Vanish twin
Reading File
Finding Sources
Finding Sources
Searching PubMed
"vanishing twin" syndrome
Reading File
Reading File
Finding Sources
Reading File
Loading Image
Loading Image
Here is a thorough overview of vanishing twin syndrome (VTS), sourced from Creasy & Resnik's Maternal-Fetal Medicine.
Vanishing Twin Syndrome
Definition
Vanishing twin syndrome (VTS) is the spontaneous loss of one embryo or fetus during the first trimester of a twin or multiple pregnancy. The remaining gestational sac and embryo are resorbed, leaving no detectable remnant on later ultrasound - hence the twin appears to have "vanished."
A related term, fetus papyraceus, refers to a compressed, mummified fetal remnant from a co-twin who died in utero, typically between 12 and 20 weeks' gestation (early second trimester). Unlike the first-trimester vanishing twin, this fetus is not fully resorbed.
Epidemiology
- VTS is reported to occur in approximately 21% of twin pregnancies
- Historically considered to have no detrimental effect on the surviving fetus
- The incidence of any single twin demise (across all gestational ages) is estimated at ~6% of all twin pregnancies
Pathogenesis
The exact etiology is unknown in most cases. Contributing factors include:
| Category | Examples |
|---|---|
| Fetal | Discordant chromosomal anomalies, discordant structural abnormalities, discordant infections, discordant fetal growth |
| Placental | Uneven placental sharing, peripheral cord insertion, placental implantation anomalies |
| Maternal | Preeclampsia, thrombophilia, placental abruption |
| Iatrogenic | Selective feticide, laser therapy for twin-to-twin transfusion syndrome (TTTS) |
Placental and Pathologic Findings
What is found at delivery depends on the gestational age at fetal death and the duration of in utero retention:
- Early first-trimester demise: The twin may vanish completely with no morphologic residue. Genetic evidence may persist as restricted placental chimerism
- Partial resorption: A plaque-like thickening within the membranes or on the fetal surface of the placenta may be the only sign; ocular pigment may be the only clue
- Fetus papyraceus (second-trimester death): The deceased fetus is progressively compressed by the growing co-twin
Fig. 5.16 - Diamniotic-dichorionic placenta from a VTS pregnancy. (A) Apparently singleton placenta with focal membrane thickening. (B) A separate sac containing a macerated, malformed embryo (the vanished twin):
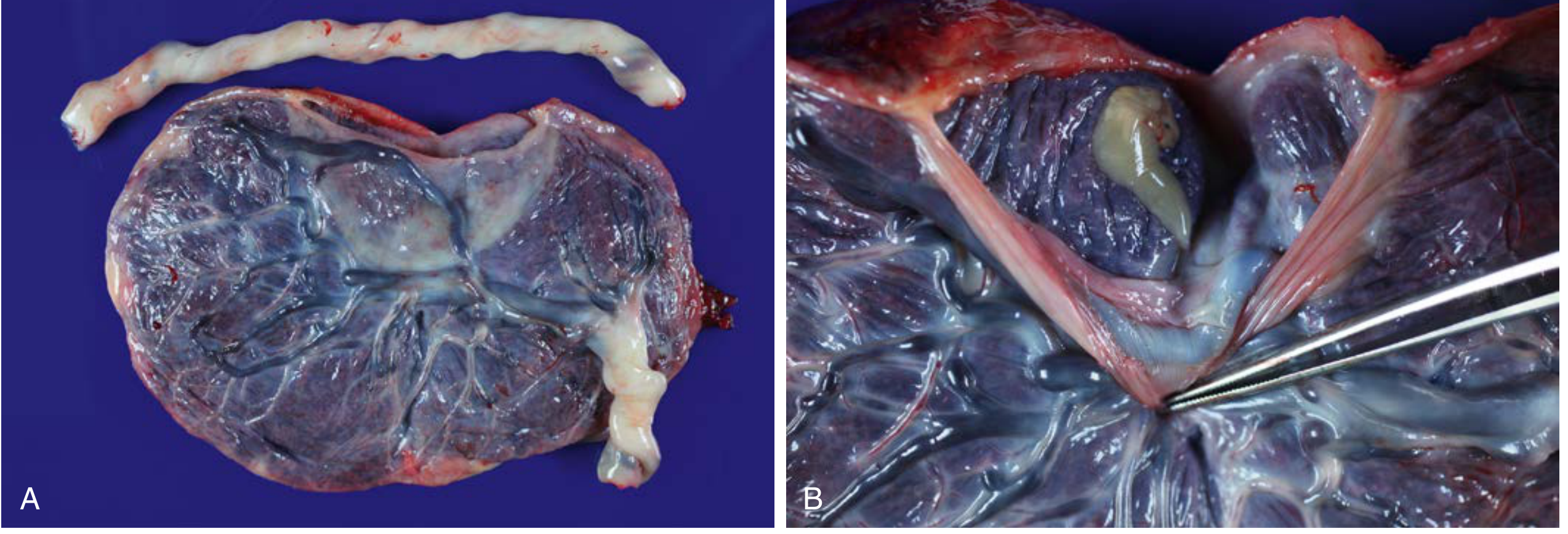
Fig. 5.17 - Diamniotic-dichorionic placenta with fetus papyraceus. (A) Plaque-like thickening on the fetal side. (B) The partially mummified fetus:

Outcome for the Surviving Twin
Role of Chorionicity (Most Important Factor)
Chorionicity is the single most important determinant of outcome after co-twin demise, due to shared vascular connections in monochorionic placentas.
Monochorionic vs. Dichorionic Outcomes
| Outcome | Monochorionic | Dichorionic |
|---|---|---|
| Co-twin death rate after one fetal loss | ~15% | ~3% |
| Abnormal neonatal cranial imaging | 34% | 16% |
| Serious neurologic abnormality (e.g., multicystic encephalomalacia) | 26% | 2% |
| Risk of small for gestational age | Increased (inversely related to gestational age at demise) | Lower |
- In monochorionic pregnancies, neurologic injury can occur as early as 12 weeks' gestation - there is no safe gestational age cutoff
- Neurologic injury risk is highest when monochorionic co-twin demise occurs between 28-33 weeks' gestation (compared to >34 weeks)
Mechanism of Neurologic Injury
The leading hypothesis is acute fetal hypotension at the moment of co-twin death. Studies using fetal blood sampling showed all surviving co-twins became anemic immediately after the co-twin's death - consistent with acute blood loss from the survivor into the deceased twin through placental anastomoses (not pre-existing anemia).
Other Risks
- Preterm birth: Increased risk of both medically indicated and spontaneous preterm birth
- Small for gestational age (SGA): Shown in a series of 642 surviving fetuses from VTS pregnancies; risk inversely correlated with gestational age at co-twin demise
Impact on Prenatal Screening (NIPT/cfDNA)
VTS is a recognized source of false-positive cell-free DNA (cfDNA/NIPT) results. The demised twin's DNA continues to circulate in the maternal bloodstream and can be misidentified as an aneuploid fetus. VTS is listed alongside confined placental mosaicism, maternal chromosomal abnormalities, and maternal malignancy as a cause of discordant NIPT results.
Careful ultrasound is recommended before interpreting any discordant cfDNA result to rule out a vanishing twin.
Summary
| Feature | Detail |
|---|---|
| Timing of "vanishing" | First trimester (before ~12 weeks) |
| Incidence | ~21% of twin pregnancies |
| Chorionicity matters? | Yes - monochorionic = much higher risk |
| Key neurologic risk | Multicystic encephalomalacia in monochorionic survivor |
| cfDNA/NIPT implication | Can cause false-positive aneuploidy screening |
- Creasy & Resnik's Maternal-Fetal Medicine: Principles and Practice (Blocks 2 and 8)
This is a shared conversation. Sign in to Orris to start your own chat.