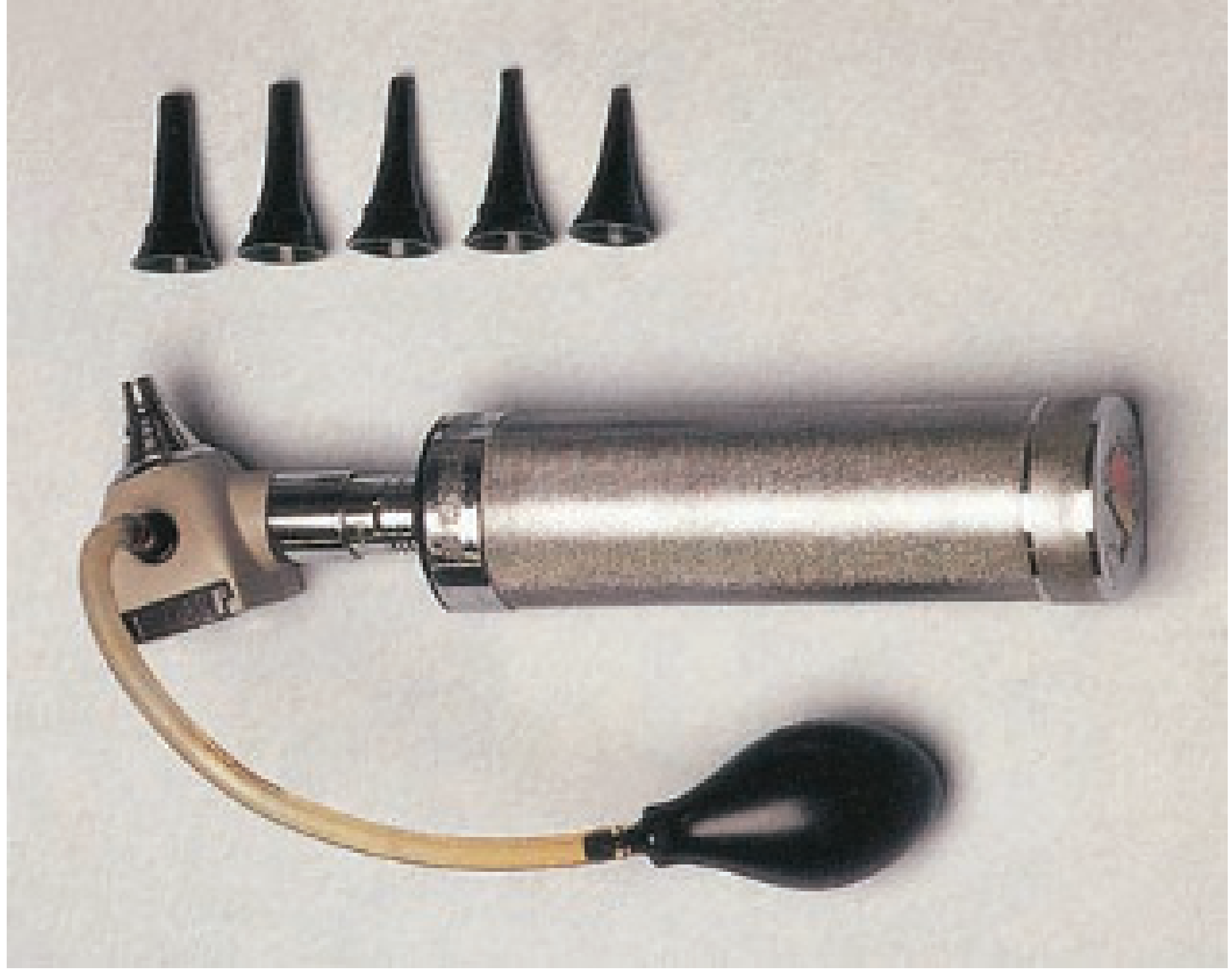
| Part | Function |
|---|---|
| Handle | Battery-powered light source; how you grip the device |
| Head / Body | Contains the light, optics, and lens |
| Magnifying lens | Magnifies what you see (can be moved aside to pass instruments) |
| Speculum | Cone-shaped tip inserted into the ear canal; comes in multiple sizes (choose the largest that fits comfortably) |
| Pneumatic bulb | Squeeze bulb attached by tubing; used to puff air and test eardrum movement (pneumatic otoscopy) |
- Standard (hand-held) otoscope - for routine examination; monocular, limited magnification
- Pneumatic otoscope - has the bulb attachment for assessing TM mobility (very useful to detect middle ear fluid)
- Operating otoscope - lens swings aside so you can insert instruments to remove cerumen or foreign bodies
- Binocular microscope (otomicroscope) - provides stereoscopic (3D) vision, higher magnification, two-handed technique
The Tympanic Membrane (what you see through the otoscope)

- Handle of malleus - the first thing to identify; a white diagonal stripe
- Lateral process of malleus - small bony bump at the top of the handle
- Umbo - the bottom tip of the malleus handle; the most concave point of the TM
- Cone of light (light reflex) - a triangular reflection from the umbo pointing anteriorly-inferiorly
- Pars tensa - the main, taut part of the TM (lower 4 quadrants)
- Pars flaccida - the small, floppy upper part above the mallear folds
- Anterior mallear fold and Posterior mallear fold - folds bordering the pars flaccida
⚡ ASOM - Acute Suppurative Otitis Media
What is it?
Common Causes (Pathogens)
| Bacteria | Notes |
|---|---|
| Streptococcus pneumoniae | Most common (up to 80% in children) |
| Haemophilus influenzae | Common; also causes otitis-conjunctivitis syndrome |
| Moraxella catarrhalis | Common in children |
How Does It Start? (Pathogenesis)
- Upper respiratory tract infection (common cold) inflames and swells the Eustachian tube
- Eustachian tube dysfunction - tube that connects the middle ear to the back of the nose gets blocked
- Bacteria travel up from the nasopharynx into the middle ear
- Pus builds up in the middle ear cavity, increasing pressure
Stages of ASOM (Classic teaching)
| Stage | What happens | TM appearance on otoscopy |
|---|---|---|
| 1. Hyperaemia | Blood vessels dilate; early inflammation | TM slightly pink/red, vessels visible |
| 2. Exudation | Fluid accumulates in middle ear | TM red, opaque, bulging |
| 3. Suppuration | Pus forms; TM under pressure | TM bright red, severely bulging, extremely painful |
| 4. Perforation | TM ruptures, pus drains out | Perforation visible; ear discharge starts; PAIN RELIEVES |
| 5. Resolution/Complications | Heals OR becomes chronic | TM heals in most cases |
Symptoms
- Ear pain (otalgia) - main symptom, sudden onset
- Fever, general unwellness
- Hearing loss (conductive)
- Children may pull at their ears, be irritable, have poor appetite
- Otorrhoea (ear discharge) if TM perforates - pain dramatically improves at this point
What You See on Otoscopy
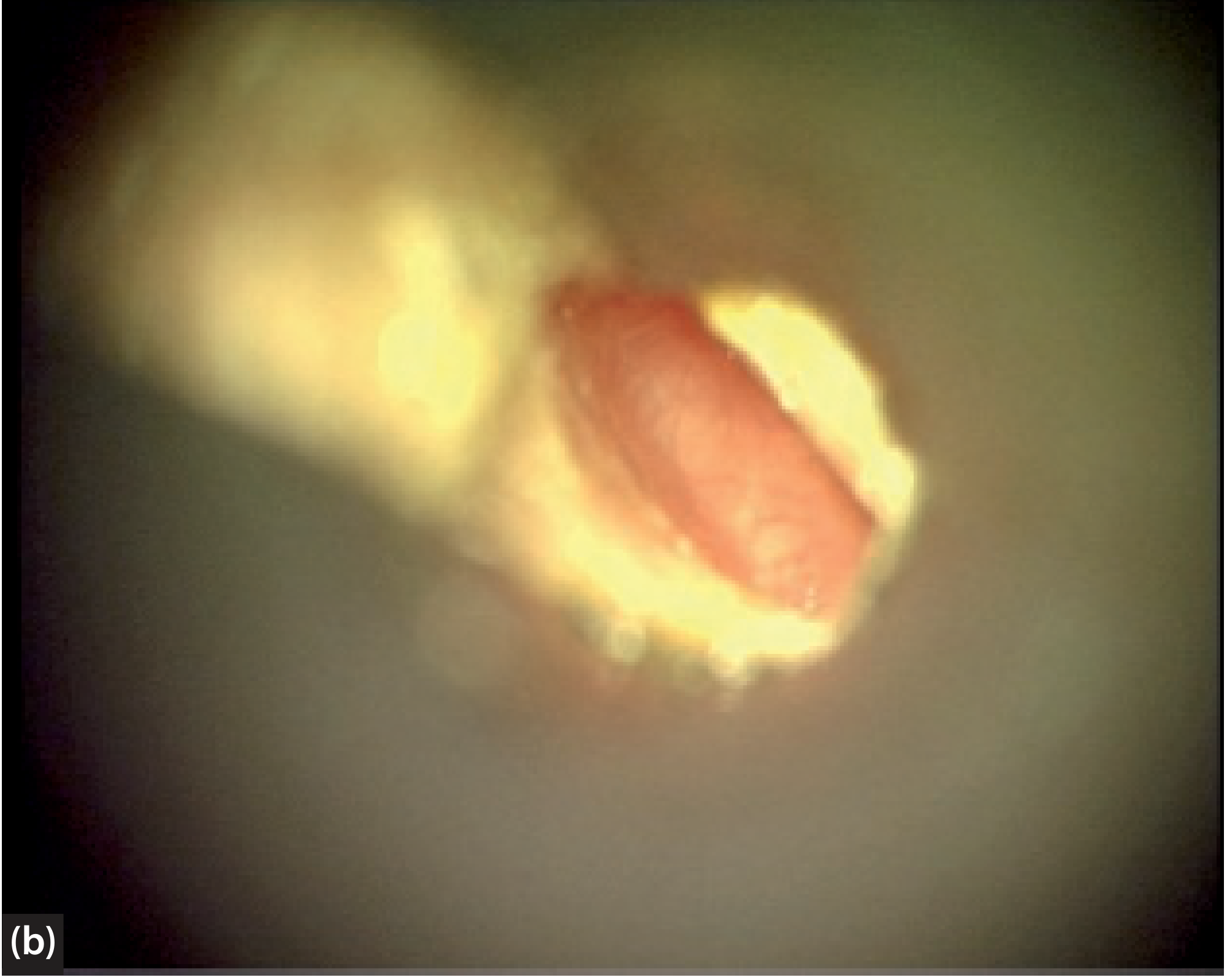
- TM is red and opaque (erythematous)
- Bulging outward - this is the most important sign (moderate-severe bulging highly predictive of AOM)
- No light reflex or distorted
- Landmarks obscured by swelling
- TM immobile on pneumatic otoscopy
- If perforated: visible hole, pus draining
Treatment
- Antibiotics: Amoxicillin is first-line; amoxicillin-clavulanate if treatment failure or severe
- Analgesia: Paracetamol/ibuprofen for pain
- Watchful waiting acceptable in mild/moderate cases in children >2 years
- Myringotomy (surgical TM incision to drain pus) if severe or not improving
Complications of ASOM
- Mastoiditis (most common complication)
- Facial nerve paralysis
- Meningitis, intracranial abscess
- Sensorineural hearing loss
- Progression to CSOM if not treated
🔄 CSOM - Chronic Suppurative Otitis Media
What is it?
WHO estimates 65-330 million people worldwide have CSOM; 50% suffer from hearing impairment. (Scott-Brown's Otorhinolaryngology)
How is CSOM Different from ASOM?
| Feature | ASOM | CSOM |
|---|---|---|
| Duration | Acute (<3 weeks) | Chronic (>6-12 weeks, recurrent) |
| Tympanic membrane | Intact (usually bulging) | Perforated (the defining feature) |
| Discharge | Only if TM perforates | Always present (through perforation) |
| Pain | Severe | Usually absent/mild |
| Fever | Common | Usually absent |
| Organisms | Pneumococcus, H. influenzae | Pseudomonas, Staph. aureus, anaerobes |
Types of CSOM
Type 1 - Tubotympanic (Safe / Mucosal) CSOM
- Perforation in the pars tensa (central/anterior)
- Mucoid or mucopurulent discharge
- No cholesteatoma
- Hearing loss present but generally less severe
- Generally considered "safe" (fewer dangerous complications)
Type 2 - Atticoantral (Unsafe / Squamous) CSOM
- Perforation in the pars flaccida or posterior-superior pars tensa (marginal/attic)
- Cholesteatoma present (accumulation of keratin-producing squamous epithelium)
- Foul-smelling, scanty discharge
- More aggressive bone destruction
- Called "unsafe" due to serious complication risk
Otoscopic Findings in CSOM

- Visible perforation in the TM (central or marginal depending on type)
- Pus/discharge in the canal or through the perforation
- Granulation tissue around the perforation edges
- In cholesteatoma: pearly white mass visible, usually in the attic region
- Marginal perforations suggest unsafe/cholesteatoma type
Symptoms
- Otorrhoea (ear discharge) - intermittent or continuous; may be mucoid or foul-smelling
- Hearing loss (conductive) - degree depends on extent of damage
- No or minimal pain (distinguishes from ASOM)
- Tinnitus
Complications of CSOM
- Mastoiditis
- Facial nerve palsy
- Labyrinthitis
- Meningitis
- Brain abscess
- Lateral sinus thrombosis
Treatment
- Medical: Aural toileting (cleaning the ear), topical antibiotic drops (ciprofloxacin), treat underlying infections
- Surgical:
- Myringoplasty - repair of the TM perforation (when ear is dry)
- Tympanoplasty - reconstruction of TM and ossicles
- Mastoidectomy - removal of diseased mastoid bone (especially if cholesteatoma)
- For cochlear implant candidates: staged approach - clear disease first, implant after ear is dry
🔑 Quick Comparison Table: ASOM vs CSOM
| Feature | ASOM | CSOM |
|---|---|---|
| Onset | Acute | Chronic/recurrent |
| TM | Intact, red, bulging | Perforated |
| Pain | Severe | Absent/mild |
| Discharge | Only if perforated | Always present |
| Fever | Yes | No |
| Hearing loss | Conductive (temporary) | Conductive (persistent) |
| Cholesteatoma | No | Possible (atticoantral type) |
| Key treatment | Antibiotics | Aural toilet + surgery |
| Dangerous complications | Rare (<1%) | More common (especially cholesteatoma type) |
📋 Structured Otoscopy Approach (How to Examine)
- Choose the largest speculum that fits comfortably
- Pull the pinna up and backward (adults) to straighten the canal
- Identify the malleus handle first - your anchor point
- Find the lateral process (small bump, top of handle)
- Find the umbo (bottom tip of handle)
- Look for the cone of light (antero-inferior)
- Assess pars tensa - is it intact? Normal position? Retracted? Bulging?
- Assess pars flaccida (attic) - for retraction pockets or cholesteatoma
- Use the pneumatic bulb - squeeze gently and watch for TM movement (no movement = fluid or perforation)
"The most recognizable feature in most ears is the handle of malleus and this should be the first structure sought." - Scott-Brown's Otorhinolaryngology
Refractive error with images very easy to understand
refractive error myopia hyperopia astigmatism presbyopia diagram labeled images
astigmatism cornea shape diagram blurred vision football shaped eye
presbyopia aging lens accommodation loss diagram near vision
Refractive Errors - Complete Visual Guide 👁️
What is a Refractive Error?
"In emmetropia, parallel rays from infinity are focused perfectly on the retina. In myopia, the globe is too long and light rays come to a focal point in front of the retina. In hyperopia, the globe is too short..." - Harrison's Principles of Internal Medicine 22E
The Big Picture - All 4 Refractive Errors

The 4 Types of Refractive Error
| Type | Common Name | Focal Point | Eye Shape | Blurred Distance |
|---|---|---|---|---|
| Myopia | Nearsightedness | In FRONT of retina | Too LONG | Far objects |
| Hyperopia | Farsightedness | BEHIND retina | Too SHORT | Near objects |
| Astigmatism | Distorted vision | Multiple points | Irregular cornea | Both |
| Presbyopia | Age-related reading difficulty | Behind retina | Stiff lens | Near only |
1. 👀 MYOPIA (Nearsightedness / Short-sightedness)
What happens?
- The eyeball is too long (axial length), OR the cornea is too steeply curved
- Light focuses in FRONT of the retina instead of on it
- You can see near objects clearly, but distant objects are blurry
Vision Correction Diagram

Key Facts
| Feature | Detail |
|---|---|
| Who gets it? | Usually children; progresses until age 20-25 |
| Prevalence | Most common refractive error globally |
| Corrective lens | Concave (minus/diverging) lens - spreads light rays out |
| Prescription | Written as negative numbers (e.g. -1.00, -3.50) |
| Surgery | LASIK, PRK, SMILE (laser reshapes cornea) |
Simple analogy
Danger - Pathologic Myopia
- Retinal detachment
- Retinal holes
- Choroidal neovascularization
- Associated with Marfan syndrome, Stickler syndrome
2. 🔭 HYPEROPIA (Farsightedness / Long-sightedness)
What happens?
- The eyeball is too short, OR the cornea is too flat
- Light focuses BEHIND the retina
- Near objects are blurry; in young people the lens can compensate partially by "accommodating" (squeezing itself to bend light more)
Key Facts
| Feature | Detail |
|---|---|
| Who gets it? | Any age; young patients may not notice (lens compensates) |
| Symptom trigger | Becomes problematic around age 40+ when lens stiffens |
| Corrective lens | Convex (plus/converging) lens - converges light rays |
| Prescription | Written as positive numbers (e.g. +1.00, +3.50) |
| Associated risk | Narrow-angle glaucoma (short eye = crowded drainage angle) |
Simple analogy
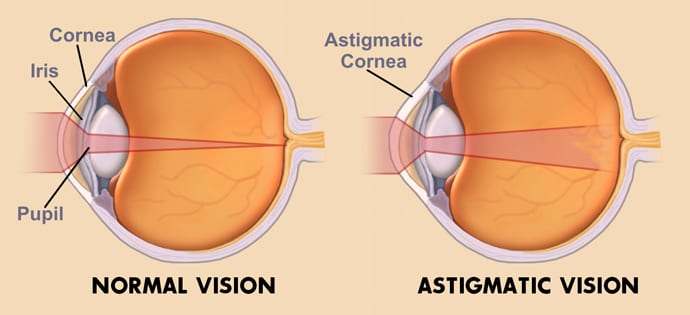
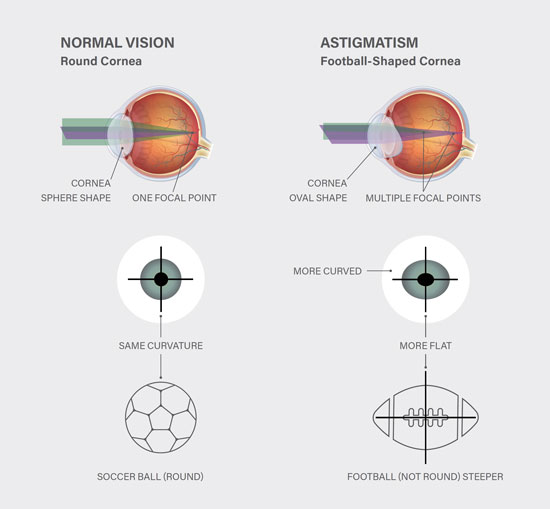
3. 🏉 ASTIGMATISM
What happens?
- The cornea (or lens) is oval/football-shaped instead of perfectly round
- Different parts of the cornea have different curvatures (like a rugby ball vs. a basketball)
- Light focuses at multiple points instead of one single point
- Vision is blurry AND distorted at ALL distances
Astigmatism vs Normal Eye
Types of Astigmatism
| Type | Cause | Treatment |
|---|---|---|
| Regular | Uniform variation; most common | Glasses, toric contact lenses, LASIK |
| Irregular | Corneal scarring, keratoconus, trauma | Rigid contact lenses; harder to correct with glasses |
Key Facts
| Feature | Detail |
|---|---|
| Corrective lens | Cylindrical (toric) lens |
| Prescription | Has a sphere + cylinder + axis component |
| Symptoms | Blurry + distorted vision, "shadowing" around letters, eyestrain |
| Common associations | Often occurs alongside myopia or hyperopia |
What does astigmatic vision look like?
4. 📖 PRESBYOPIA (Age-related near vision loss)
What happens?
Normal Accommodation (Young Eye)
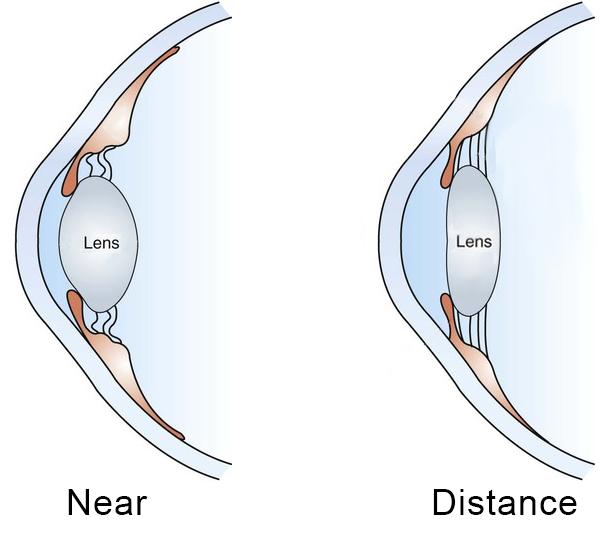
How accommodation works (and why presbyopia happens):
YOUNG EYE looking at something near:
Ciliary muscle CONTRACTS → Zonule fibres RELAX → Lens becomes FAT & round → More power → Near focus ✓
PRESBYOPIC EYE (age 40+):
Lens becomes STIFF & hard → Even when ciliary muscle contracts, lens CANNOT change shape → Near focus FAILS ✗
Key Facts
| Feature | Detail |
|---|---|
| Age of onset | Typically 40-45 years |
| Universal? | YES - affects nearly everyone by age 50 |
| Symptom | Can't read small print; holds reading material at arm's length |
| Treatment | Reading glasses, bifocals, progressive lenses, multifocal IOLs |
| Interesting exception | A myopic patient can remove their glasses to read clearly! |
Progression with age
| Age | Typical Add Power Needed |
|---|---|
| 40 | +1.00 D |
| 45 | +1.50 D |
| 50 | +2.00 D |
| 55 | +2.50 D |
| 60+ | +3.00 D (maximum) |
Snellen Chart - Testing Visual Acuity
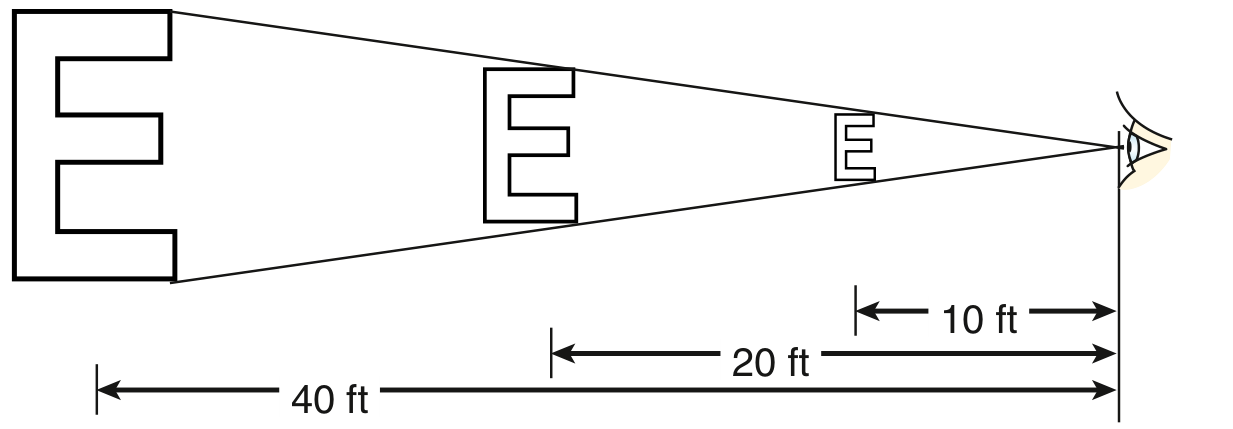
- 20/20 = Normal vision
- 20/40 = Minimum for driving (most states/countries)
- 20/200 = Legal blindness threshold
- Pinhole test: Placing a pinhole in front of the eye sharpens blurred vision caused by refractive error - if pinhole improves vision, refractive error is the cause
Treatment Summary
| Condition | Glasses Lens | Contacts | Surgery |
|---|---|---|---|
| Myopia | Concave (minus -) | Yes | LASIK, PRK, SMILE, ICL |
| Hyperopia | Convex (plus +) | Yes | LASIK (up to +4-5D), CK |
| Astigmatism | Cylindrical (toric) | Toric contacts | LASIK, PRK |
| Presbyopia | Bifocals / reading glasses | Multifocal contacts | Multifocal IOL, monovision LASIK, corneal inlays |
Quick Memory Aid
Myopia = Minus lens (concave) - can't see Mountains far away Hyperopia = plus lens (convex) - can't read the Headline close up Astigmatism = All distances blurry - football-shaped cornea Presbyopia = over 40 - Phone goes further away to read
All about Anastasia easy to understand with image
anastomosis surgery types end-to-end end-to-side side-to-side diagram medical
anastomosis vascular bowel surgical images types examples clinical
ANASTOMOSIS - Complete Guide 🔗
What is an Anastomosis?
"An anastomosis is a surgical connection between two tubes in your body. This could be between two blood vessels or between two parts of your intestines." - Cleveland Clinic
Where are Anastomoses Used?
| System | Example |
|---|---|
| Bowel / GI tract | After removing a diseased segment of bowel - rejoin the two ends |
| Blood vessels (Vascular) | Bypass surgery - join a graft to a vessel |
| Urinary | Connect ureter to bowel (ureteroileal) or bladder to urethra |
| Biliary | Join bile duct to bowel (bilioenteric) |
| Esophagus | After esophageal resection - join esophagus to stomach |
The 3 Basic Types (Configurations)
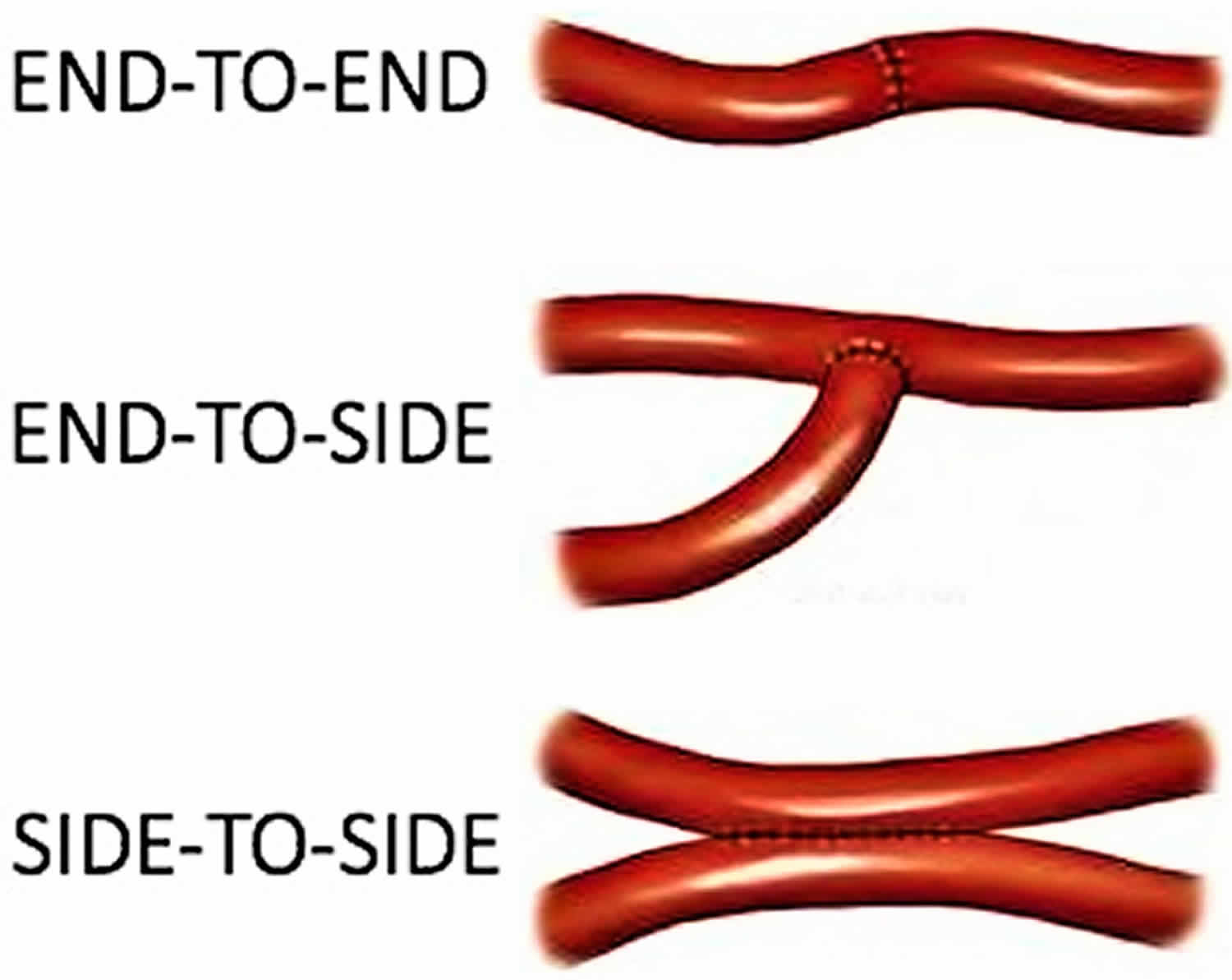
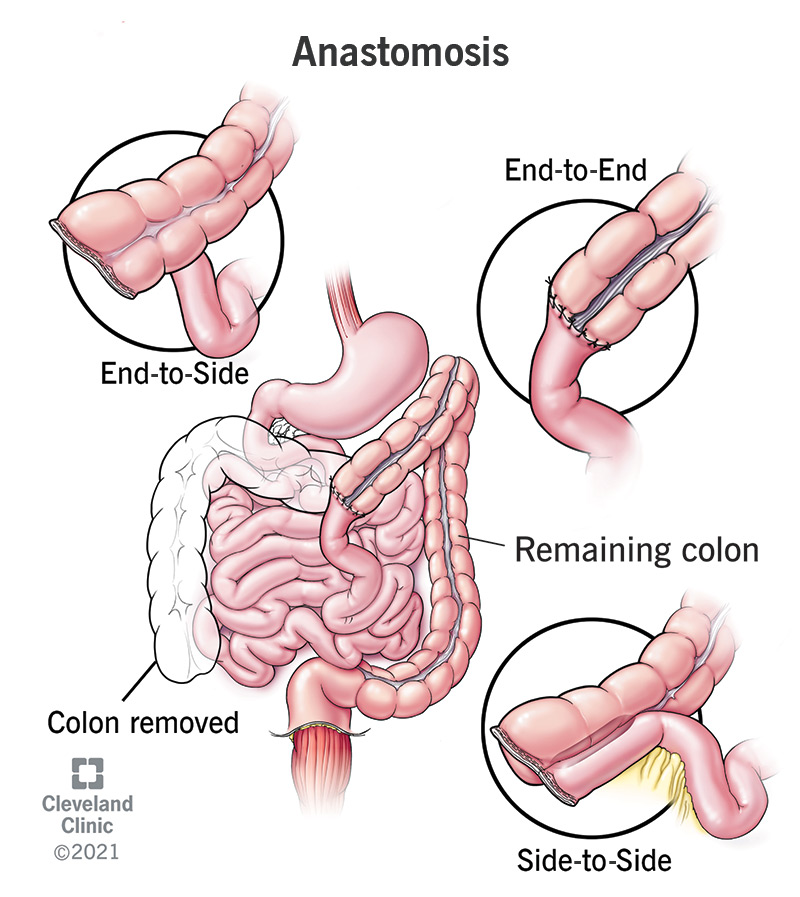
1. 🔴 End-to-End Anastomosis (EEA)
- The two open ends of two structures are joined directly together
- Like screwing two pipes end-to-end
- Best used when: Both segments are roughly the same diameter
- Common examples: Rectal resections, small bowel joins, colocolic anastomosis
2. 🔵 End-to-Side Anastomosis
- The open end of one structure is sewn into the side of another structure
- Like connecting a small pipe into the side of a larger main pipe
- Best used when: One piece of bowel is larger than the other (e.g. after chronic obstruction)
- Common examples: Ileocolic anastomosis, esophagogastric joins, liver transplant portal vein
3. 🟢 Side-to-Side Anastomosis
- The sides of two structures are sewn/stapled together, creating a wide connection
- Like joining two parallel pipes together along their lengths
- Best used when: You want a large, well-vascularized join on the antimesenteric side
- Common examples: Small bowel anastomoses, ileocolic joins (most common technique with staplers)
"The geometry of the anastomosis may be end-to-end, end-to-side, side-to-end, or side-to-side. The submucosal layer of the intestine provides the strength of the bowel wall and must be incorporated in the anastomosis to assure healing." - Schwartz's Principles of Surgery 11th Ed.
The 2 Techniques: How Surgeons Make an Anastomosis
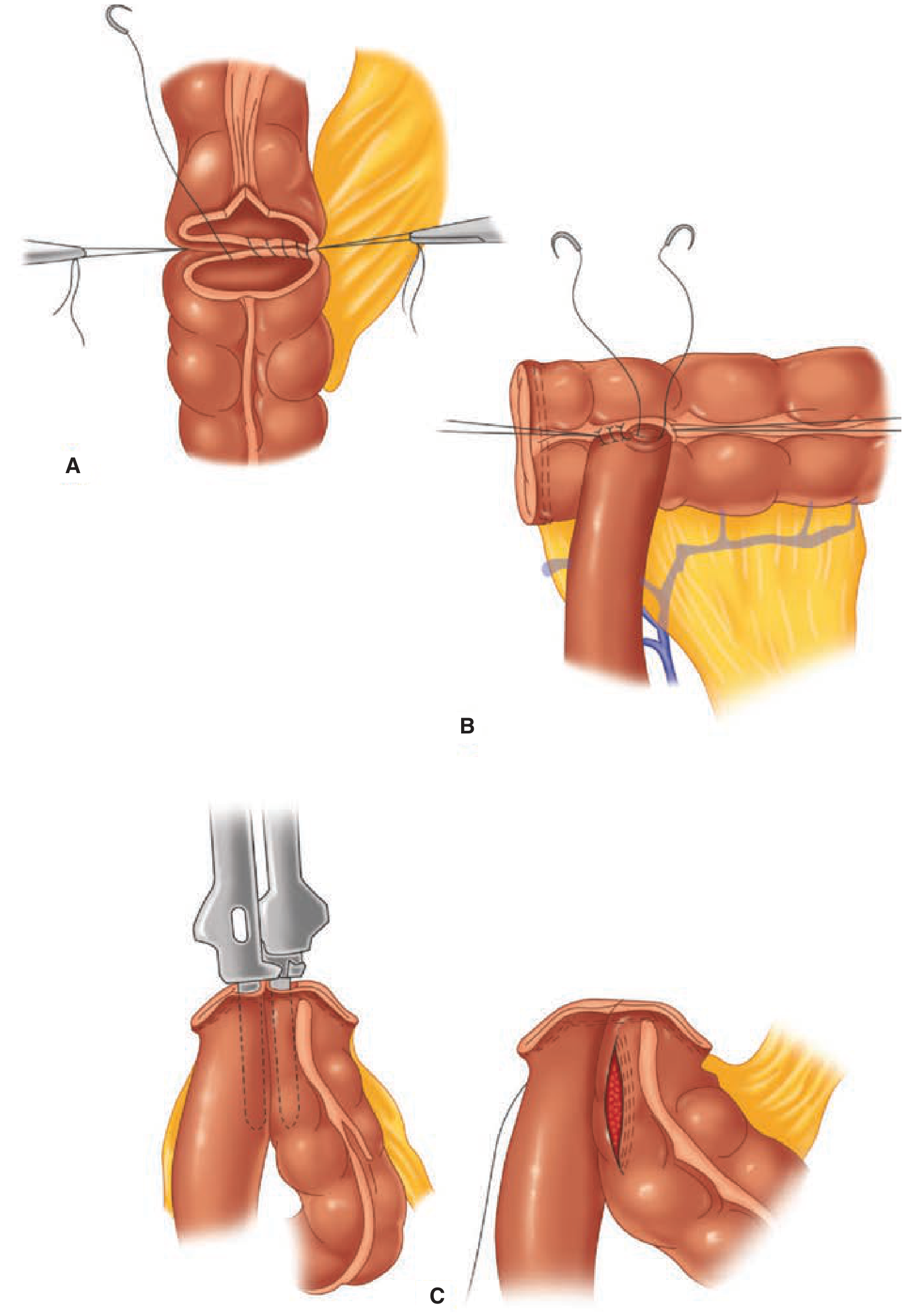
🧵 Hand-Sewn (Sutured) Technique
- Surgeon uses sutures (stitches) to sew the two ends together
- Can be done with single layer or double layer of sutures
- Sutures can be interrupted (individual knots) or continuous (running stitch)
- The submucosal layer must always be included - it provides the strength
- Can be done in any configuration (end-to-end, end-to-side, side-to-side)
🔧 Stapled Technique
- Uses mechanical stapling devices to join the structures
- Linear stapler: Cuts and staples simultaneously; used for side-to-side joins
- Circular/EEA stapler: Creates a round anastomosis; used especially for low rectal or esophageal joins where hand-sewing is physically difficult
- Double-stapling technique: Particularly used in the pelvis - rectal stump is closed with one stapler, then circular stapler is passed up through the anus to create the anastomosis
"No anastomotic technique has been proven to be superior... Accurate approximation of two well-vascularized, healthy limbs of bowel without tension almost always results in a good outcome." - Schwartz's Principles of Surgery
The Golden Rules for a Safe Anastomosis
| Rule | Why it matters |
|---|---|
| ✅ Tension-free | Pulling forces tear the join apart before it heals |
| ✅ Good blood supply | Tissue needs oxygen to heal; ischaemic ends will die and leak |
| ✅ No infection/sepsis | Bacteria produce collagenase that breaks down the healing join |
| ✅ Good nutrition | Collagen synthesis requires adequate protein and vitamins |
How an Anastomosis Heals
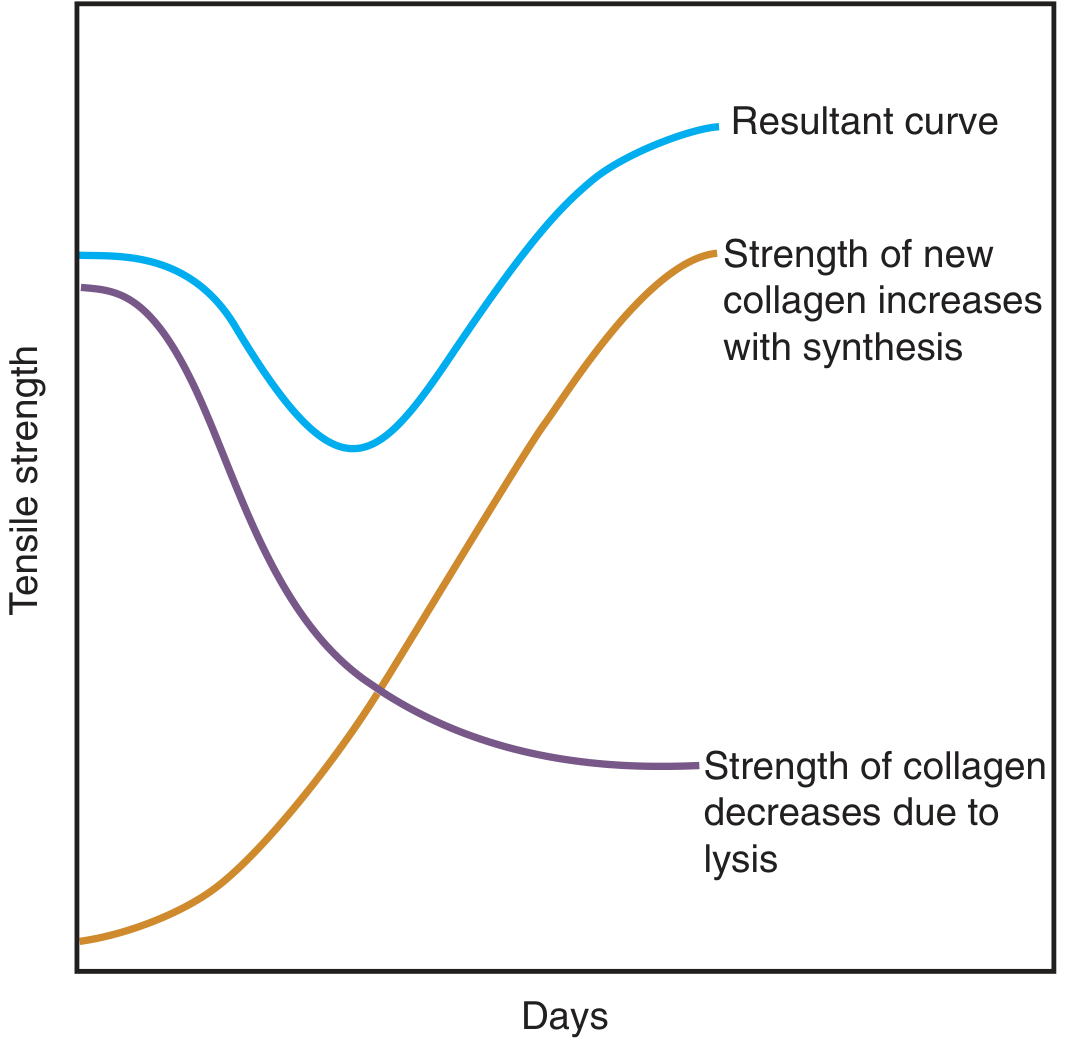
- Inflammatory phase (Days 0-3): Old collagen is broken down by collagenase - the anastomosis is at its WEAKEST. This is the danger window for leaks.
- Proliferative phase (Days 4-14): Fibroblasts make new collagen; strength rapidly increases
- Remodelling phase (Weeks to months): Collagen matures and cross-links; the join becomes strong
The Most Feared Complication: Anastomotic Leak
What is it?
"Anastomotic dehiscence is one of the most dreaded complications in colorectal surgery with rates ranging from 3% to 21%." - Sleisenger and Fordtran's GI and Liver Disease
Risk Factors for Anastomotic Leak
| Patient Factors | Technical Factors | Disease Factors |
|---|---|---|
| Malnutrition | Tension on the join | Colorectal cancer |
| Steroids/immunosuppression | Poor blood supply | Crohn's disease |
| Diabetes | Contaminated field | Irradiated bowel |
| Obesity | Very low pelvic anastomosis | Peritoneal soiling |
| Smoking | Incomplete staple ring | Obstruction above the join |
Signs of Anastomotic Leak (post-op)
- Fever on day 3-5 (classic!)
- Tachycardia
- Abdominal pain/peritonitis
- Purulent or faeculent drainage
- CT scan confirms: free fluid, gas, or extravasation of contrast
Prevention Strategies
- Diverting ileostomy (loop ileostomy): A temporary stoma is created upstream to divert faeces away from the anastomosis while it heals - if leak occurs, consequences are less severe
- Ghost/Virtual ileostomy: A vessel loop is placed around a bowel loop and brought to skin - if a leak occurs, it can quickly be converted to a real stoma at bedside
- Intraoperative leak test: Air insufflation into the rectum while the pelvis is filled with saline - bubbles = defect in the anastomosis
Special Types of Anastomoses (Named Procedures)
| Name | What it is |
|---|---|
| Ileoanal pouch anastomosis (IPAA / J-pouch) | After removing the whole colon/rectum (for ulcerative colitis), a pouch made from small bowel is joined to the anus - preserves continence |
| Bricker anastomosis | Ureter-to-ileum join (used in urinary diversion / ileal conduit) |
| Roux-en-Y anastomosis | Y-shaped join of small bowel - used in gastric bypass and hepaticojejunostomy |
| Hepaticojejunostomy | Bile duct joined to small bowel (used when CBD is blocked or injured) |
| Coronary artery bypass graft (CABG) | Vascular anastomosis - graft vessel joined to coronary artery to bypass a blockage |
Quick Summary Table
| Feature | Details |
|---|---|
| Definition | Surgical connection between two tubular structures |
| Types | End-to-End, End-to-Side, Side-to-Side |
| Techniques | Hand-sewn (sutures) vs Stapled |
| Key layer | Submucosa - must be included for strength |
| 4 golden rules | Tension-free, Good blood supply, No sepsis, Good nutrition |
| Weakest point | Days 3-5 post-op (collagenolysis > synthesis) |
| Main complication | Anastomotic leak (3-21% in colorectal surgery) |
| Protection | Diverting stoma, leak test intraoperatively |
All about Anastasia easy to understand with image
anesthesia types general local regional spinal epidural diagram medical student easy
spinal vs epidural anesthesia diagram difference labeled needle placement
general anesthesia components triad hypnosis analgesia muscle relaxation diagram
Nose anatomy and physiology with images very easy to understand
An error occurred (ValidationException) when calling the ConverseStream operation: The model returned the following errors: messages.1.content.44.image.source.base64.data: At least one of the image dimensions exceed max allowed size for many-image requests: 2000 pixels
We encountered an error while processing your request. Please try again or reach out to us for help.