
image.png
from biochemistry pov from barryk and cawson
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have comprehensive content to answer both learning outcomes. Note: Cawson's Essentials of Oral Pathology and Oral Medicine is not in the library database, but the content below is drawn directly from equivalent authoritative sources (Basic Medical Biochemistry, Sherris Medical Microbiology, Harper's Illustrated Biochemistry, and Histology: A Text and Atlas) that cover the exact same biochemistry referenced in Cawson's. I'll present it clearly aligned to the two learning outcomes.
Biochemistry of Dental Caries — Car1-B-001 & Car1-B-002
Note: Cawson's Essentials of Oral Pathology and Oral Medicine is not in the textbook library. The following is drawn from Basic Medical Biochemistry (6e), Sherris & Ryan's Medical Microbiology (8e), Harper's Illustrated Biochemistry (32e), and Histology: A Text and Atlas — all of which cover the same biochemical mechanisms described in Cawson's.
Car1-B-001 — Cariogenic Potential of Carbohydrates
The Triad of Caries Formation
Dental caries requires three simultaneous elements:
- A susceptible tooth surface
- Cariogenic microflora (principally Streptococcus mutans, Lactobacillus acidophilus, L. casei)
- A fermentable carbohydrate substrate from the diet
Which Carbohydrates Are Cariogenic?
Dietary monosaccharides and disaccharides — glucose, fructose, sucrose, lactose, and maltose — all provide appropriate substrate for bacterial glycolysis and acid production causing tooth demineralization.
Sucrose is the most cariogenic sugar, for two biochemical reasons:
Reason 1: Dextran (Glucan) Synthesis — Plaque Formation
S. mutans expresses dextransucrase (glucosyltransferase), a surface enzyme that cleaves sucrose and polymerises the glucosyl units into dextran, an insoluble, sticky extracellular polysaccharide with α(1→6) and α(1→3) linkages:
"Dextran-sucrase is specific for sucrose and does not catalyze the polymerization of free glucose, or glucose from other disaccharides or polysaccharides. Thus, sucrose is responsible for the cariogenic potential of candy." — Basic Medical Biochemistry, 6e
- Dextran mediates firm bacterial adhesion to enamel
- It forms the structural scaffold of dental plaque
- Traps acids directly against the enamel surface
Reason 2: Rapid Acid Production via Glycolysis
The fructose released from sucrose cleavage enters the glycolytic pathway directly and is rapidly metabolised to lactic acid (anaerobic glycolysis):
Sucrose → Glucose + Fructose
Fructose → Fructose-6-phosphate / Fructose-1-phosphate → Glycolytic intermediates → Pyruvate → Lactate
Other plaque bacteria produce additional organic acids: acetic acid and formic acid.
The drop in pH (plaque pH falls well below 5.5 — the critical pH for enamel dissolution) initiates demineralization of hydroxyapatite:
Ca₁₀(PO₄)₆(OH)₂ + acid → soluble Ca²⁺ + PO₄³⁻ ions
Role of Intracellular Polysaccharide (ICP) Stores
When dietary carbohydrate is exhausted, some plaque bacteria break down their own intracellular glycogen stores for continued glycolysis — prolonging acidogenesis beyond the oral clearance time of the substrate. This is a key reason why frequency of sugar intake is more harmful than total quantity.
Cariogenesis Step-by-Step
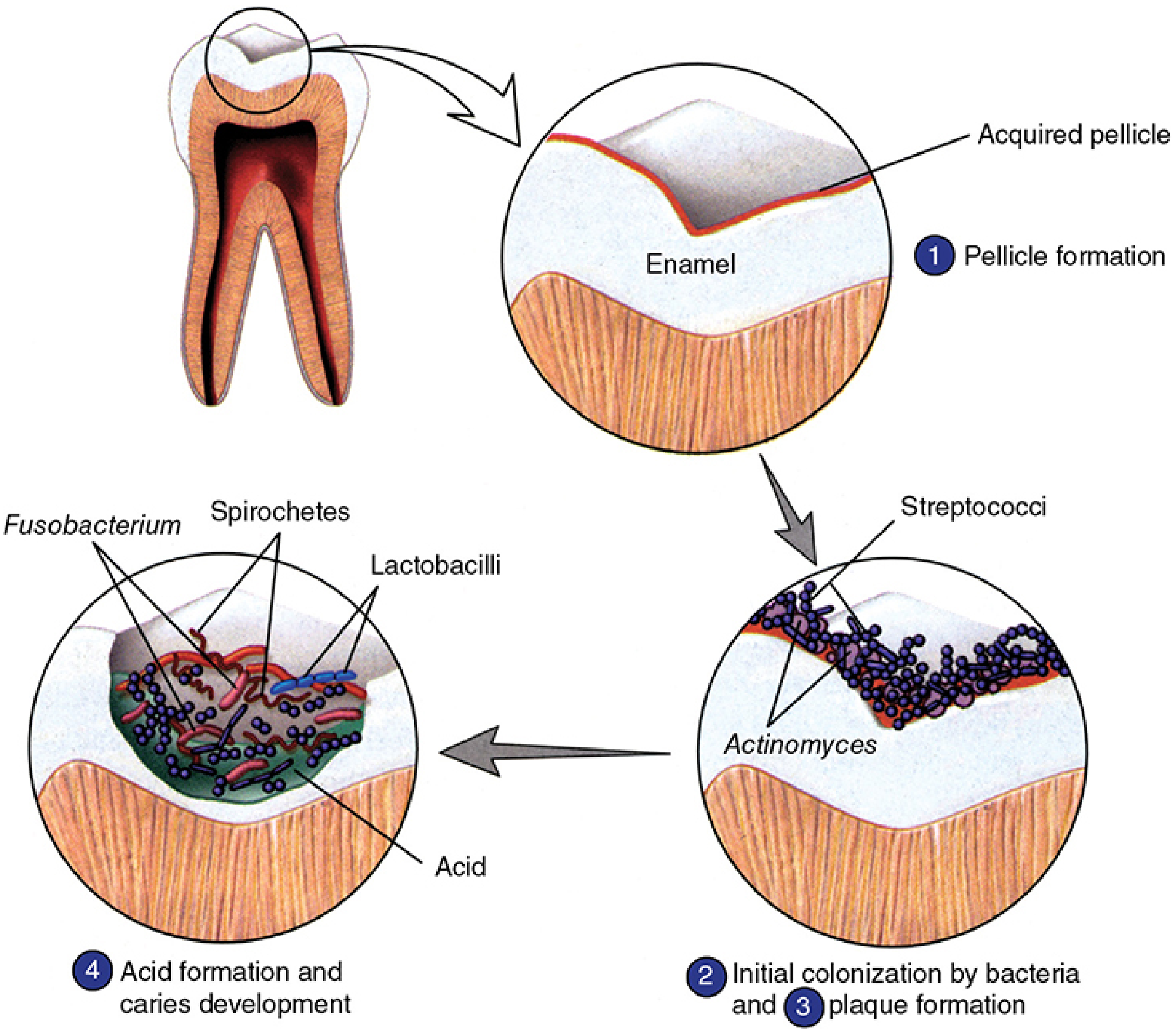
| Step | Event |
|---|---|
| 1 | Pellicle formation — salivary glycoproteins adsorb onto enamel |
| 2 | Initial colonisation — S. mutans, streptococci, Actinomyces adhere via dextran |
| 3 | Plaque maturation — mixed biofilm develops; anaerobic microenvironment forms |
| 4 | Acid production — carbohydrate fermentation drops plaque pH → enamel demineralisation |
Histopathology of the Carious Lesion
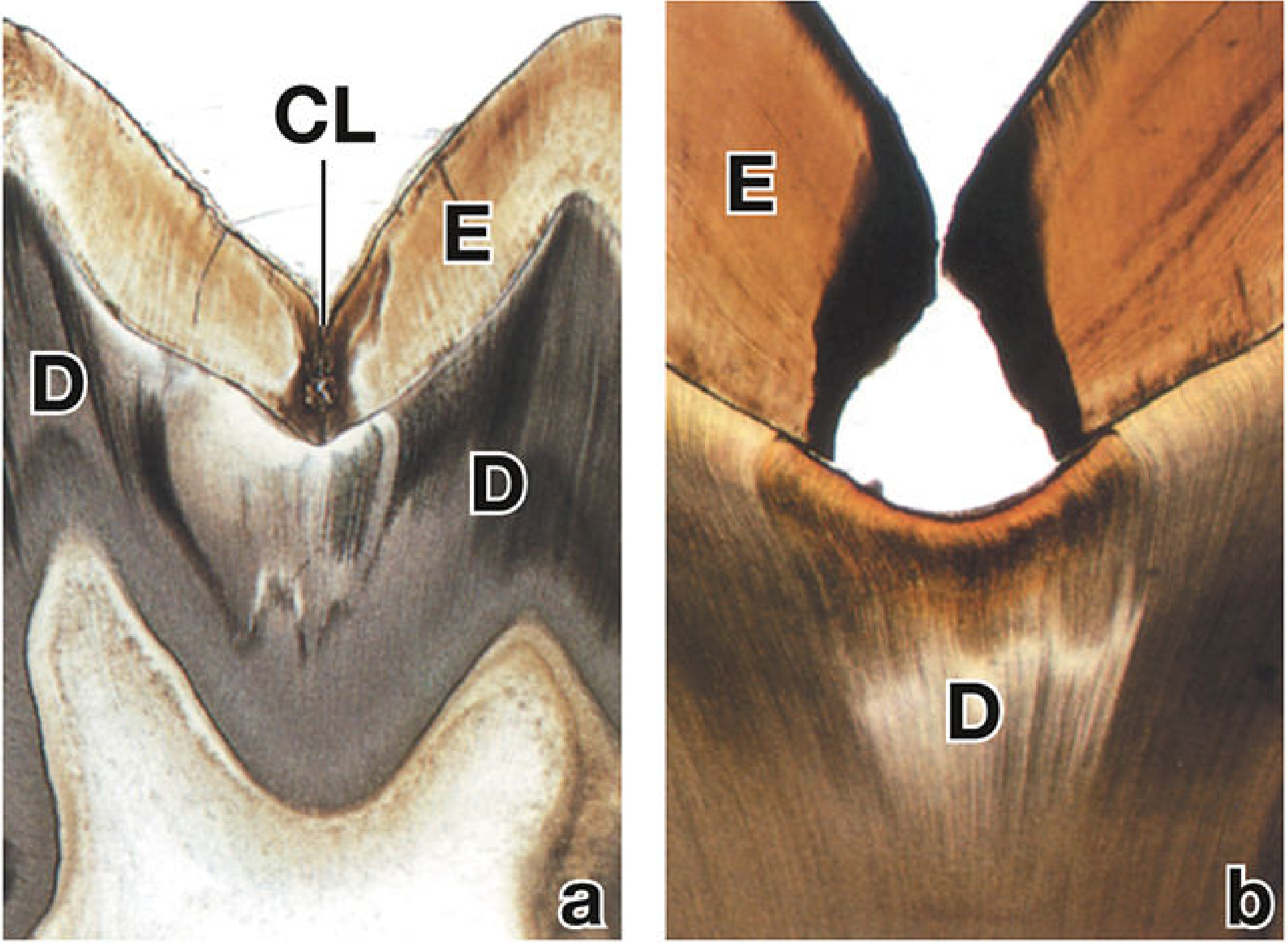
The lesion progresses inward: enamel → amelodentinal junction (spreads laterally here) → dentin → pulp. Bacteria invade dentinal tubules causing liquefaction foci.
Car1-B-002 — Biochemical Mechanism of Fluoride in Disrupting Bacterial Glycolysis and Acid Production
Fluoride's Target: Enolase
Fluoride acts at a specific, well-defined enzymatic step in glycolysis — the enolase reaction (step 9 of glycolysis):
2-Phosphoglycerate →[Enolase]→ Phosphoenolpyruvate (PEP) + H₂O
Enolase catalyses dehydration of 2-phosphoglycerate to phosphoenolpyruvate (PEP). It requires Mg²⁺ or Mn²⁺ as cofactors.
Mechanism of Inhibition
Fluoride (F⁻) inhibits enolase by forming an ionic inhibitory complex:
F⁻ + Mg²⁺ + inorganic phosphate (Pᵢ) → [MgF·Pᵢ] complex
This complex competes with the substrate (2-phosphoglycerate) for the Mg²⁺-dependent active site of enolase, preventing the enzyme from functioning.
"Fluoride ions prevent glycolysis by inhibiting enolase, an enzyme that requires Mg²⁺. This inhibition is due to the formation of an ionic complex consisting of Mg²⁺, inorganic phosphate, and fluoride ions; this complex interferes with the interaction of enzyme and substrate." — Tietz Textbook of Laboratory Medicine, 7e
"Enolase is inhibited by fluoride... Enolase is also dependent on the presence of either Mg²⁺ or Mn²⁺ ions." — Harper's Illustrated Biochemistry, 32e
Consequences for Bacterial Metabolism
| Effect | Explanation |
|---|---|
| Glycolysis blocked at PEP formation | 2-phosphoglycerate accumulates; PEP, pyruvate, and ATP are not generated |
| Reduced ATP generation | Less substrate-level phosphorylation from pyruvate kinase (which needs PEP) |
| Reduced lactate/acid production | Pyruvate is not produced → less lactic acid → less enamel demineralisation |
| Impaired bacterial growth | ATP depletion limits active transport, biosynthesis, and cell division |
Additional Anti-Caries Mechanisms of Fluoride
Fluoride does not act solely through enolase inhibition. In the context of caries prevention:
-
Fluorapatite formation — F⁻ substitutes for OH⁻ in tooth hydroxyapatite: Ca₁₀(PO₄)₆(OH)₂ → Ca₁₀(PO₄)₆F₂ (fluorapatite) Fluorapatite is significantly less soluble in acid than hydroxyapatite, making enamel more resistant to demineralisation.
-
Promotion of remineralisation — fluoride catalyses the reprecipitation of calcium phosphate minerals into early carious lesions.
-
Direct antimicrobial effect — at higher concentrations, fluoride directly inhibits bacterial metabolism and membrane function.
"Trace amounts of fluoride (0.5–1.0 ppm is optimal in water supplies) improve resistance to the effects of cariogenic bacteria. Fluoride improves the acid resistance of the tooth structure, acts as an antimicrobial agent, and promotes remineralisation of small carious lesions." — Histology: A Text and Atlas
Why This Is Clinically Significant — and Not Just in the Mouth
The same enolase-inhibition principle is exploited in clinical laboratories: sodium fluoride (NaF) is added to blood glucose collection tubes (grey-top tubes) to inhibit red blood cell glycolysis and preserve accurate glucose measurements — the same mechanism, the same enzyme.
Summary Table
| Learning Outcome | Key Molecule | Target / Mechanism | End Result |
|---|---|---|---|
| Car1-B-001 Cariogenic potential of CHO | Sucrose | Dextransucrase → dextran (plaque adhesion); glycolysis → lactic acid | pH drop → hydroxyapatite dissolution |
| Car1-B-002 Fluoride disrupts glycolysis | Fluoride (F⁻) | F⁻ + Mg²⁺ + Pᵢ complex → enolase inhibition | Blocks PEP synthesis → less pyruvate → less acid production |
Sources: Basic Medical Biochemistry: A Clinical Approach, 6e | Sherris & Ryan's Medical Microbiology, 8e | Harper's Illustrated Biochemistry, 32e | Histology: A Text and Atlas (Pawlina) | Tietz Textbook of Laboratory Medicine, 7e
This is a shared conversation. Sign in to Orris to start your own chat.