Ceftriaxone bd vs od
Reading File
Searching the Web
ceftriaxone once daily vs twice daily dosing pharmacodynamics
Finding Sources
Searching PubMed
ceftriaxone once daily twice daily pharmacokinetics clinical outcomes
Reading Web Page
https://pmc.ncbi.nlm.nih.gov/articles/PMC9331887
Here is a thorough breakdown of the ceftriaxone OD vs BD debate:
Ceftriaxone: Once Daily (OD) vs Twice Daily (BD)
Pharmacokinetic Basis
Ceftriaxone is a time-dependent antibiotic (like all beta-lactams). Its efficacy depends on the time that free (unbound) drug concentration remains above the MIC - the pharmacodynamic target is typically fT>MIC for 60-70% of the dosing interval.
Key PK properties that make OD dosing possible:
- Half-life: 7-8 hours (the longest of all cephalosporins)
- Protein binding: 85-95% (concentration-dependent - decreases at higher concentrations, releasing more free drug)
- Biliary + renal dual elimination - not renally adjusted
- No dose adjustment needed for isolated renal or hepatic impairment
These properties allow a single daily dose to maintain drug levels above the MIC for the required fraction of the dosing interval for most susceptible organisms - Katzung's Pharmacology notes that ceftriaxone "can be injected once every 24 hours."
Standard Dosing (OD): When to Use What Dose
| Indication | Dose |
|---|---|
| CAP (inpatient, non-severe) | 1-2 g OD |
| UTI / pyelonephritis | 1 g OD |
| Intra-abdominal infections | 1-2 g OD |
| Meningitis | 2 g BD (high CNS penetration required) |
| Endocarditis (streptococcal, HACEK) | 2 g OD |
| Critically ill (any infection) | Consider 2 g OD or 2 g BD |
When BD Dosing May Be Justified (2 g OD → 1 g BD or 2 g BD)
BD dosing is NOT routinely superior to OD but becomes relevant in specific scenarios:
-
Augmented renal clearance (ARC) - seen in young critically ill patients, sepsis, trauma, burns. Drug is cleared faster than normal, reducing fT>MIC. A PK model shows 1 g BD provides better coverage than 2 g OD in ARC.
-
Higher MIC pathogens - when the causative organism's MIC is near the susceptibility breakpoint (e.g., MIC = 1-2 mg/L), splitting the dose ensures more consistent time above MIC.
-
CNS infections / meningitis - standard guideline recommendation is 2 g IV BD (or even more frequent dosing in some protocols) because CSF penetration is limited and you need sustained levels well above the MIC.
-
Severe/critically ill patients - ICU patients often have volume redistribution, hypoalbuminemia (which alters protein binding and increases free drug but also increases clearance), making PK unpredictable.
-
Obesity - obese patients (BMI ≥30) receiving only 1 g OD showed significantly higher clinical failure rates (62% vs 40%), suggesting higher or split dosing may be needed.
Head-to-Head Evidence: 2 g OD vs 1 g BD
A retrospective study comparing 1 g BD vs 2 g OD in aspiration pneumonia (Mie University Hospital) found:
- Early improvement was better with 2 g OD - in vitro hollow-fiber models showed 2 g OD achieved 1-log bacterial kill within 24 hours and sustained it to 72 hours
- 1 g BD showed initial bacterial growth in the first 12 hours before achieving 1-log kill, with effect waning after 36 hours
- No significant difference in clinical outcomes overall in the retrospective cohort
- Cholelithiasis (a known ceftriaxone side effect from biliary sludge) was more common with 2 g OD, though the mechanism remains unclear
In acute cholangitis (Toki et al., 2019), no difference in clinical efficacy was found between 2 g OD and 1 g BD. In CAP, a meta-analysis of 24 RCTs found no significant mortality difference between 1 g, 2 g OD, and 1 g BD.
Practical Summary
| Scenario | Preferred Regimen |
|---|---|
| Most community infections (CAP, UTI, IAI) | 1-2 g OD - standard of care |
| Meningitis | 2 g BD (guideline-mandated) |
| Critically ill with ARC | Consider 1 g BD or 2 g BD |
| High MIC organisms | Consider BD dosing |
| Obesity (BMI ≥30) | Use 2 g OD minimum |
| Non-critically ill, normal renal function | OD dosing is sufficient and preferred |
Bottom line: Ceftriaxone OD is the evidence-based standard for most infections due to its long half-life. BD dosing is not simply "more is better" - it is specifically indicated for meningitis, critically ill patients with ARC, and situations where the MIC is near the breakpoint. For routine infections, 2 g OD is preferred over 1 g BD as it provides more consistent bactericidal activity (based on in vitro data) without increasing adverse effects.
Cause of generalized hyoerhydrosis
Reading File
Finding Sources
Searching the Web
causes of generalized hyperhidrosis secondary systemic classification
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
I have the detailed textbook content now. Here is the full answer:
Causes of Generalized Hyperhidrosis
Generalized hyperhidrosis is almost always secondary - it reflects a systemic disturbance rather than a primary sweat gland disorder. Primary hyperhidrosis is typically focal (palms, soles, axillae). Generalized sweating, especially nocturnal or asymmetric sweating, should always prompt a search for an underlying cause.
(Fitzpatrick's Dermatology): "Secondary hyperhidrosis was more often unilateral or asymmetric, generalized, and present nocturnally."
Classification by Source of Neural Drive
Sweating can be driven at multiple levels of the neuroaxis:
| Level | Example |
|---|---|
| Cortical | Emotional/anxiety states |
| Hypothalamic | Thermoregulatory (fever, menopause) |
| Medullary | Gustatory sweating |
| Spinal cord | Spinal cord injury, syringomyelia |
| Local | Eccrine nevus, compensatory |
Causes by System (Mnemonics: NEIM-D)
1. Neurological (32% of secondary cases)
- Stroke, brain tumors, head trauma
- Spinal cord injury, syringomyelia
- Parkinson's disease
- Peripheral neuropathy (autonomic)
- Familial dysautonomia (Riley-Day syndrome)
- Diencephalic epilepsy (episodic hypothermia + hyperhidrosis)
- Agenesis of corpus callosum, brainstem tumors
2. Endocrine / Metabolic (57% of secondary cases - the most common cause)
- Hyperthyroidism - classic cause
- Diabetes mellitus - especially hypoglycemia (adrenergic surge)
- Pheochromocytoma - present in ~71% of patients with pheo
- Acromegaly / Hyperpituitarism
- Carcinoid syndrome
- Menopause - hot flushes with thermoregulatory instability
- Pregnancy
- Hypoglycemia (any cause - insulin, sulphonylureas)
- Obesity
3. Infections
- Tuberculosis - classic cause of night sweats
- Brucellosis
- HIV / AIDS
- Endocarditis (subacute)
- Malaria
- Any cause of fever (pyrogen-driven hypothalamic reset)
4. Malignancy
- Lymphoma (Hodgkin's and non-Hodgkin's) - night sweats are a B symptom
- Pheochromocytoma (also endocrine)
- Carcinoid tumors
- Intrathoracic / mediastinal tumors
- Renal cell carcinoma
- Leukemia
5. Drugs / Medications
| Category | Examples |
|---|---|
| Antidepressants | SSRIs (fluoxetine, venlafaxine), TCAs |
| Opioids | Morphine, tramadol |
| Antipyretics | Aspirin, NSAIDs |
| Cholinergic agents | Pilocarpine, physostigmine |
| Antihypertensives | Propranolol, clonidine (paradoxically) |
| Hormonal agents | Tamoxifen, GnRH agonists |
| Antidiabetics | Insulin, sulphonylureas (via hypoglycemia) |
| Antibiotics / antivirals | Various |
| Topical glucocorticoids, isotretinoin |
6. Cardiovascular
- Cardiovascular shock / syncope
- Respiratory failure
- Severe acute pain (sympathetic surge)
- Heart failure
7. Psychiatric
- Anxiety disorders
- Panic disorder
8. Withdrawal states
- Alcohol withdrawal
- Opioid withdrawal
- Benzodiazepine withdrawal
Key Clinical Features Pointing to Secondary (Generalized) Hyperhidrosis
| Feature | Significance |
|---|---|
| Nocturnal sweating | Strongly suggests secondary cause (TB, lymphoma, pheo) |
| Onset after age 25 | More likely secondary |
| No family history | More likely secondary |
| Asymmetric or generalized pattern | More likely secondary |
| Associated systemic symptoms | Weight loss (malignancy), palpitations (pheo/thyroid), fever (infection) |
Key Investigations to Consider
- TFTs (thyroid)
- Fasting glucose / HbA1c
- Urine catecholamines / metanephrines (pheo)
- ESR, CXR (TB, lymphoma)
- HIV serology
- IGF-1 (acromegaly)
- CBC + blood film
Sources: Fitzpatrick's Dermatology; Dermatology 2-Volume Set 5e (Elsevier)
Muscles of hand
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Reading File
Loading Image
Reading File
Loading Image
Here is a complete, well-illustrated reference on the intrinsic muscles of the hand.
Intrinsic Muscles of the Hand
Source: THIEME Atlas of Anatomy - General Anatomy and Musculoskeletal System
The intrinsic muscles of the hand are divided into four groups:
- Thenar muscles (thumb eminence)
- Hypothenar muscles (little finger eminence)
- Lumbricals (4 muscles)
- Interossei (dorsal + palmar)
Thenar and Hypothenar Muscles
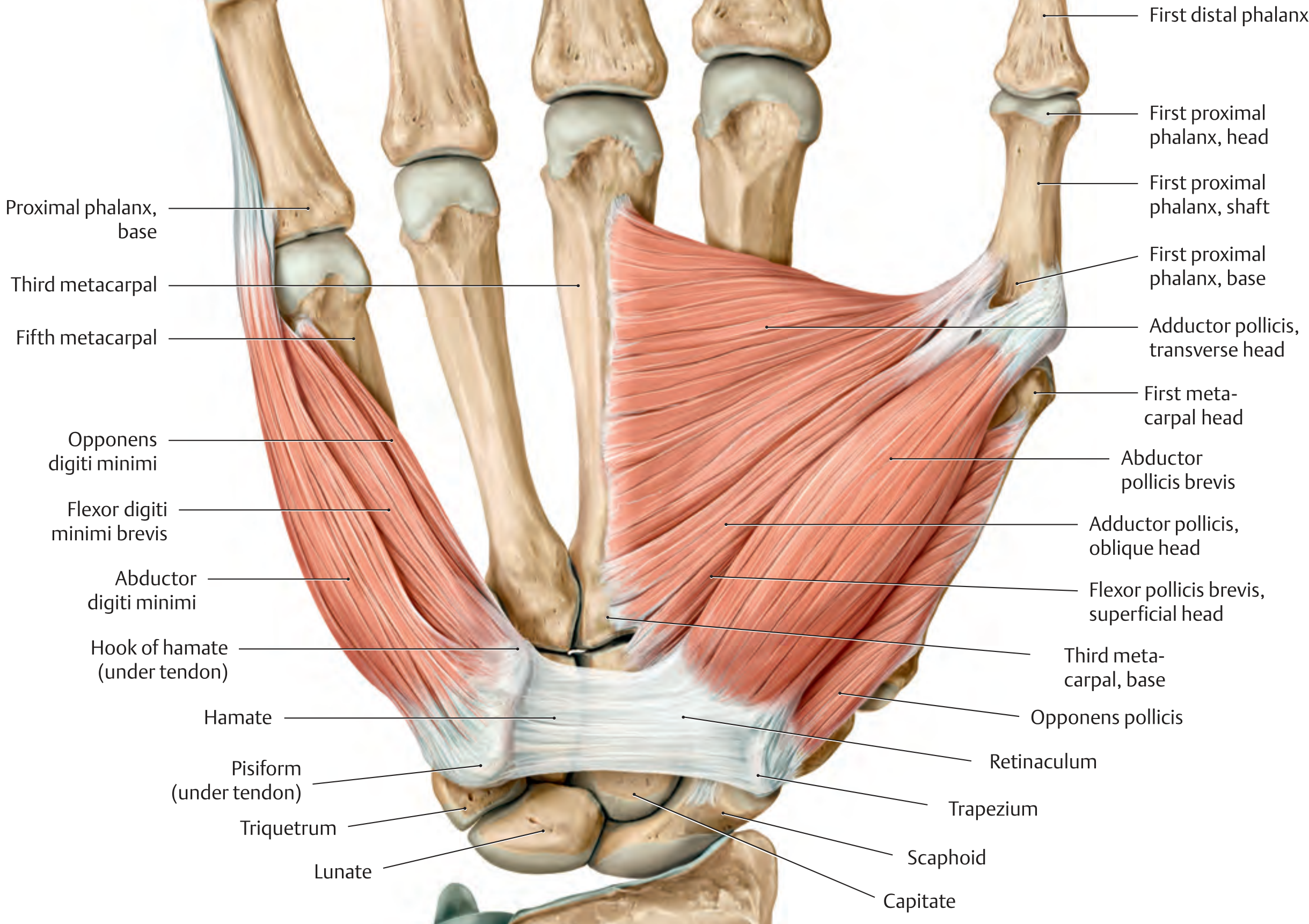
GROUP 1: Thenar Muscles (4 muscles)
| Muscle | Origin | Insertion | Action | Nerve |
|---|---|---|---|---|
| Abductor pollicis brevis | Scaphoid, trapezium, flexor retinaculum | Base of proximal phalanx of thumb (radial sesamoid) | Abduction of thumb | Median (C8, T1) |
| Flexor pollicis brevis | Superficial head: flexor retinaculum; Deep head: capitate, trapezium | Base of proximal phalanx of thumb (radial sesamoid) | CMC: flexion, opposition; MCP: flexion | Superficial head: Median; Deep head: Ulnar (C8, T1) |
| Opponens pollicis | Trapezium | Radial border of 1st metacarpal | CMC: opposition | Median (C8, T1) |
| Adductor pollicis | Transverse head: palmar surface of 3rd metacarpal; Oblique head: capitate, base of 2nd & 3rd metacarpals | Base of proximal phalanx of thumb (ulnar sesamoid) | CMC: opposition; MCP: flexion | Ulnar (C8, T1) |
Memory aid: All thenar muscles = Median nerve, EXCEPT adductor pollicis = Ulnar nerve ("LOAF" - Lumbricals 1&2, Opponens pollicis, Abductor pollicis brevis, Flexor pollicis brevis superficial head = Median)
GROUP 2: Hypothenar Muscles (4 muscles)
| Muscle | Origin | Insertion | Action | Nerve |
|---|---|---|---|---|
| Abductor digiti minimi | Pisiform | Ulnar base of proximal phalanx of 5th digit + dorsal digital expansion | MCP: flexion + abduction; PIP/DIP: extension | Ulnar (C8, T1) |
| Flexor digiti minimi brevis | Hook of hamate, flexor retinaculum | Base of proximal phalanx of 5th digit | MCP: flexion | Ulnar (C8, T1) |
| Opponens digiti minimi | Hook of hamate, flexor retinaculum | Ulnar border of 5th metacarpal | Draws metacarpal palmarly (opposition) | Ulnar (C8, T1) |
| Palmaris brevis | Ulnar border of palmar aponeurosis | Skin of hypothenar eminence | Tightens palmar aponeurosis (protective) | Ulnar (C8, T1) |
Lumbricals and Interossei (Metacarpal Muscles)
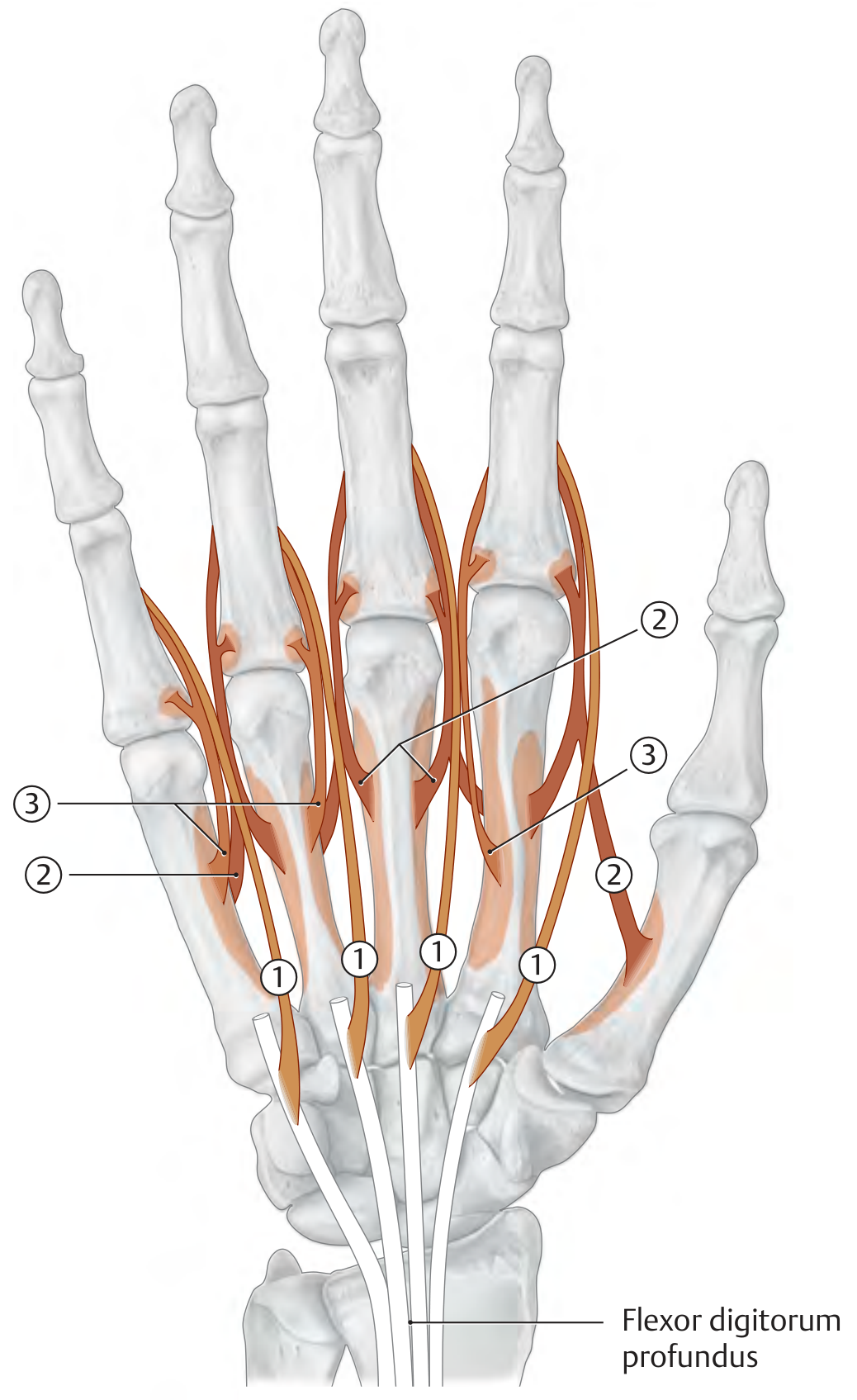
GROUP 3: Lumbricals (4 muscles)
| Muscle | Origin | Insertion | Action | Nerve |
|---|---|---|---|---|
| 1st lumbrical | Radial side of FDP tendon to index finger | Dorsal digital expansion of 2nd digit | MCP flexion; PIP + DIP extension | Median (C8, T1) |
| 2nd lumbrical | Radial side of FDP tendon to middle finger | Dorsal digital expansion of 3rd digit | MCP flexion; PIP + DIP extension | Median (C8, T1) |
| 3rd lumbrical | Adjacent sides of FDP tendons (ring + middle) | Dorsal digital expansion of 4th digit | MCP flexion; PIP + DIP extension | Ulnar (C8, T1) |
| 4th lumbrical | Adjacent sides of FDP tendons (little + ring) | Dorsal digital expansion of 5th digit | MCP flexion; PIP + DIP extension | Ulnar (C8, T1) |
Memory aid: Lateral 2 lumbricals (1st & 2nd) = Median; Medial 2 (3rd & 4th) = Ulnar
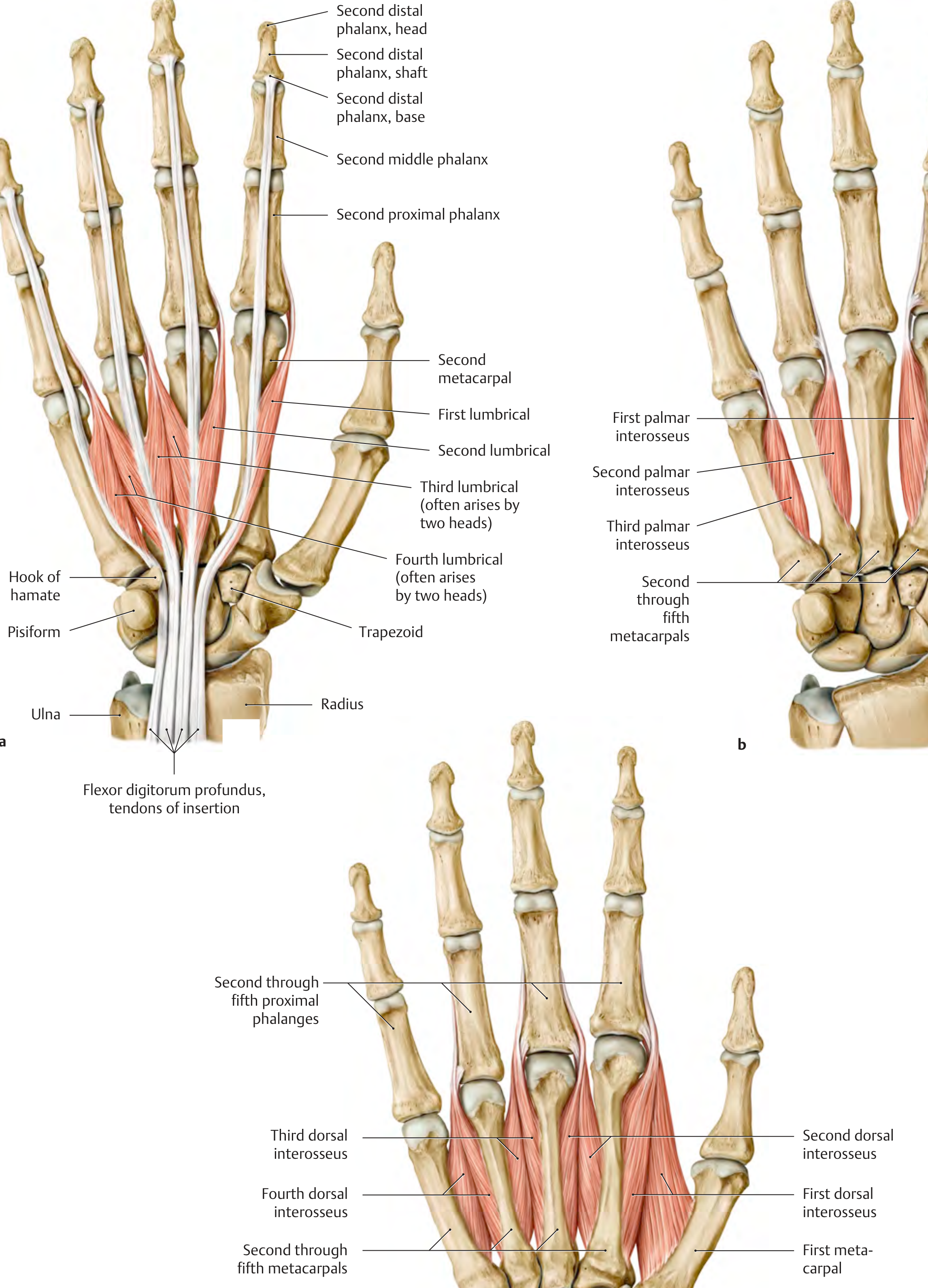
GROUP 4: Interossei
Dorsal Interossei (4 muscles) - "DAB" = Dorsal ABduct
| Muscle | Origin | Insertion | Action | Nerve |
|---|---|---|---|---|
| 1st DI | Adjacent sides of 1st + 2nd metacarpals | Radial side of 2nd proximal phalanx (index) | MCP flexion; PIP/DIP extension; abduction of index | Ulnar (C8, T1) |
| 2nd DI | Adjacent sides of 2nd + 3rd metacarpals | Radial side of 3rd proximal phalanx (middle) | MCP flexion; PIP/DIP extension; abduction of middle | Ulnar (C8, T1) |
| 3rd DI | Adjacent sides of 3rd + 4th metacarpals | Ulnar side of 3rd proximal phalanx (middle) | MCP flexion; PIP/DIP extension; abduction of middle | Ulnar (C8, T1) |
| 4th DI | Adjacent sides of 4th + 5th metacarpals | Ulnar side of 4th proximal phalanx (ring) | MCP flexion; PIP/DIP extension; abduction of ring | Ulnar (C8, T1) |
Palmar Interossei (3 muscles) - "PAD" = Palmar ADduct
| Muscle | Origin | Insertion | Action | Nerve |
|---|---|---|---|---|
| 1st PI | Ulnar side of 2nd metacarpal (index) | Dorsal digital expansion + proximal phalanx of index | MCP flexion; PIP/DIP extension; adduction of index | Ulnar (C8, T1) |
| 2nd PI | Radial side of 4th metacarpal (ring) | Dorsal digital expansion + proximal phalanx of ring | MCP flexion; PIP/DIP extension; adduction of ring | Ulnar (C8, T1) |
| 3rd PI | Radial side of 5th metacarpal (little) | Dorsal digital expansion + proximal phalanx of little | MCP flexion; PIP/DIP extension; adduction of little | Ulnar (C8, T1) |
Note: The thumb and middle finger have no palmar interosseus (middle finger is the reference axis; the thumb has its own adductor pollicis).
Summary: Nerve Supply
| Nerve | Muscles |
|---|---|
| Median nerve (C8, T1) | Abductor pollicis brevis, Opponens pollicis, FPB (superficial head), Lumbricals 1 & 2 → "LOAF" |
| Ulnar nerve (C8, T1) | All other intrinsic muscles: Adductor pollicis, FPB (deep head), all hypothenar muscles, Lumbricals 3 & 4, all interossei |
Summary: Actions of Lumbricals + Interossei Together
Both groups flex at MCP and extend at PIP/DIP - they are responsible for the "writing position" of the fingers and are tested clinically by the intrinsic-plus posture.
Source: THIEME Atlas of Anatomy - General Anatomy and Musculoskeletal System, 9781626237186
This is a shared conversation. Sign in to Orris to start your own chat.