Pink colour sputum
Reading File
Finding Sources
Finding Sources
Searching PubMed
"pulmonary edema" AND "pink frothy sputum"
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Finding Sources
Here is a comprehensive clinical overview of pink/frothy sputum based on authoritative textbooks.
Pink Frothy Sputum
Pink frothy sputum is a mixture of air, alveolar transudate/fluid, and a small amount of blood that has been aerated during breathing. It is a classic sign of alveolar flooding and carries serious clinical significance.
Pathophysiology
Pink frothy sputum forms when elevated pulmonary capillary pressure (or increased capillary permeability) forces fluid - including a small amount of RBCs - into the alveolar spaces. As this fluid is mixed with air during respiration, it becomes frothy. The red blood cells give it the characteristic pink color. It is distinct from frank hemoptysis (bright red blood).
- Harrison's Principles of Internal Medicine 22E explains: "Acute pulmonary edema, due to marked elevation of the pulmonary capillary wedge pressure, is manifested by severe shortness of breath and pink, frothy sputum."
- Fuster and Hurst's The Heart distinguishes it from hemoptysis of mitral stenosis: "This increase is thought to cause rupture of small pulmonary vein anastomoses, leading to frank hemoptysis, to be distinguished from the pink frothy sputum seen in pulmonary edema."
Causes
1. Acute Pulmonary Edema (Most Common)
The classic cause. Due to markedly elevated pulmonary capillary wedge pressure (PCWP), forcing fluid into alveoli.
Underlying etiologies include:
- Acute left ventricular failure (MI, decompensated heart failure)
- Mitral stenosis - pulmonary venous hypertension leads to pink frothy sputum; additionally, sudden rise in left atrial pressure can rupture thin-walled bronchial veins causing "pulmonary apoplexy" - Frameworks for Internal Medicine
- Valvular disease - any lesion causing left-sided failure (tricuspid endocarditis, mitral regurgitation with flail leaflet, aortic stenosis)
- Congestive heart failure - hemoptysis in CHF is nonmassive and described as "pink, frothy" sputum - Frameworks for Internal Medicine
2. High-Altitude Pulmonary Edema (HAPE)
A noncardiogenic pulmonary edema in unacclimatized individuals ascending > 2500 m. Progressive exertional dyspnea evolves to dyspnea at rest, with cough becoming productive of pink frothy sputum. Mechanism: exaggerated hypoxic pulmonary vasoconstriction (HPV) raises pulmonary artery pressure (~60 mmHg), causing stress failure of pulmonary capillaries. - Miller's Anesthesia, 10e
3. Negative Pressure (Postobstructive) Pulmonary Edema (NPPE)
Occurs after laryngospasm or upper airway obstruction following extubation. Forced inspiration against a closed glottis generates extreme negative intrathoracic pressure, which:
- Augments RV preload
- Increases LV afterload, reducing ejection fraction
- Elevates pulmonary hydrostatic pressure
Pink frothy sputum with dyspnea appears within 90 minutes of obstruction. Mortality can reach 40% if treatment is delayed. - Miller's Anesthesia, 10e
4. Immersion/Drowning
Pink frothy sputum can be produced in drowning victims as fluid floods the alveoli. Associated findings include tachypnea, tachycardia, cyanosis, possible arrhythmias, and progression to ARDS. - Goldman-Cecil Medicine
5. Pulmonary Embolism (PE)
Hemoptysis in PE is more likely when there is an associated pulmonary infarction. It can present as pink frothy sputum in some cases but is usually frank blood-streaked sputum. - Frameworks for Internal Medicine
6. Toxic Inhalation (e.g., NO₂)
Nitrogen dioxide and other toxic gases can cause pulmonary edema with frothy sputum production. - Katzung's Basic & Clinical Pharmacology
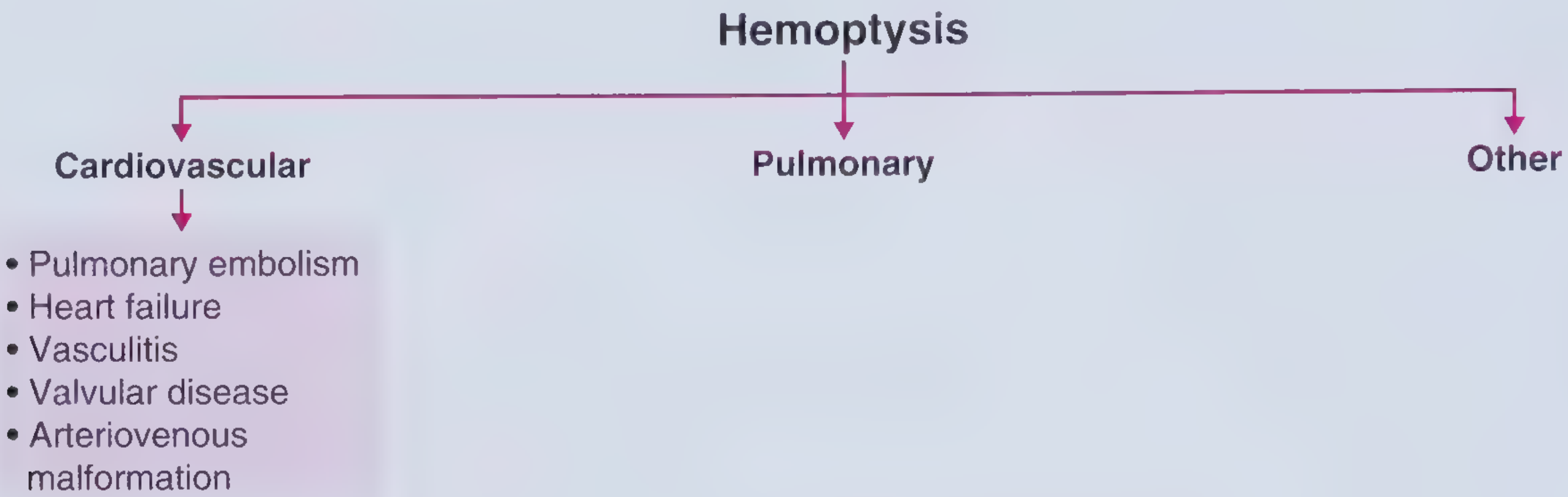
Causes of Hemoptysis - Differential Framework
Clinical Features Accompanying Pink Frothy Sputum
| Feature | Details |
|---|---|
| Dyspnea | Severe, often orthopneic |
| Tachycardia & tachypnea | Almost universal |
| Cyanosis | Indicates significant hypoxemia |
| Bilateral crepitations | Alveolar flooding |
| SpO₂ | Markedly reduced |
| CXR | Bilateral fluffy/patchy alveolar infiltrates ("bat-wing" pattern in cardiogenic edema) |
Management Principles
| Condition | Key Treatment |
|---|---|
| Acute cardiogenic pulmonary edema | Oxygen, IV furosemide (diuresis), nitrates (preload reduction), CPAP/BiPAP, treat underlying cause |
| HAPE | Descent, supplemental O₂, nifedipine (calcium channel blocker to lower PAP), portable hyperbaric chamber |
| NPPE | Supplemental O₂, diuresis, positive pressure ventilation (PPV) in severe cases; resolves in 12-48 hours with treatment |
| Drowning | Basic life support, airway management, CPR if needed; hospitalize all submersion victims for 24-hour monitoring |
Key Clinical Pearls
- Pink frothy sputum = alveolar edema until proven otherwise - treat as a medical emergency
- Distinguish from frank hemoptysis (bright red, not frothy) - different mechanisms and etiologies
- In a mountaineer at altitude with dyspnea + pink frothy sputum = HAPE - immediate descent + oxygen + nifedipine
- Post-extubation pink frothy sputum within 90 minutes = NPPE - support and monitor; mortality 40% if missed
- In mitral stenosis, two hemoptysis mechanisms: (1) pink frothy sputum from pulmonary venous hypertension; (2) massive self-limited bleed from bronchial vein rupture (pulmonary apoplexy)
Sources: Harrison's Principles of Internal Medicine 22E; Frameworks for Internal Medicine; Miller's Anesthesia 10e; Goldman-Cecil Medicine; Fuster and Hurst's The Heart 15e; Barash's Clinical Anesthesia 9e
How to learn the atrial flutter for vegginer with ecg
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Reading File
Reading File
Loading Image
Loading Image
Here is a beginner-friendly guide to Atrial Flutter on ECG, built from authoritative cardiology textbooks with real ECG images.
Atrial Flutter - A Beginner's Guide to ECG
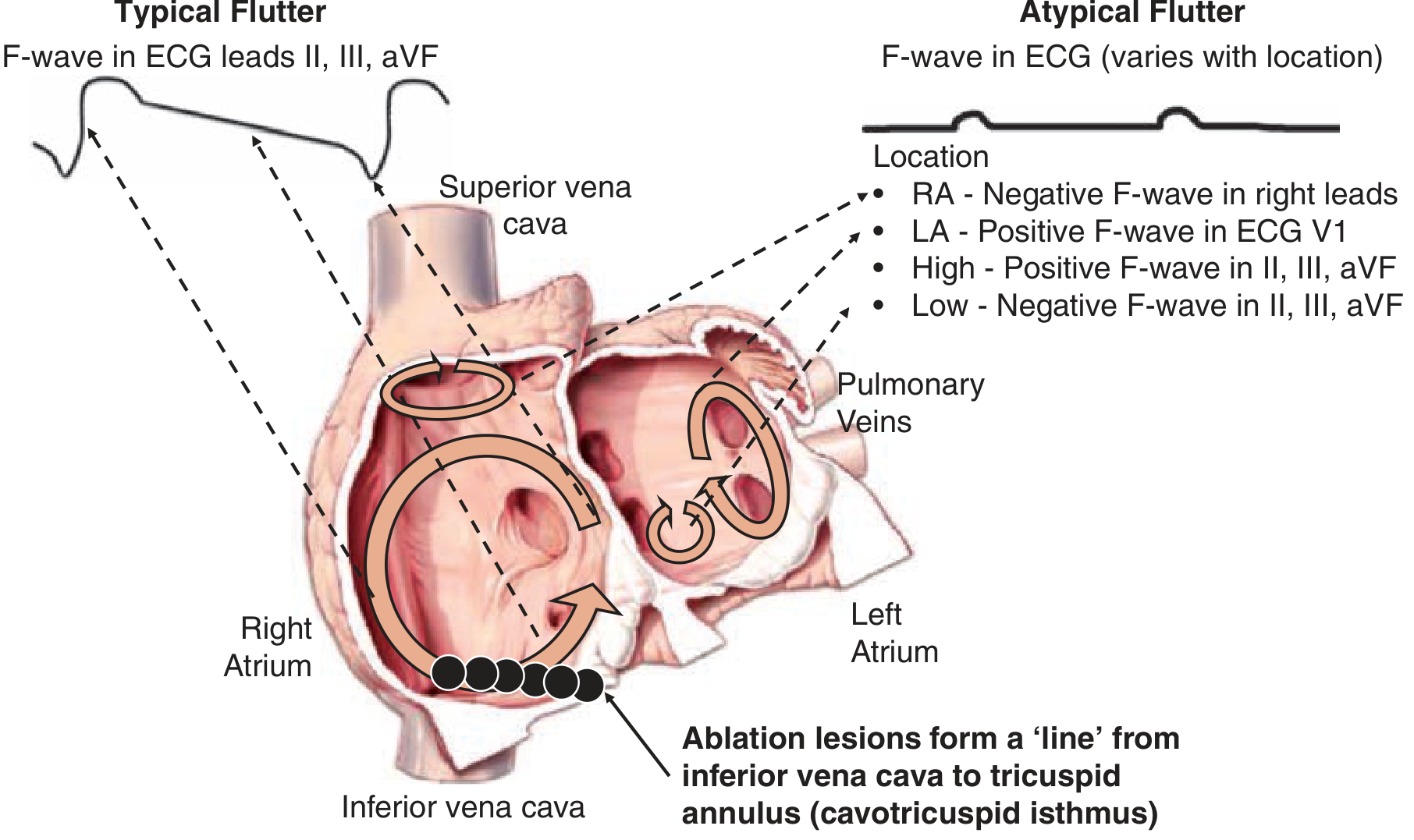
Step 1: Understand What is Happening in the Heart
Think of the normal heart as having an orderly electrical system - one signal fires from the SA node, spreads through the atria, pauses at the AV node, then triggers the ventricles. Everything is neat and organized.
In atrial flutter, the electrical signal gets "trapped" in a loop inside the right atrium. Instead of one clean beat, it keeps going around and around - like a hamster on a wheel - producing rapid, repetitive atrial contractions at ~300 beats per minute.
The reentry circuit loops around the tricuspid valve annulus (the ring around the tricuspid valve), using a narrow bottleneck of tissue called the cavotricuspid isthmus (CTI) at the bottom of the right atrium.
Step 2: The Key Numbers to Remember
| What | Rate |
|---|---|
| Atrial rate (flutter waves) | 250-350 bpm (classically 300 bpm) |
| Ventricular rate (QRS) at 2:1 block | ~150 bpm |
| Ventricular rate at 3:1 block | ~100 bpm |
| Ventricular rate at 4:1 block | ~75 bpm |
Why is the ventricular rate slower? The AV node acts as a gatekeeper and cannot conduct 300 impulses per minute - its refractory period protects the ventricles. So only 1 out of every 2 (or 3 or 4) flutter waves gets through. This is called 2:1, 3:1, or 4:1 conduction block.
Step 3: The Classic ECG Pattern - "Sawtooth"
This is the most important feature to recognize.
Look at leads II, III, and aVF first (the inferior leads)
Typical (counterclockwise) atrial flutter:
- Flutter waves are NEGATIVE (pointing down) in leads II, III, aVF - like a sawtooth
- Flutter waves are POSITIVE (pointing up) in lead V1
Here is the classic 12-lead ECG of typical atrial flutter with 2:1 block:
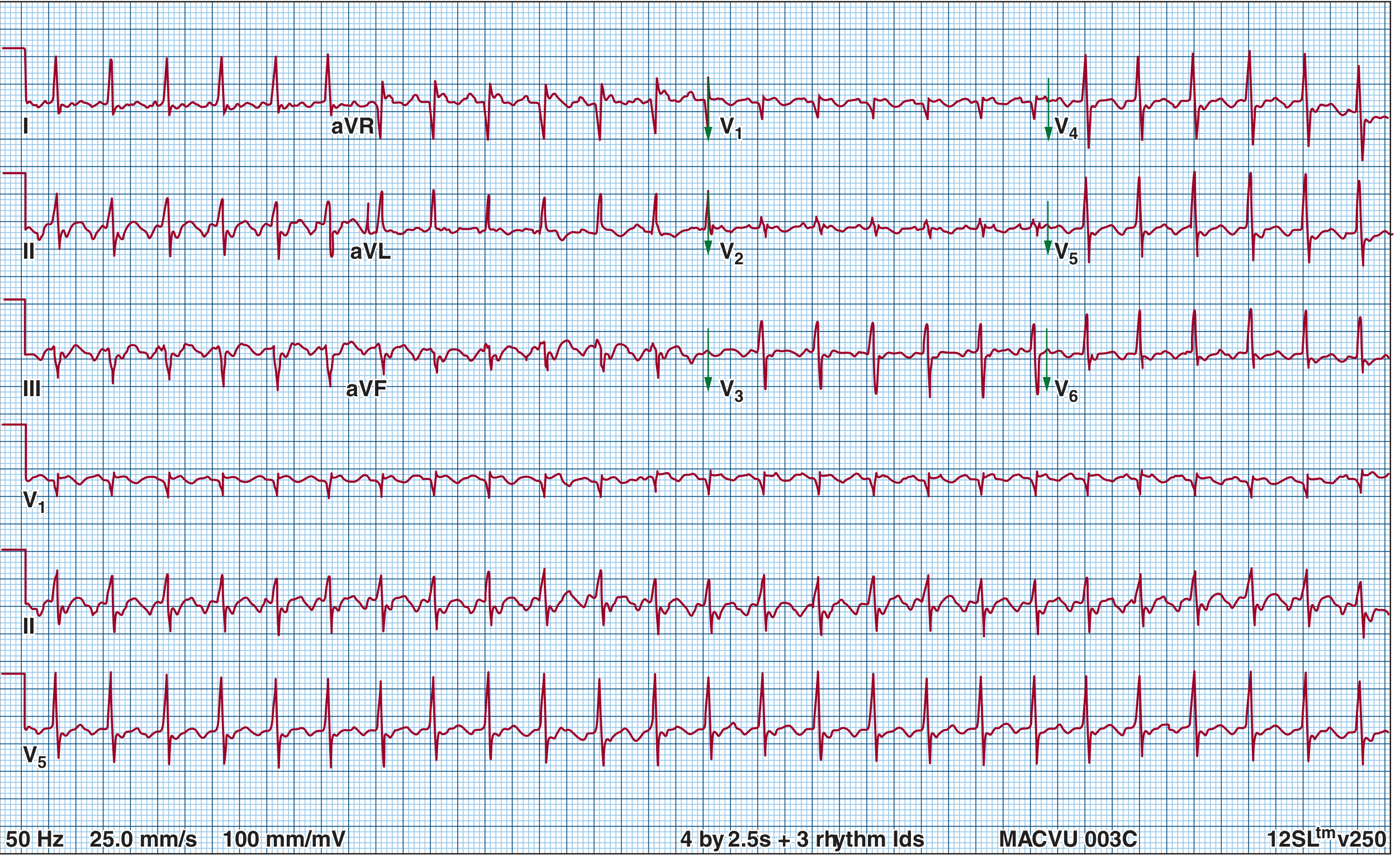
Notice the regular sawtooth "F waves" - there are 2 flutter waves for every QRS complex (2:1 block), giving a ventricular rate of ~150 bpm.
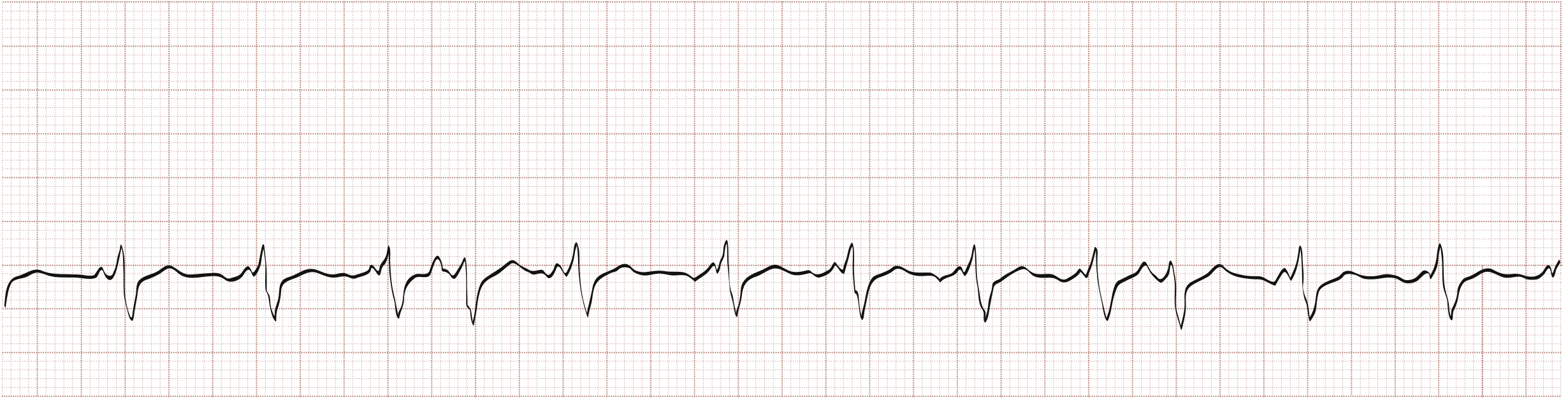
Step 4: The Simple ECG Tracing (Lead II)
Here is a simple, clean tracing showing the sawtooth pattern clearly:
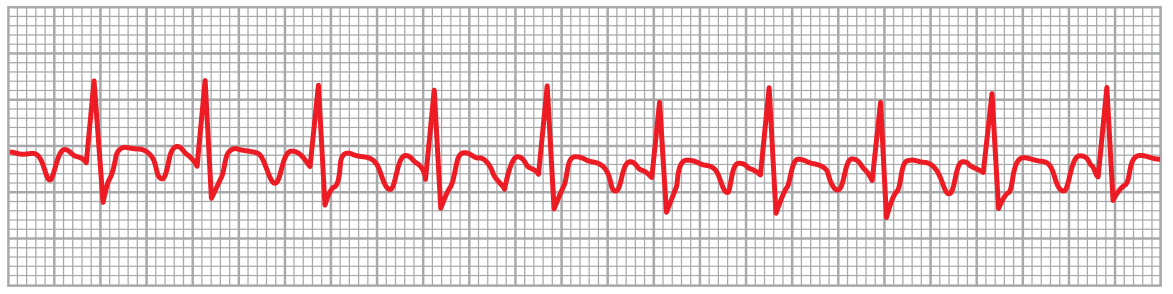
- The repetitive up-down pattern between QRS complexes = flutter (F) waves
- There is no flat baseline (isoelectric line) between waves - the sawtooth is continuous
- One QRS follows every 2 flutter waves = 2:1 block
Step 5: The 5-Step Method to Read Atrial Flutter ECG
Follow this checklist when you see a fast, regular rhythm:
1. Is the rhythm regular?
- Atrial flutter with fixed block (2:1, 3:1) = regular
- Variable block = slightly irregular
- (Compare: atrial fibrillation is irregularly irregular)
2. Count the ventricular rate (QRS rate)
- If ~150 bpm in an untreated patient → think 2:1 atrial flutter immediately
3. Look between the QRS complexes
- Do you see a sawtooth/zigzag pattern without any flat baseline?
- Count the "teeth" between two QRS complexes → if 2 teeth = 2:1 flutter
4. Check the inferior leads (II, III, aVF)
- Negative (downward) sawtooth = typical counterclockwise flutter
- Positive (upward) flutter waves = clockwise (reverse) flutter
5. Check lead V1
- Typical flutter: upright (positive) P/F waves in V1
Step 6: What if Flutter Waves are Hidden?
At 2:1 conduction, flutter waves can be buried inside the QRS or T wave and hard to see. To unmask them:
- Perform carotid sinus massage (vagal maneuver) - slows AV conduction temporarily
- Give IV adenosine - transiently blocks AV node, revealing flutter waves clearly
- Both work by increasing the AV block so more flutter waves become visible on the ECG
Step 7: Atrial Flutter vs Atrial Fibrillation - Spot the Difference
| Feature | Atrial Flutter | Atrial Fibrillation |
|---|---|---|
| Atrial rate | 250-350 bpm (organized) | 350-600 bpm (chaotic) |
| Rhythm | Regular (or regularly irregular) | Irregularly irregular |
| P waves | Sawtooth flutter waves (F waves) | No distinct P waves (fibrillatory baseline) |
| Baseline | Continuous sawtooth, no flat line | Undulating, irregular |
| AV conduction | Fixed ratio (2:1, 3:1, 4:1) | Variable |
Step 8: Why Does Atrial Flutter Happen? (Causes)
- Valvular heart disease (esp. mitral/tricuspid)
- Coronary artery disease / heart failure
- Post-cardiac surgery
- Thyrotoxicosis / acute alcohol exposure
- Acute pulmonary embolism
- Congenital heart disease
- Electrolyte abnormalities
Step 9: Basic Treatment Concepts
| Goal | Methods |
|---|---|
| Rate control | AV nodal blockers (beta-blockers, diltiazem) - but harder to control than AF |
| Rhythm control | Electrical cardioversion (low energy, easy), ibutilide, dofetilide, amiodarone |
| Prevent stroke | Anticoagulation (same risk as AF - use CHA₂DS₂-VASc score) |
| Cure (definitive) | Catheter ablation of cavotricuspid isthmus - >95% success rate, first-line therapy |
Memory Aid
"Flutter = 300, Sawtooth, II/III/aVF negative, 2:1 block = 150"
Think of the letter F for Flutter:
- F waves (flutter waves)
- Fast atria (~300 bpm)
- Filtered by AV node (2:1 block)
- Fixed regular rhythm
Sources: Guyton & Hall Medical Physiology; Fuster & Hurst's The Heart 15e; Harrison's Principles of Internal Medicine 22E; Goldman-Cecil Medicine
Atrial tacgycardia
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Loading Image
Reading File
Finding Sources
Loading Image
Reading File
Loading Image
Here is a complete beginner's guide to Atrial Tachycardia (AT) with ECG images from authoritative cardiology textbooks.
Atrial Tachycardia - A Beginner's Guide
What is Atrial Tachycardia?
Atrial tachycardia (AT) is a fast atrial rhythm (>100 bpm) that arises from a site outside the sinus node - from an ectopic (abnormal) focus somewhere in the atrial muscle or the great cardiac veins.
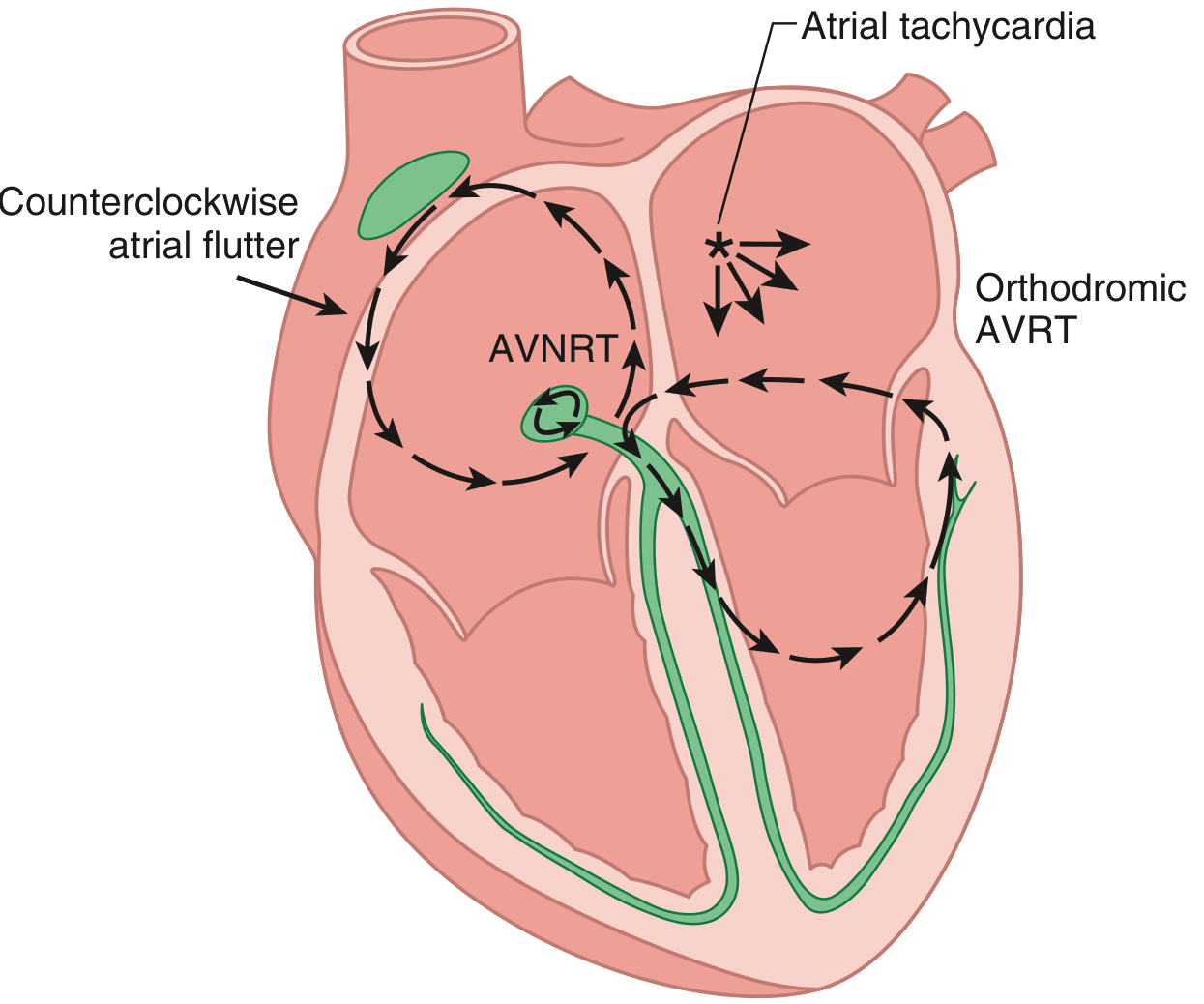
Unlike atrial flutter (a big reentry loop) or AF (chaotic activity), AT comes from a single small spot firing rapidly and spreading outward like ripples in a pond.
This concept is shown clearly here:
Key Numbers
| Feature | Value |
|---|---|
| Heart rate | 100-250 bpm (rarely exceeds 200 bpm) |
| Rhythm | Usually regular |
| P waves | Present, but abnormal shape (different from sinus P waves) |
| PR interval | Usually normal or slightly prolonged |
| QRS | Narrow (normal - the ventricles activate normally) |
The 3 Mechanisms That Cause AT
| Mechanism | What Happens |
|---|---|
| Enhanced automaticity | An ectopic atrial cell fires faster than the sinus node and takes over |
| Triggered activity | Afterdepolarizations (small voltage oscillations) trigger extra beats - common in digoxin toxicity |
| Reentry | A small reentry loop within a patch of atrial tissue (micro-reentry) |
Where Does AT Come From? (Anatomic Origins)
AT arises from predictable locations in the atria:
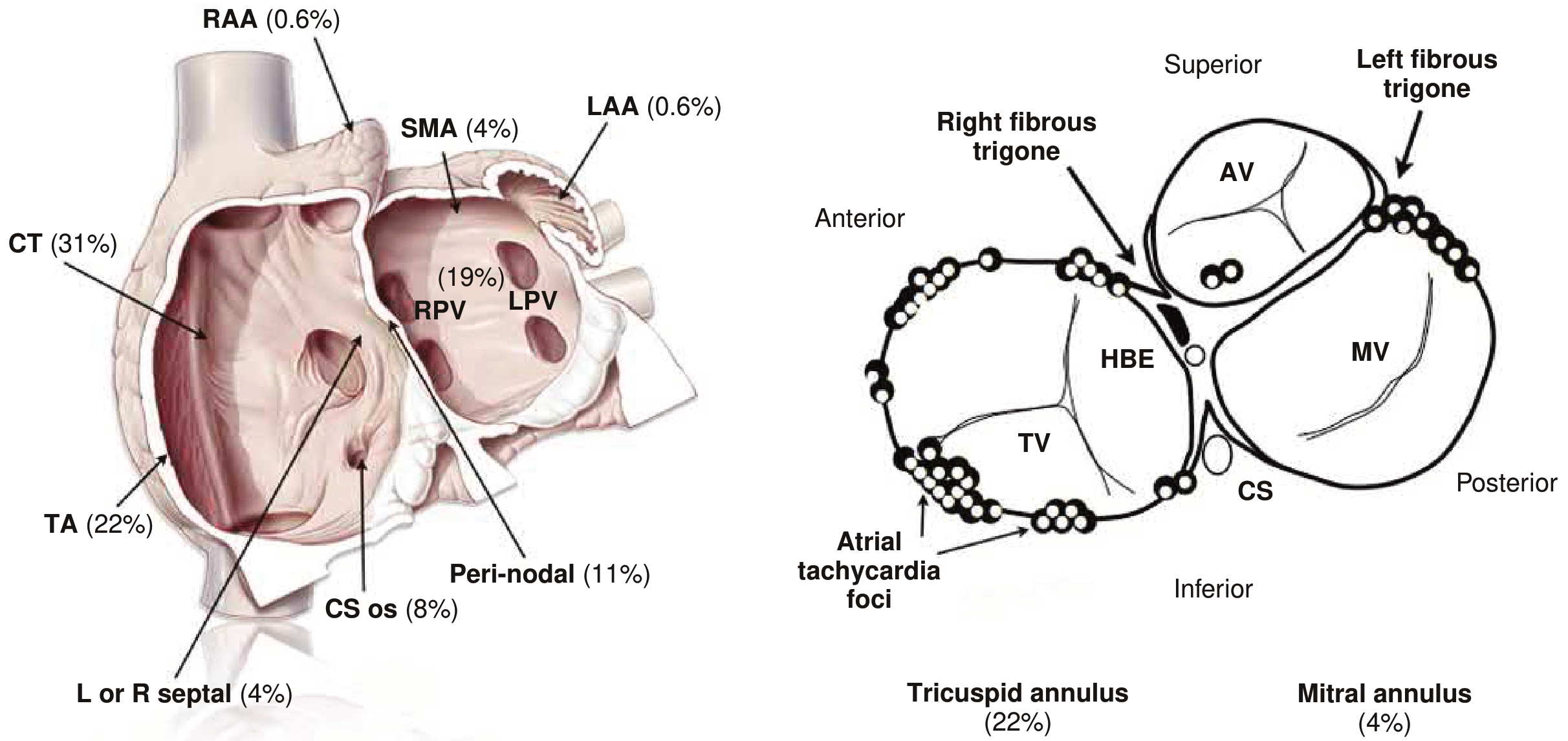
Right atrium (~75% of ATs):
- Crista terminalis (CT) - 31% - most common!
- Tricuspid annulus (TA) - 22%
- Peri-nodal region - 11%
- Coronary sinus ostium - 8%
Left atrium (~25%):
- Pulmonary vein ostia - 19%
- Superior mitral annulus - 4%
ECG Features - Step by Step
The #1 Rule: Find the P wave first
In AT, every QRS is preceded by a P wave - but that P wave looks different from your normal sinus P wave.
Normal sinus P wave: upright and rounded in leads I and II, upright in aVF
AT P wave: shape depends on where the focus is - can be inverted, biphasic, flat, or pointed
Classic ECG of Focal Atrial Tachycardia
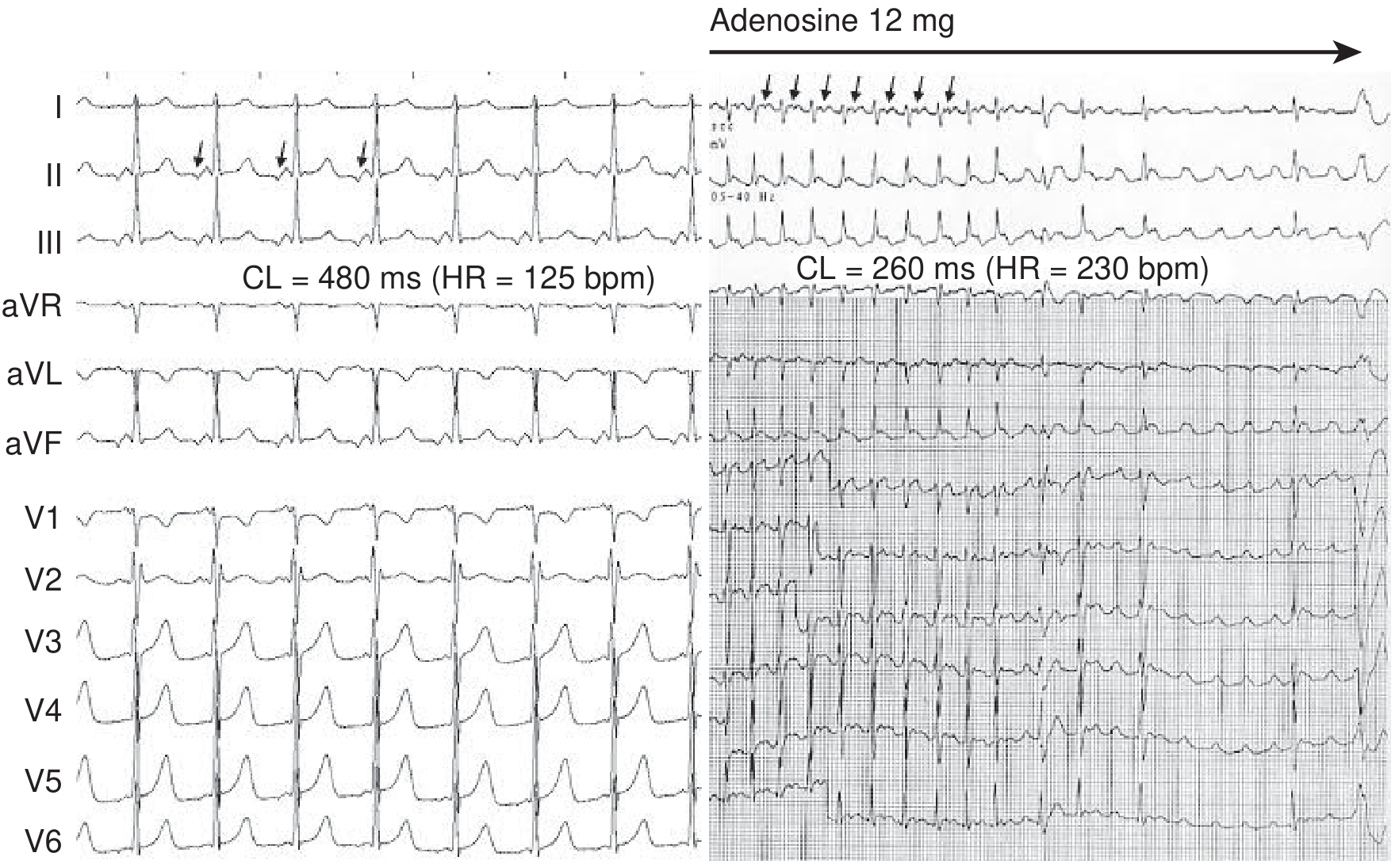
- Left panel (125 bpm): P waves clearly visible before each QRS. Note the P wave in lead II is biphasic (negative-positive) - not a normal sinus P wave. There is a clear isoelectric (flat) baseline between P waves.
- Right panel (230 bpm, given adenosine): The AV node is blocked by adenosine - QRS complexes disappear - but the P waves keep firing independently. This proves the tachycardia is in the atrium, not the AV node.
This is the key teaching point: Adenosine blocks AV conduction but does NOT stop AT - the atrial rhythm continues. This helps distinguish AT from AVNRT/AVRT where adenosine usually terminates the arrhythmia.
ECG of AT with 2:1 Block (Digoxin Toxicity)
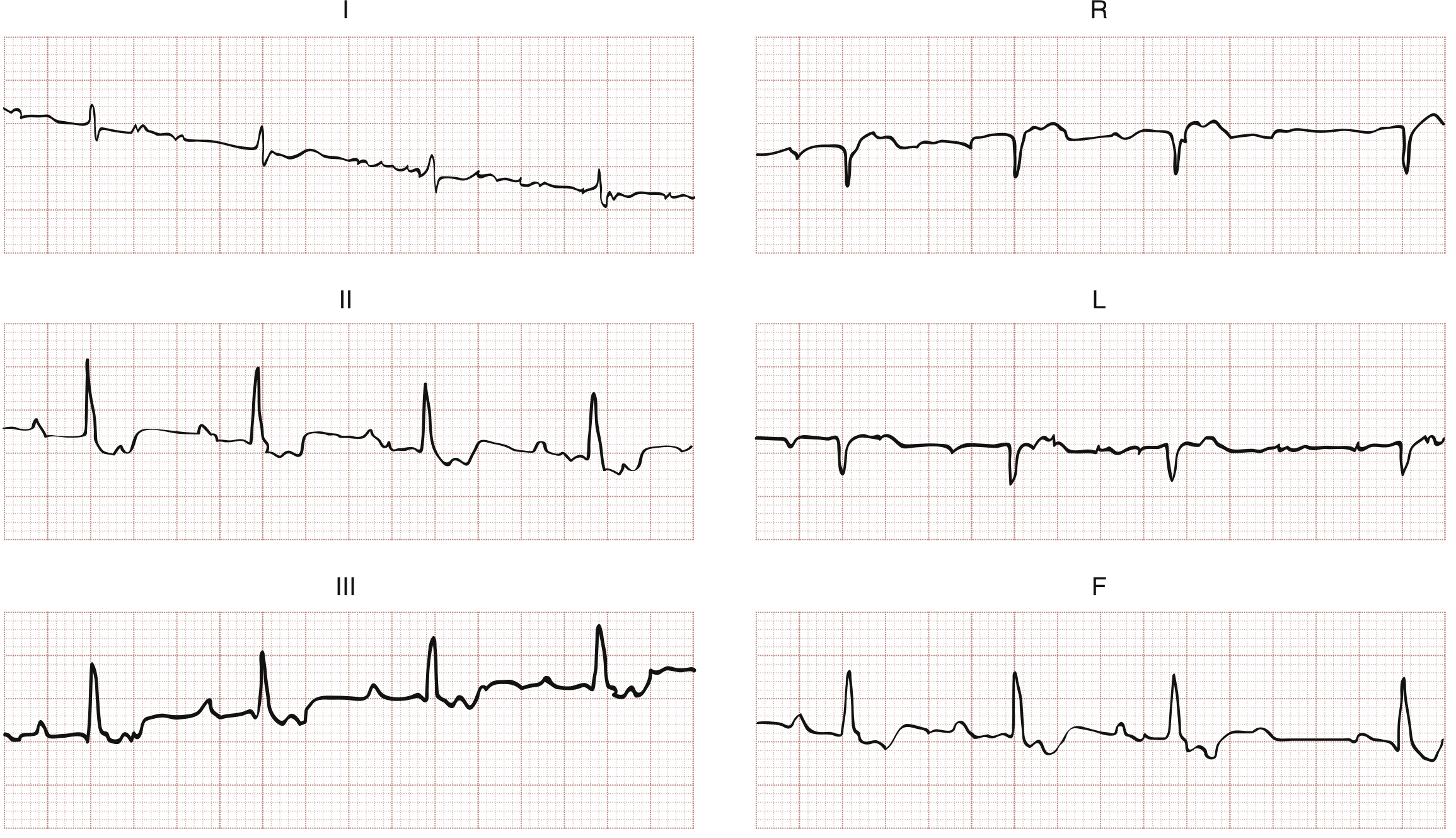
When AT is fast or when AV conduction is impaired (e.g., digoxin toxicity), the AV node cannot conduct every P wave - giving a 2:1 pattern (2 P waves for every 1 QRS). This can look similar to atrial flutter but the rate is slower and P waves have a different shape.
How to Read the P Wave - Localizing the Focus
The shape of the P wave tells you WHERE in the atrium the focus is:
| P wave in V1 | Likely origin |
|---|---|
| Upright (positive) in V1 | Left atrium |
| Negative (inverted) in V1 | Right atrium |
| Negative in II, III, aVF | Focus is low in the atrium or in the coronary sinus |
| Positive in II, III, aVF | Focus is high (near the top of the atrium) |
Special Type: Multifocal Atrial Tachycardia (MAT)
MAT = AT with 3 or more different P wave morphologies in the same lead, with varying PR and P-P intervals. Each beat comes from a different atrial location.
Key facts about MAT:
- Rate > 100 bpm with at least 3 different P wave shapes
- Irregular rhythm (often confused with atrial fibrillation!)
- Strongly associated with COPD (up to 60% of cases) and severe pulmonary disease
- Treatment: treat the underlying lung disease first; IV diltiazem, verapamil, or metoprolol if needed
AT vs Other SVTs - Quick Comparison
| Feature | Atrial Tachycardia | AVNRT | Atrial Flutter | Sinus Tachycardia |
|---|---|---|---|---|
| Rate | 100-250 bpm | 150-250 bpm | ~300 bpm atrial / 150 ventricular | 100-180 bpm |
| P wave | Abnormal shape, before QRS | Retrograde (buried in QRS or just after) | Sawtooth F waves | Normal upright P |
| Baseline | Isoelectric between P waves | No visible P or retrograde P | Continuous sawtooth, no baseline | Flat baseline |
| Adenosine | Continues (AV block only) | Terminates | Unmasks flutter waves | Slows then returns |
| Regularity | Regular | Regular | Regular | Regular |
Causes / Risk Factors
- Children and young adults with structural heart disease (congenital)
- Digoxin toxicity (AT with 2:1 block = digoxin toxicity until proven otherwise)
- Hypoxemia (e.g., COPD, PE)
- Electrolyte disturbances (hypokalemia, hypomagnesemia)
- Metabolic disturbances
- Prior cardiac surgery (scarring creates reentry substrate)
- Cardiomyopathy, valvular disease
- Incessant AT → tachycardia-induced cardiomyopathy (reversible after ablation!)
Warm-Up and Cool-Down - A Hallmark of AT
- AT from enhanced automaticity has a characteristic:
- Warm-up: rate gradually accelerates at the start over a few beats
- Cool-down: rate gradually slows before terminating
- Reentrant AT starts and stops abruptly
Treatment
| Setting | Approach |
|---|---|
| Acute (unstable) | DC cardioversion |
| Acute (stable) | IV adenosine (diagnostic + may terminate), IV beta-blocker or calcium channel blocker (diltiazem/verapamil) |
| Precipitating factor | Treat hypoxia, correct electrolytes, stop digoxin if toxic |
| Chronic/recurrent | Oral beta-blockers or calcium channel blockers |
| Definitive cure | Catheter ablation - first-line for symptomatic or incessant AT (>95% success for many locations) |
| MAT | Treat underlying pulmonary disease; cardioversion rarely works long-term |
Important: Incessant AT causing a persistently rapid ventricular rate can lead to tachycardia-induced cardiomyopathy (dilated cardiomyopathy from rate alone). This is fully reversible after successful ablation or rate control.
Memory Aid
"AT = Abnormal P, Atrial focus, Adenosine won't stop it"
- A = Abnormal P wave shape
- T = Tachycardia from ectopic atrial focus
- Adenosine = exposes P waves but does NOT terminate AT
- Warm-up/cool-down = automaticity mechanism
Sources: Braunwald's Heart Disease 12e; Rosen's Emergency Medicine; Goldman-Cecil Medicine; Fuster & Hurst's The Heart 15e; Guyton & Hall Medical Physiology
This is a shared conversation. Sign in to Orris to start your own chat.