Mammrry gland anatomy full in details
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
Reading File
Reading File
I now have all the detail needed for a comprehensive answer. Let me compile the full response:
Mammary Gland Anatomy - Detailed Overview
1. Position and Surface Anatomy
The mammary gland lies in the superficial fascia of the anterior thoracic wall, between the overlying skin/subdermal fat and the superficial pectoral fascia. In women, each breast is located between ribs II and VI vertically, and from the lateral border of the sternum to the mid-axillary line horizontally. The gland overlies the pectoralis major muscle (and partly the serratus anterior inferolaterally).
The superolateral portion of the gland extends around the lower margin of the pectoralis major toward the axilla - this is the axillary tail (axillary process of Spence). It may pass around the muscle margin, penetrate the deep fascia, and enter the axilla proper, although it rarely reaches the apex of the axilla.
- Sabiston Textbook of Surgery, p. 1369
- Gray's Anatomy for Students, p. 869
2. Gross Anatomy and Structural Components
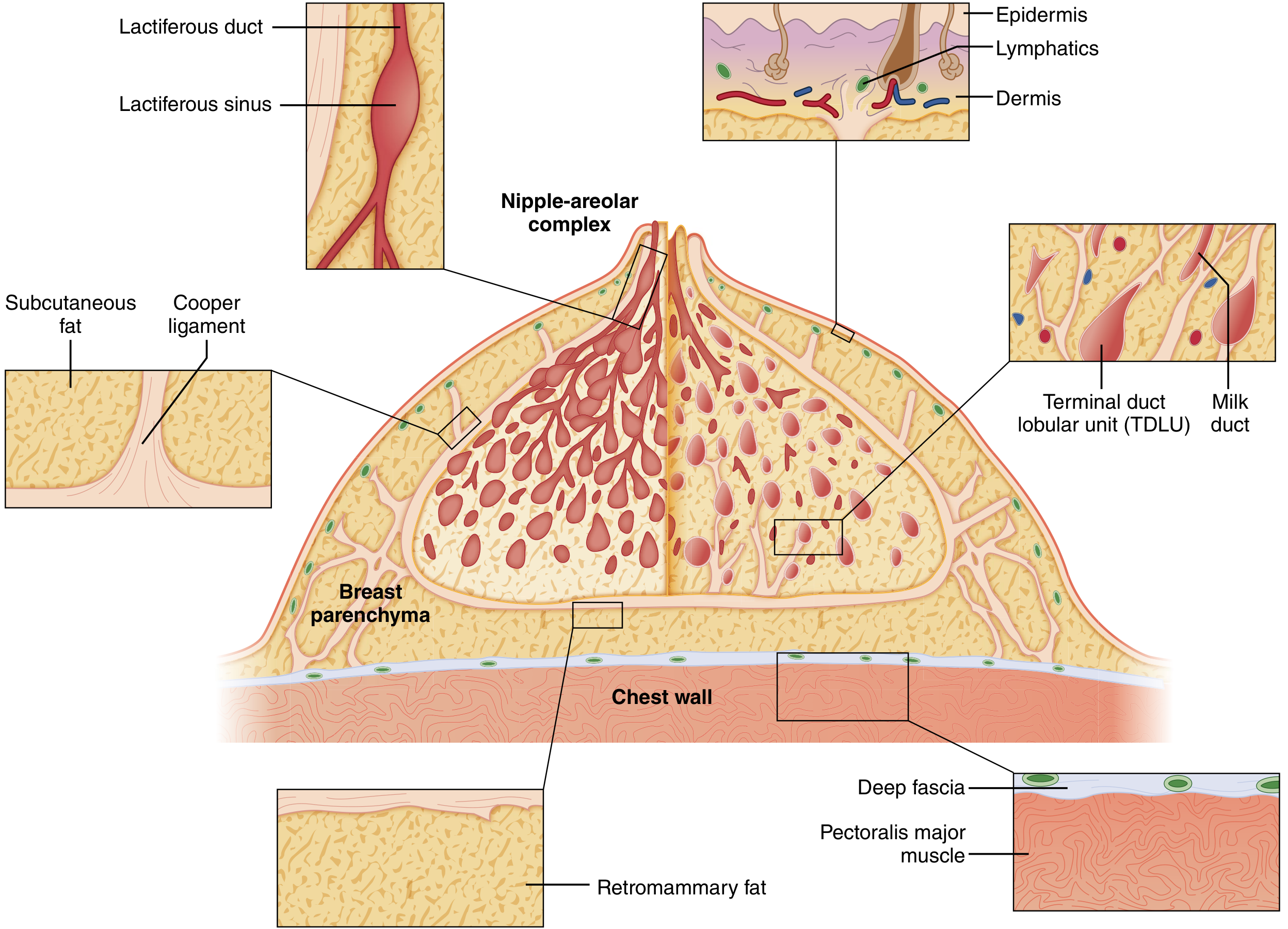
Cutaway diagram of a mature resting breast - Sabiston Textbook of Surgery
The mature breast is composed of three principal tissue types:
- Glandular epithelium (parenchyma)
- Fibrous stroma (including Cooper ligaments)
- Adipose tissue
It also contains lymphocytes and macrophages. In adolescents, epithelium and stroma predominate. After menopause, glandular structures involute and are replaced largely by adipose tissue.
The Nipple-Areolar Complex (NAC)
- The nipple is a cylindrical projection, surrounded by the areola (pigmented circular zone ~2.5 cm diameter)
- The areola contains sebaceous glands (glands of Montgomery) - small elevated nodules on the areolar surface that lubricate the nipple during lactation
- The nipple contains 15-20 lactiferous duct openings, smooth muscle fibres (causing erection on stimulation), and abundant sensory nerve endings
The Duct System
The glandular apparatus is organized as a branching, radial ductal system spreading outward from the NAC - like an inverted tree:
| Level | Structure |
|---|---|
| Nipple surface | 15-20 lactiferous duct orifices |
| Subareolar | Lactiferous sinuses (dilated ampullae) |
| Intermediate | Major collecting ducts, segmental ducts |
| Peripheral | Terminal ducts |
| Lobule | Intralobular terminal ductules and acini |
There are 15-20 lobes, each draining by a single lactiferous duct at the nipple. Each major duct has a dilated lactiferous sinus (ampulla) below the NAC. Ducts progressively branch and terminate in the terminal duct lobular units (TDLUs).
Each ductal system is functionally independent - there is no cross-communication between adjacent systems.
- Sabiston Textbook of Surgery, p. 1369-1370
3. The Terminal Duct Lobular Unit (TDLU)
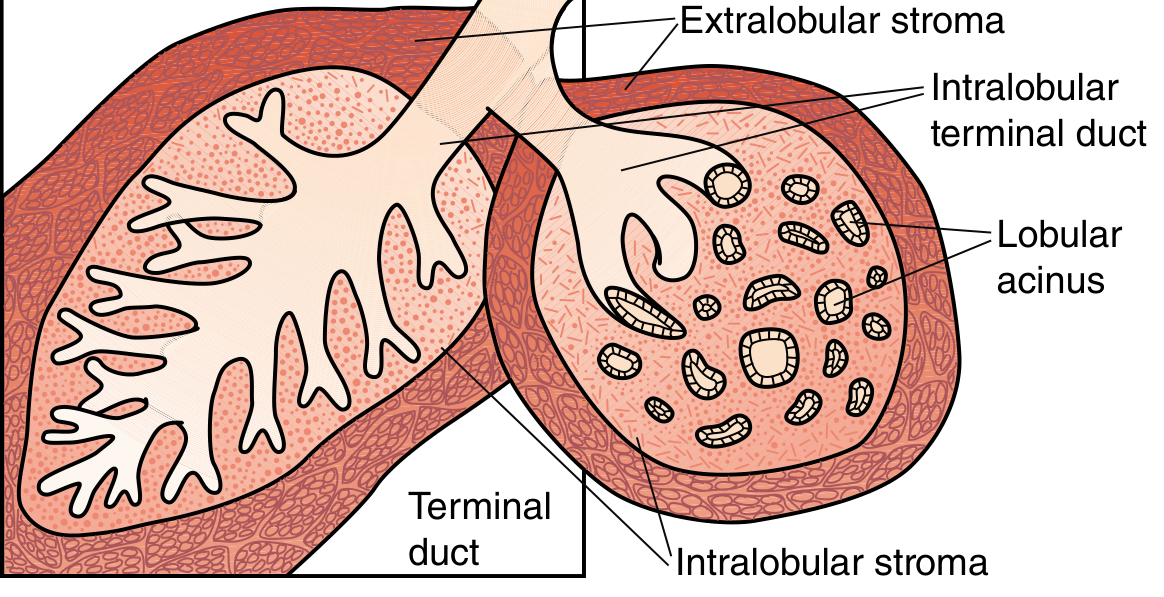
TDLU showing intralobular terminal duct, lobular acini, intralobular stroma, and extralobular stroma - Sabiston Textbook of Surgery
The TDLU is the functional unit of the breast and the site of most pathologic processes:
- Each lobule consists of 10-100 acini (blind-ended saccules) opening into an intralobular terminal duct
- Acini are the milk-forming units of the lactating breast
- Invested in specialized loose intralobular stroma containing capillaries, lymphocytes, plasma cells, and mononuclear cells
- Surrounded by denser, less cellular interlobular (extralobular) stroma and fat
The ductal and acinar epithelium has two cell layers:
- Inner luminal epithelial cells (cuboidal to columnar) - secretory
- Outer myoepithelial cells - contractile, propel milk toward nipple
Outside these layers is a continuous basement membrane (containing laminin, type IV collagen, proteoglycans). This basement membrane is the critical boundary between in-situ and invasive carcinoma.
- Sabiston Textbook of Surgery, p. 1370-1371
- Histology: A Text and Atlas (Pawlina), p. 2361
4. Suspensory Ligaments of Cooper
Multiple fibrous septa run from the deep fascia (overlying pectoralis major) through the breast parenchyma to anchor into the overlying dermis. These are the suspensory ligaments of Cooper (Cooper's ligaments).
- They give shape and structural support to the breast
- Because they anchor into skin, infiltration by carcinoma or breast oedema causes skin dimpling or "peau d'orange" (orange-peel skin) appearance, which is a clinical sign of breast cancer
A distinct retromammary space (potential space) lies between the posterior surface of the breast (deep fascia) and the anterior surface of the pectoralis major fascia, allowing some mobility of the gland.
- Sabiston Textbook of Surgery, p. 1369
5. Blood Supply
Arterial supply (from three main sources):
| Artery | Contribution |
|---|---|
| Internal thoracic (mammary) artery - perforating branches through 2nd-4th intercostal spaces | ~60% of blood supply (medial and central breast) |
| Lateral thoracic artery (branch of axillary) | Superolateral breast |
| Thoracoacromial artery (pectoral branch, axillary) | Upper breast |
| Anterior intercostal arteries (branches of internal thoracic/musculophrenic) | Lateral breast |
| Subscapular and thoracodorsal arteries | Lateral breast |
Branches travel along alveolar ducts and reach capillary beds surrounding the acini.
Venous drainage:
Veins basically follow the arteries - drain to the axillary vein (lateral), internal thoracic veins (medial), and intercostal veins (posteriorly to azygos/hemiazygos). The latter route is relevant as a pathway for haematogenous metastasis to vertebrae and lungs.
- Histology: A Text and Atlas (Pawlina), p. 2317
- Fischer's Mastery of Surgery, p. 2150
6. Lymphatic Drainage
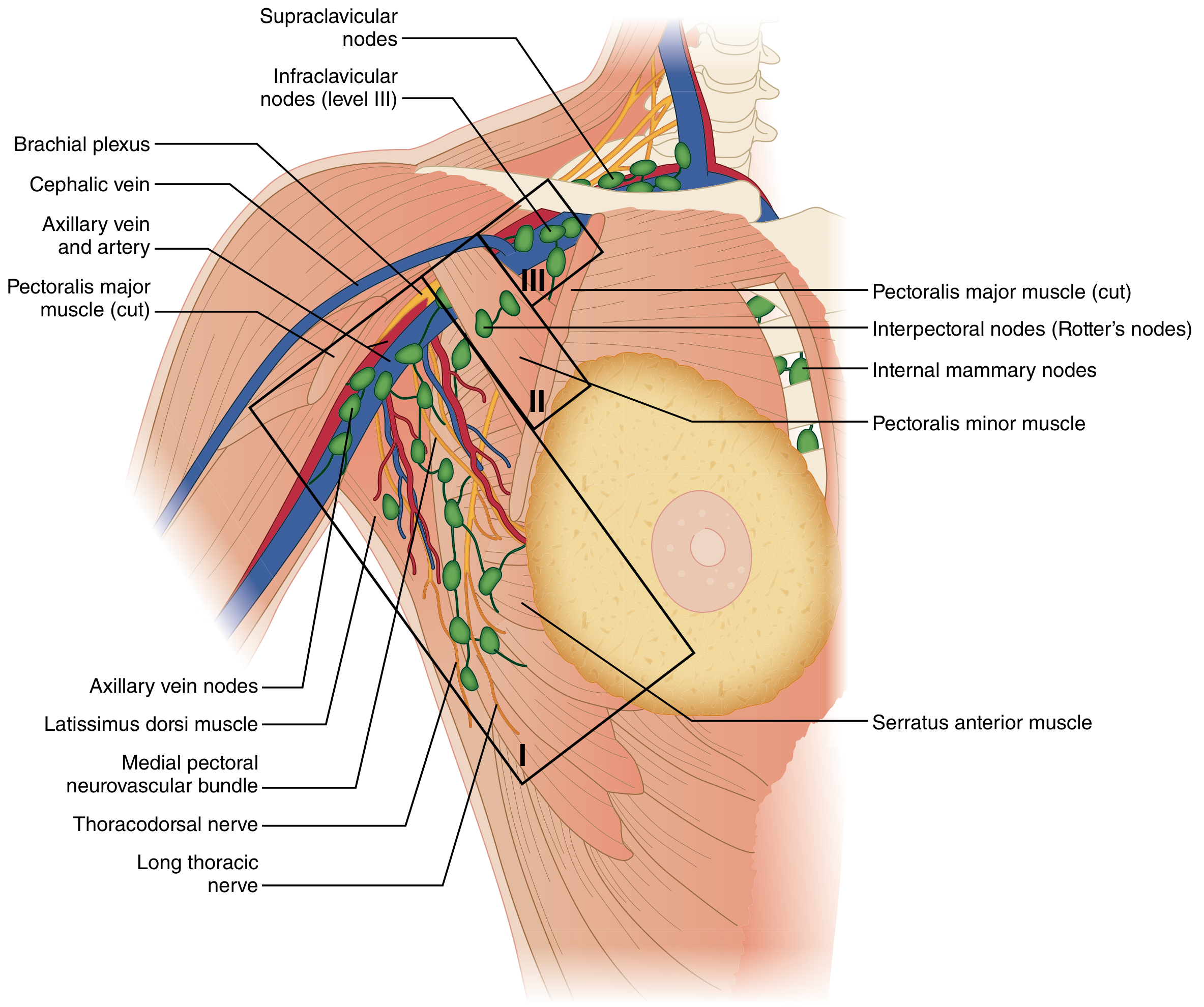
Lymphatic drainage of the breast with axillary nodal levels - Sabiston Textbook of Surgery
Lymphatic capillaries begin around the acini in the intralobular connective tissue and converge into larger vessels that drain primarily to the axilla (~75%) and medially to parasternal (internal mammary) nodes.
Axillary Nodal Levels (defined by relationship to pectoralis minor):
| Level | Location | Description |
|---|---|---|
| Level I | Lateral to pectoralis minor | Anterior/pectoral, posterior/subscapular, lateral groups - the first echelon in most cancers |
| Level II | Behind pectoralis minor | Includes Rotter's nodes (interpectoral nodes) between pectoralis major and minor |
| Level III | Medial to pectoralis minor | Infraclavicular (apical) nodes; highest axillary level |
| - | Beyond level III | Supraclavicular nodes - outside axilla proper |
Medial drainage path goes to internal mammary (parasternal) nodes along the internal thoracic vessels (2nd-4th intercostal spaces), particularly from the medial and inferior breast. This is an important route for metastatic spread.
The sentinel lymph node (SLN) - the first node in the drainage chain - is most commonly found in the Level I external mammary group.
Key surgical nerves in the axilla (must be preserved during lymphadenectomy):
-
Long thoracic nerve - serratus anterior (damage = winged scapula)
-
Thoracodorsal nerve - latissimus dorsi (damage = weakness in arm adduction)
-
Medial pectoral nerve - pectoralis major
-
Intercostobrachial nerves - sensory to medial upper arm
-
Sabiston Textbook of Surgery, p. 1371-1372
7. Nerve Supply
The breast is innervated by the anterior and lateral cutaneous branches of the 2nd to 6th intercostal nerves (T2-T6):
-
Convey afferent (sensory) and sympathetic fibres
-
The 4th intercostal nerve (T4) typically provides the principal sensory supply to the nipple-areola complex
-
Secretory function of the gland is primarily hormonal, not neural
-
However, afferent impulses from suckling trigger the neuroendocrine reflex arc - stimulating pituitary prolactin (PRL) release and oxytocin release (milk let-down)
-
Histology: A Text and Atlas (Pawlina), p. 2317
8. Histology of the Mammary Gland
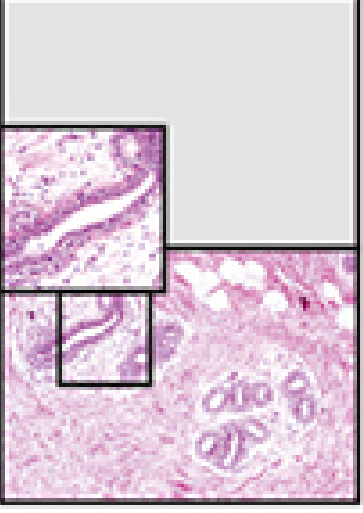
Inactive mammary gland (H&E ×200) showing ducts (D), loose intralobular connective tissue (CT/L) with lymphocytes and plasma cells, and dense interlobular connective tissue (CT/D) with adipocytes - Histology: A Text and Atlas
Inactive/Resting State
- Sparse parenchyma composed mostly of duct elements surrounded by loose connective tissue
- Lobular units (TDLUs) contain small ducts lined by cuboidal epithelium subtended by myoepithelial cells
- True alveoli are absent; only alveolar precursors as cellular thickenings of duct walls
- Loose intralobular stroma (contains scattered lymphocytes and plasma cells) vs. dense interlobular stroma (contains adipocytes and larger ducts)
Histological Cell Types:
| Cell | Location | Function |
|---|---|---|
| Luminal epithelial cells | Inner layer of ducts and acini | Secretory (protein and lipid) |
| Myoepithelial cells | Outer/basal layer | Contractile, milk ejection |
| Fibroblasts | Stroma | Structural support |
| Lymphocytes, Plasma cells | Intralobular stroma | Immune (IgA secretion into milk) |
| Adipocytes | Interlobular stroma | Fat storage, paracrine signaling |
9. Development and Hormonal Regulation
Embryology
- The milk line (mammary ridge) forms as an ectodermal thickening from axilla to inguinal region at week 4-5 of gestation
- By week 9, the ridge involutes except for the pectoral segment (forms one pair of glands)
- Failure of involution → polymastia (accessory breasts) or polythelia (accessory nipples)
- Failure of milk bud development → amastia/athelia
- At birth, maternal hormones/prolactin may cause transient neonatal secretion (witch's milk)
Pubertal Development (Thelarche)
- Onset: ages 9-12 in girls (in the US)
- Driven by estrogen (ductal elongation and branching) and progesterone (lobulo-alveolar development)
- Initial growth occurs under the influence of ovarian estrogen and progesterone
Cyclical Changes (Menstrual Cycle)
- Follicular phase: Estrogen stimulates proliferation of lactiferous duct components
- Luteal phase (post-ovulation): Progesterone stimulates alveolar growth; intralobular stroma becomes edematous; breast feels fuller/tender
Pregnancy and Lactation
-
Continuous estrogen + progesterone (corpus luteum, placenta) cause massive increase in TDLUs
-
Also requires: prolactin (anterior pituitary), human chorionic somatomammotropin/hCS (placenta), and adrenal glucocorticoids
-
Alveoli proliferate extensively; myoepithelial cells also proliferate
-
Milk secretion mechanism:
- Protein component: synthesized and released by merocrine (exocytosis) secretion
- Lipid component: released by apocrine secretion (lipid droplets surrounded by apical membrane)
-
Colostrum (first 2-3 days): alkaline, high protein/vitamin A/sodium/chloride, rich in antibodies (IgA) providing passive immunity to the neonate; produced by plasma cells in breast stroma
-
Maintained by suckling-induced prolactin and oxytocin release
-
Histology: A Text and Atlas (Pawlina), p. 2313-2364
-
Sabiston Textbook of Surgery, p. 1372
10. Post-Menopausal Involution
After menopause, with loss of ovarian hormone stimulation:
-
Secretory cells of TDLUs degenerate and disappear; only duct elements remain (resembles male breast histologically)
-
Connective tissue undergoes degenerative changes: decreased fibroblasts, collagen, elastic fibers
-
Glandular parenchyma largely replaced by adipose tissue, making the breast softer and less dense on mammography
-
Histology: A Text and Atlas (Pawlina), p. 2317
Summary Table
| Feature | Detail |
|---|---|
| Position | Ribs II-VI, over pectoralis major |
| Tissue types | Glandular epithelium, fibrous stroma, fat |
| Lobes | 15-20, each with one lactiferous duct |
| Functional unit | TDLU (terminal duct lobular unit) |
| Supportive ligaments | Cooper's suspensory ligaments |
| Axillary process | Tail of Spence (superolateral extension) |
| Arterial supply | Internal thoracic (main), lateral thoracic, intercostals |
| Venous drainage | Axillary, internal thoracic, intercostal veins |
| Lymphatics | 75% axillary (levels I-III), 25% internal mammary nodes |
| Nerve supply | T2-T6 intercostal (anterior + lateral cutaneous branches) |
| Secretion type | Merocrine (protein) + Apocrine (lipid) |
This is a shared conversation. Sign in to Orris to start your own chat.