Kindly provide detailed theory of 1. Types of incision used in Tympanomastoid surgery with photo 2. Types of endoscopic Tympanomastoid surgery
Reading File
Finding Sources
Finding Sources
Searching the Web
tympanomastoid surgery incisions types postauricular endaural endoscopic
Finding Sources
Finding Sources
Reading Web Page
https://entokey.com/incisions-and-approaches
Finding Sources
Finding Sources
Searching the Web
types endoscopic tympanomastoid surgery TEES endoscopic ear surgery classification 2024
Finding Sources
Loading Image
Loading Image
Reading File
Reading Web Page
https://pmc.ncbi.nlm.nih.gov/articles/PMC11546356
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
Searching the Web
postauricular incision ear surgery photo diagram mastoidectomy approach
Loading Image
Loading Image
Reading Web Page
https://otosurgeryatlas.stanford.edu/otologic-surgery-atlas/…
I now have comprehensive material from the Stanford Oto Surgery Atlas (Jackler/Gralapp), the Entokey textbook reference, and the PMC review on endoscopic ear surgery. Let me compile the full detailed answer.
Tympanomastoid Surgery: Incisions and Endoscopic Approaches
PART 1 - Types of Incisions Used in Tympanomastoid Surgery
The three principal incisions for tympanomastoid surgery are the transcanal, the endaural, and the postauricular (with its modifications). Each offers a different balance of exposure, scar visibility, and donor-site access for grafts.
1. Transcanal (Meatal) Incision
Definition: All surgery is performed entirely through the external auditory canal (EAC), without any external skin incision.
Anatomy of the incision: A tympanomeatal flap is raised inside the EAC. The classic incision is a posteriorly based U-shaped (or anteriorly based) cut in the canal skin, typically starting at the 6 o'clock and 12 o'clock positions, approximately 5-6 mm lateral to the tympanic annulus.
Technique:
- The patient's head is turned away
- Incisions are placed in the posterior and/or inferior canal skin
- The meatal flap is elevated medially to expose the tympanic membrane and posterior tympanicum
- No skin incision is made outside the ear
Access provided: Tympanic membrane and posterior tympanicum only. The anterior TM is often partially hidden by an anterior canal bulge.
Indications:
- Tympanoplasty for posterior perforations
- Stapedectomy (anteriorly based tympanomeatal flap)
- Ventilating tube insertion
- Ossiculoplasty for posterior/inferior ossicular pathology
- Excision of small glomus tympanicum tumors visible at otoscopy
- Myringotomy
Limitations: Cannot access the mastoid. Limited access to anterior TM, epitympanum, or large glomus tumors extending anteriorly/inferiorly.
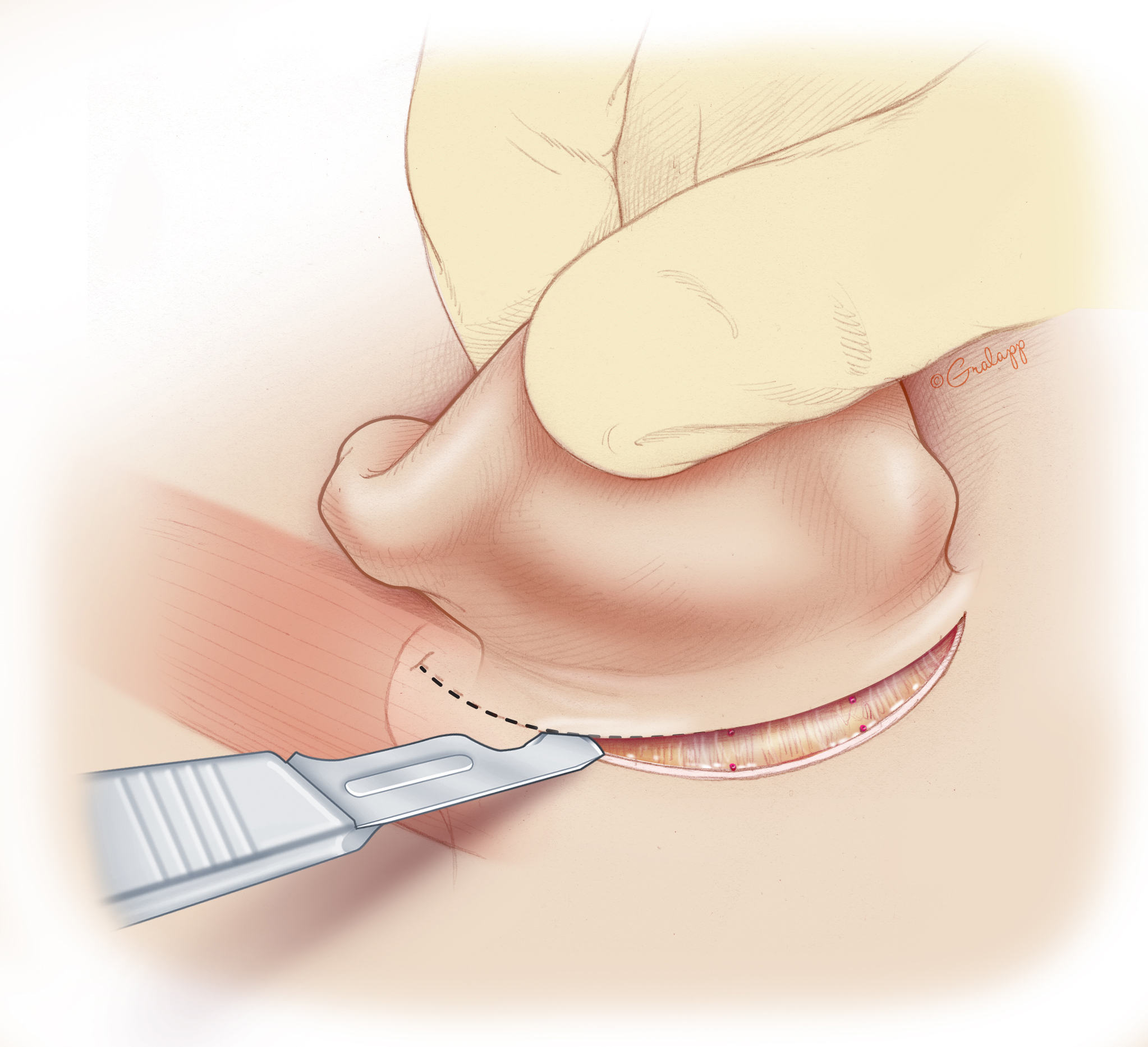
2. Endaural Incision
Definition: An incision that uses the natural opening of the EAC, extended superiorly between the helical crus and tragus (the intercartilaginous notch) to reach the temporal region.
Three segments of the endaural incision:
- Circumferential (canal) segment - runs circumferentially inside the canal
- Intercartilaginous segment - passes between the helical crus and the tragus (the "Lempert notch")
- Vertical (temporal) limb - extends superiorly toward the temporal region

Technique:
- The circumferential incision is carried at the bony-cartilaginous junction of the EAC
- The incision is extended superiorly through the intercartilaginous cleft between the helical crus and tragus
- The vertical limb extends up to expose temporalis fascia
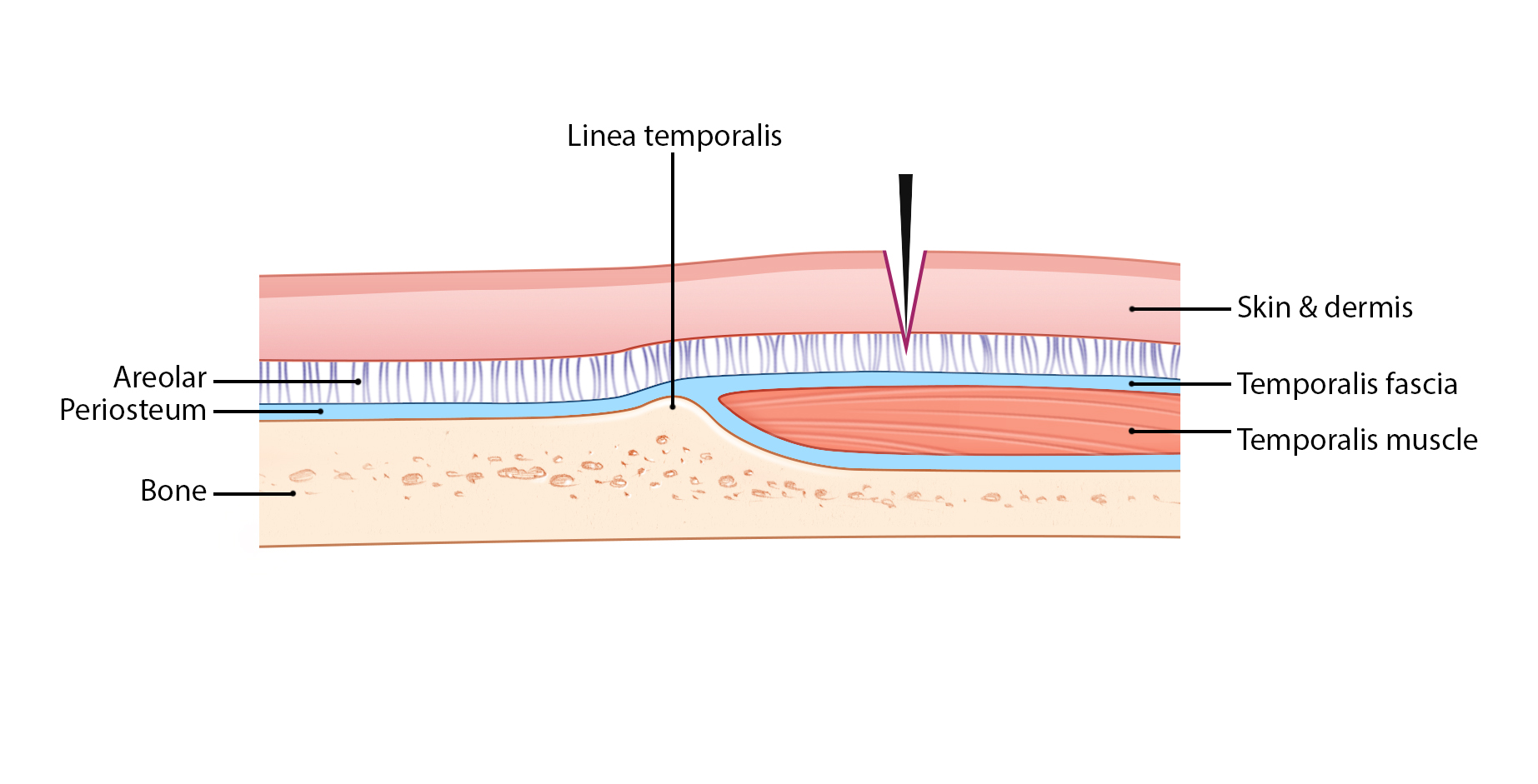
- Needle-point electrocautery is used through the dermis to reach the temporalis fascia superiorly
- The temporalis muscle is elevated off the linea temporalis
- This gives access to the superior canal, epitympanum, and (with the Heermann extension) the mastoid
Access provided: EAC, tympanic membrane, epitympanum, anterior canal, and mastoid (with Heermann extension).
Indications:
- Canalplasty (for exostoses, stenosis)
- Tympanoplasty - especially for anterior perforations and total drum replacement
- Anterior atticotomy
- When the postauricular approach risks collapsing the ear canal (the auricle migrates anteriorly with postauricular incisions)
- Procedures in an abnormally narrow meatus
- As an alternative to postauricular incision for limited mastoidectomy
Advantages:
- Scar is hidden within the conchal bowl / intercartilaginous area (cosmetically superior to postauricular in some patients)
- No risk of anterior ear canal collapse postoperatively
- Good access to the anterior EAC and epitympanum
- Temporalis fascia graft is readily accessible
Disadvantages:
- Visible scar in the concha in some patients
- Limited posterior exposure compared to the postauricular approach
- Not ideal when wide mastoidectomy is anticipated
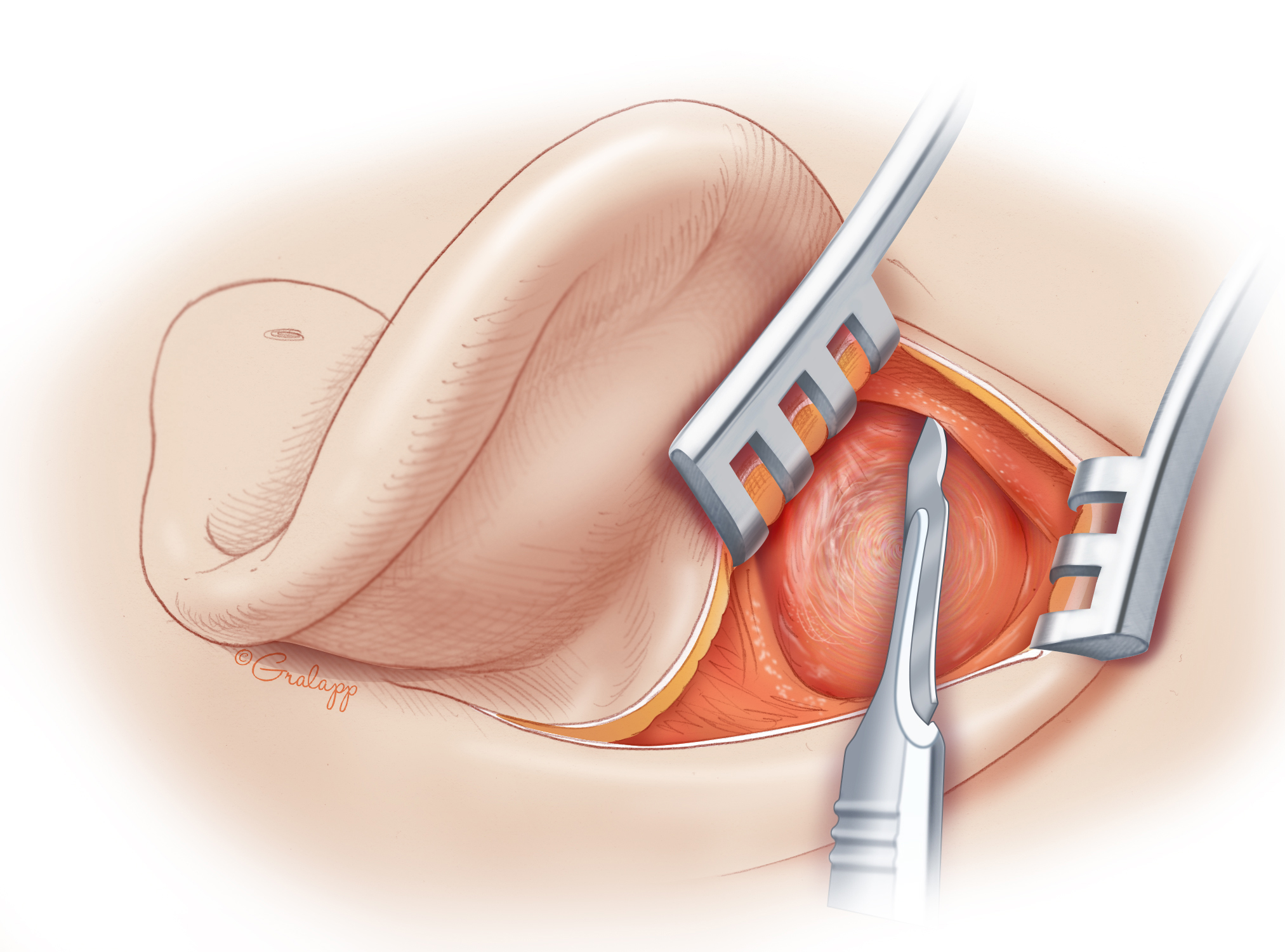
3. Postauricular (Retroauricular) Incision
Definition: A vertical incision placed in the postauricular sulcus (or 5-10 mm posterior to it), curving from the helical root superiorly to the mastoid tip inferiorly.
Technique:
- The pinna tilts ~15 degrees posteriorly relative to the axis of the malleus/TM
- The incision is made 5-10 mm behind the postauricular sulcus (heal better, less retraction than sulcus incisions)
- The superior limb is carried forward to allow the ear to rotate anteriorly for full middle ear access
- Inferiorly, the incision is carried to the mastoid tip (in infants, take care - no developed mastoid tip, facial nerve at risk)
- Skin and subcutaneous tissue are incised through to periosteum
- The linea temporalis is identified - the bony ridge forming the inferior margin of the temporalis muscle fossa (a key surgical landmark)
- Electrocautery opens the periosteum along the linea temporalis, extending forward to the anterior aspect of the EAC so soft tissues rotate forward
- A periosteal elevator (e.g., Lempert) exposes the mastoid cortex
- The SCM insertion is dissected off the mastoid tip
- Two retractors are placed: one spanning ear canal to sinodural angle, one lifting temporalis muscle
Access provided: TM, entire tympanomastoid compartment, hypotympanum.
Indications:
- Tympanoplasty (all types, especially anterior perforations requiring wider access)
- Tympanomastoidectomy (canal wall up or down)
- Hypotympanotomy
- Cochlear implantation (modified postauricular)
- Ossiculoplasty
- Facial nerve decompression
- Access to mastoid for revision surgery
Advantages:
- Widest exposure of the tympanomastoid compartment
- Excellent access for temporalis fascia harvest through the same incision
- Standard approach for all mastoid surgery
Disadvantages:
- Scar behind the ear (usually well-hidden)
- Risk of anterior migration of the auricle postoperatively (can cause ear canal collapse)
- Greater tissue dissection than endaural or transcanal approaches
3a. Modified Postauricular Incision
Extended superiorly into the temporal region (more than the standard postauricular curve). Used for cochlear implantation and procedures requiring access to the temporal fossa (e.g., middle fossa approach entry point).
3b. Extended Postauricular Incision
The incision extends superiorly toward the temporal region AND inferiorly into the neck. Provides access to:
- Tympanomastoid compartment
- Upper neck structures
- Infratemporal fossa
Indicated for: infratemporal fossa tumors, jugular paragangliomas, and petrous apex lesions requiring combined cervico-mastoid access.
Summary Table of Incisions
| Incision | Access | Typical Procedures |
|---|---|---|
| Transcanal tympanomeatal | TM, posterior tympanicum | Tympanoplasty (posterior perf), stapedectomy, VT, small glomus |
| Endaural | EAC, TM, epitympanum | Canalplasty, ant. tympanoplasty, atticotomy, limited mastoidectomy |
| Postauricular | TM, tympanomastoid compartment | Tympanomastoidectomy, all mastoid surgery, hypotympanotomy |
| Modified postauricular | Tympanomastoid + temporal fossa | Cochlear implant, middle fossa approach |
| Extended postauricular | Tympanomastoid + neck + ITF | Infratemporal fossa tumors, jugular paraganglioma |
(Based on: Entokey Incisions and Approaches; Stanford Oto Surgery Atlas, Jackler & Gralapp)
PART 2 - Types of Endoscopic Tympanomastoid Surgery
Endoscopic ear surgery (EES) has evolved rapidly over the past decade. The principal modality is Transcanal Endoscopic Ear Surgery (TEES), which uses rigid angled endoscopes (0°, 30°, 45°, and even 70°) inserted through the natural EAC to perform middle ear, tympanoplasty, mastoid, and even lateral skull base procedures - without any external incision.
A. Classification of Endoscopic Ear Surgery (TEES Classification System)
The most widely accepted classification divides TEES into three categories based on the extent of disease and approach used:
Type 1 - Exclusive (Purely Endoscopic, Transcanal)
All dissection is performed entirely through the EAC using the endoscope alone. No postauricular or external incision.
- Used for: Myringoplasty, tympanoplasty (limited perforations), stapedectomy, ossiculoplasty, attic cholesteatoma limited to epitympanum, exploration of middle ear recesses (sinus tympani, facial recess)
- The endoscope replaces the microscope entirely
- Single hand holds the endoscope; the other hand works instruments
Type 2 - Endoscope-Assisted (Combined Endoscopic + Microscopic)
The microscope is used as the primary visualization tool for the main surgical procedure, but the endoscope is introduced at key points to visualize otherwise blind areas.
- Used for: Combined approach tympanoplasty for cholesteatoma, second-look procedures after microscopic canal wall up mastoidectomy, identification of residual disease in the sinus tympani or facial recess
- Particularly valuable for inspecting the posterior mesotympanum through the facial recess
- Reduces the residual/recurrent cholesteatoma rate by identifying disease invisible to the angled microscope
Type 3 - Extended Endoscopic (Endoscopic with External Approach)
A combined endoscopic transcanal approach supplemented by a postauricular (or other external) incision when the extent of disease exceeds purely transcanal access.
- Used for: Large cholesteatomas with extensive mastoid involvement, cases requiring canal wall down or open mastoidectomy, endoscopic open tympanoplasty for attic and antral cholesteatoma in sclerotic mastoids
- The mastoid is drilled from behind (postauricular), and the endoscope is used trancanally for the tympanic/epitympanic components
B. Specific Endoscopic Tympanomastoid Procedures
1. Endoscopic Tympanoplasty (Myringoplasty)
- Performed entirely transcanally with the endoscope
- The graft (cartilage, temporalis fascia via separate small incision above the ear, or fat) is placed under/over the TM
- Closure rates comparable to microscopic approach (endoscopic: ~85%, microscopic: ~86.4%)
- Advantage: no postauricular incision, shorter operating time, lower morbidity
2. Endoscopic Atticotomy
- Transcanal removal of the scutum to expose the lateral epitympanum
- Piezosurgery or chisel used to remove the lateral attic wall
- Indicated for attic cholesteatomas
- The attic is reconstructed with cartilage at the end
3. Endoscopic Canal Wall Up Tympanomastoidectomy (with or without microscope)
- The lateral attic wall is removed trancanally with the endoscope (atticotomy)
- If mastoid involvement is limited, the entire procedure can be endoscopic
- Endoscope provides unparalleled views of the facial recess, sinus tympani, and retrotympanum - areas notorious for residual cholesteatoma after microscopic surgery
- Facial recess can be drilled and inspected endoscopically without posterior tympanotomy
4. Endoscopic Canal Wall Down (Open) Tympanoplasty
- Introduced for sclerotic mastoid or attic cholesteatoma with antral extension
- The endoscopic "open" technique provides a wide atticotomy to expose and exteriorize the antrum, left open toward the EAC (analogous to classical CWD)
- Avoids postauricular incision in select cases with sclerotic mastoid
5. Endoscopic Second-Look Mastoidoscopy
- After primary microscopic canal wall up mastoidectomy for cholesteatoma
- Endoscope introduced trancanally (or through the mastoid cavity) ~12 months postoperatively
- Inspects for residual disease in the mastoid antrum, epitympanum, sinus tympani, and facial recess
- McKennan (1993) first described this as "endoscopic second look mastoidoscopy"
6. Endoscopic Stapedectomy / Stapedotomy
- Fully transcanal, no external incision
- The endoscope provides a wider field of view of the oval window niche than the monocular microscope
- Comparable outcomes to microscopic stapedotomy
7. Endoscopic Sinus Tympani and Retrotympanum Exploration
- The sinus tympani (posterior recess behind the facial nerve) is notoriously invisible to the operating microscope
- The sinus tympani has been classified into three types based on depth:
- Type A: Shallow - fully explorable endoscopically
- Type B: Deep - explorable endoscopically
- Type C: Deep with posterior extension behind the facial nerve - NOT fully accessible even endoscopically
- The endoscope (30° or 45° angled) allows direct visualization and removal of cholesteatoma from this recess
8. Endoscopic Transpromontorial Approach (Lateral Skull Base)
- Most advanced application of TEES
- The entire cochlea and vestibule are drilled through the external canal and middle ear after ossicular removal
- Provides access to the internal auditory canal (IAC) for acoustic neuroma removal
- Preserves the posterior fossa dura approach entirely from the transcanal route
C. Advantages of Endoscopic Over Microscopic Tympanomastoid Surgery
| Feature | Endoscope | Microscope |
|---|---|---|
| External incision | Not required (TEES type 1) | Required (postauricular/endaural) |
| Field of view | Wide-angle, panoramic | Narrow, monocular |
| Angled views | Yes (30°, 45°) - visualizes hidden recesses | No - blind spots in sinus tympani, facial recess |
| One-handed surgery | Yes (scope in one hand) | Both hands free |
| Learning curve | Steeper (loss of binocular depth) | Standard training |
| Perforation closure | ~85% | ~86% (comparable) |
| Hospital stay | Shorter | Longer |
| Residual cholesteatoma | Lower rates (better recess inspection) | Higher rates in blind areas |
D. Limitations of TEES
- One hand always holds the endoscope (one-handed dissection)
- Loss of stereoscopic (binocular) depth perception
- Heat from the endoscope tip (irrigation needed to prevent inner ear thermal injury)
- Blood and secretions obscure the lens
- Cannot fully access Type C sinus tympani (deep, behind facial nerve)
- Extensive mastoid disease still requires combined or postauricular approach (Type 3 TEES or conventional mastoidectomy)
References
- Stanford Oto Surgery Atlas (Jackler & Gralapp) - Endaural and Postauricular Incision chapters
- Entokey: "Incisions and Approaches" - Chapter 9
- PMC 11546356: Villari D et al. "Endoscopic Ear Surgery, from the Last Ten to the Next Ten Years: A Critical Perspective" (2024)
- K.J. Lee's Essential Otolaryngology - Endoscopic tympanoplasty outcomes
- Scott-Brown's Otorhinolaryngology - Surgical approaches for paediatric cholesteatoma; minimally invasive second-look CAT
This is a shared conversation. Sign in to Orris to start your own chat.