How to identity pneumonia in chest X ray
Reading File
Finding Sources
Searching the Web
pneumonia chest X-ray findings identification radiology signs
Finding Sources
Loading Image
Finding Sources
Searching the Web
lobar pneumonia vs bronchopneumonia vs atypical pneumonia chest xray differences
Reading File
Loading Image
Loading Image
Loading Image
Finding Sources
Reading File
Loading Image
Loading Image
Here is a thorough guide on identifying pneumonia on a chest X-ray, sourced from Grainger & Allison's Diagnostic Radiology and Murray & Nadel's Textbook of Respiratory Medicine.
Identifying Pneumonia on Chest X-Ray
The Core Finding: Opacity (White Area) in the Lung
On a normal chest X-ray, lungs appear dark (air-filled). In pneumonia, alveoli fill with fluid, pus, or inflammatory cells, making the affected area appear white/opaque. The pattern of this opacity helps identify the type and likely cause.
Step 1: Look at the Chest X-Ray Systematically
Use a PA (posteroanterior) view as the primary film. A lateral view helps localize the affected lobe. Key areas to compare:
- Left vs. right lung fields
- Upper, middle, and lower zones bilaterally
- Look for any area that is denser (whiter) than surrounding lung
Three Main Radiological Patterns of Pneumonia
(Grainger & Allison's Diagnostic Radiology)
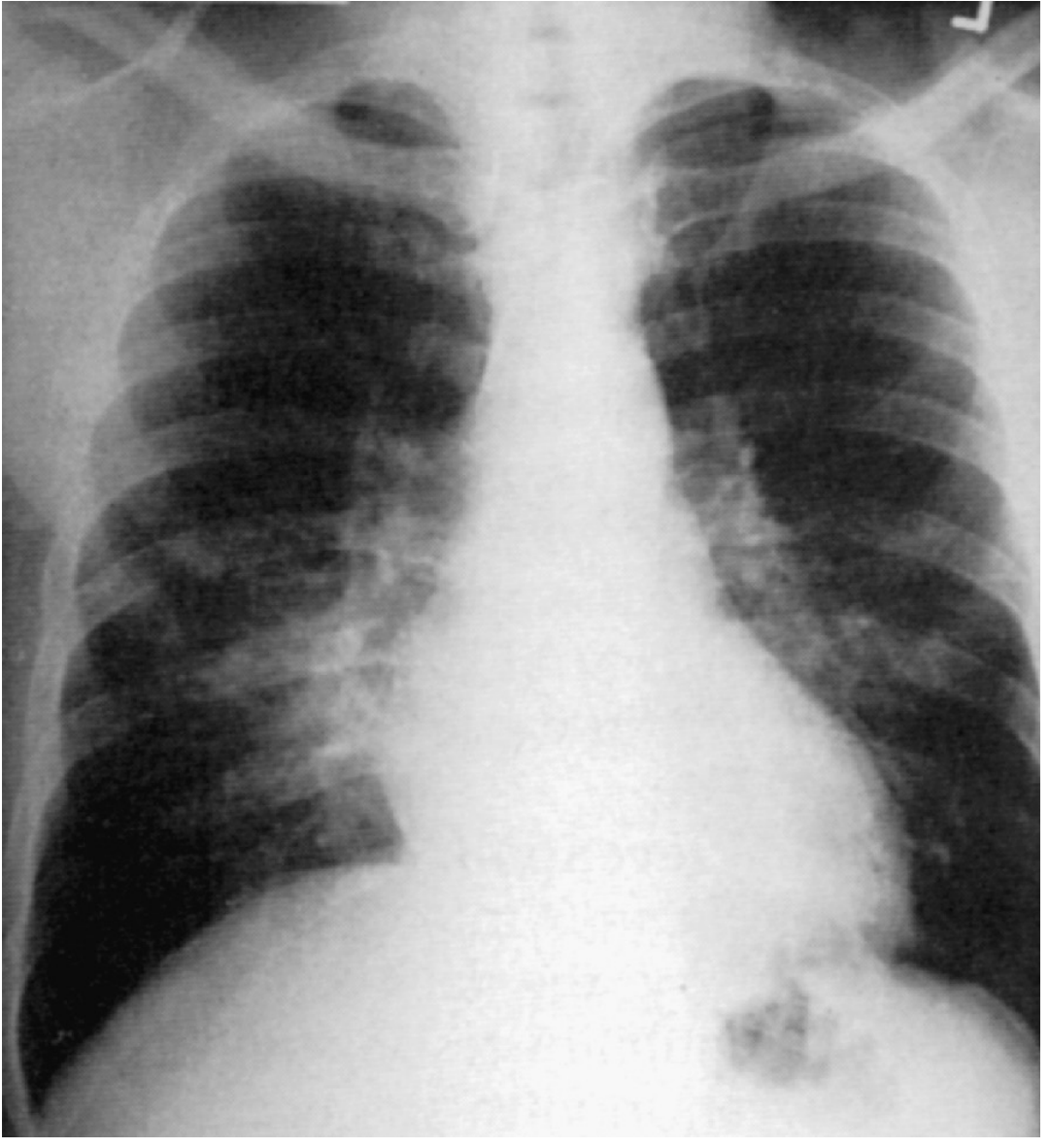
1. Lobar Pneumonia (most classic)

- Homogeneous (uniform) white opacity filling a segment or entire lobe
- Margins are sharply demarcated at fissures
- The opacity spreads via air drift (pores of Kohn) - does NOT cross fissures
- Air bronchogram is frequently seen (dark branching lines of bronchi visible inside the white opacity - because the airways remain open but alveoli are filled)
- Most common cause: Streptococcus pneumoniae (also Klebsiella, Legionella, H. influenzae)
- No significant volume loss - the lobe maintains its size
2. Bronchopneumonia (Lobular Pneumonia)
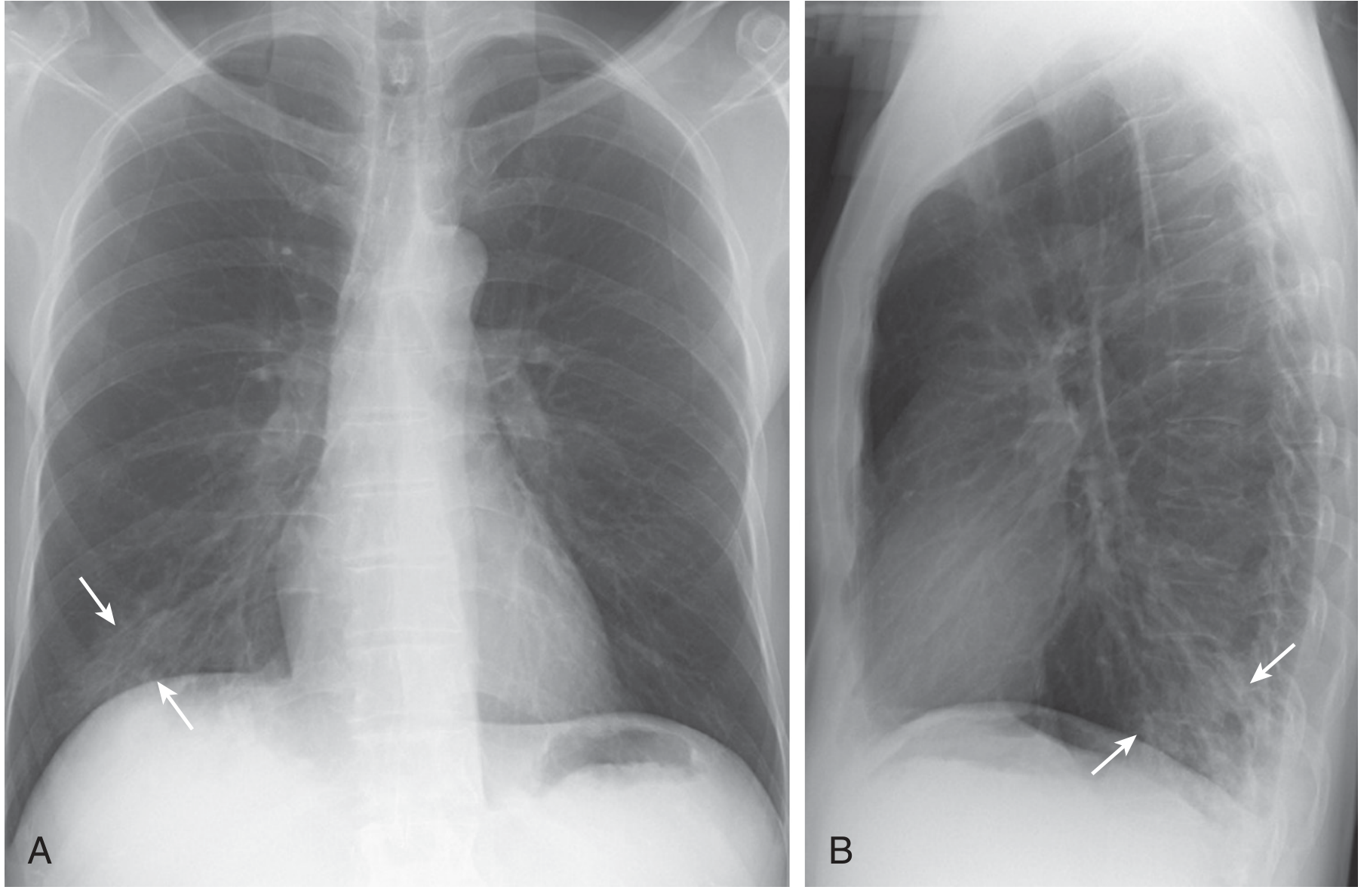
- Patchy, multifocal opacities in multiple lobules/segments - does not neatly fill one lobe
- Peribronchial inflammation that spreads outward
- Poorly defined margins
- Often bilateral, lower lobe predominant
- Common causes: H. influenzae, S. aureus, Mycoplasma, gram-negative organisms
3. Interstitial (Atypical) Pneumonia
- Diffuse, bilateral hazy opacities - a "ground-glass" pattern
- Bronchovascular thickening (thickened lung markings radiating from the hilum)
- Less dense opacification than lobar pneumonia
- Can appear almost normal early in the disease
- Common causes: Mycoplasma pneumoniae, Chlamydia, Legionella, viruses, Pneumocystis jirovecii (PCP)
- Note: In PCP (especially with HIV), the CXR can be completely normal in up to 10% of cases
Key Radiological Signs to Know
| Sign | What It Means |
|---|---|
| Air bronchogram | Dark airways visible inside white opacity - confirms true consolidation (not collapse) |
| Silhouette sign | Loss of the normal border between lung and adjacent structure (e.g., right heart border lost = right middle lobe; left heart border lost = lingula; diaphragm lost = lower lobe) |
| Consolidation | Dense white opacity where alveoli are filled; does not move with bronchi |
| Pleural effusion | Blunting of costophrenic angle - fluid alongside the lung |
| Cavitation | A lucency (dark area) within the consolidation = abscess (classic: S. aureus, Klebsiella, anaerobes, TB) |
Lobe Localization Using the Silhouette Sign
The silhouette sign is one of the most useful tricks:
- Right heart border obscured → right middle lobe pneumonia
- Left heart border obscured → left upper lobe / lingula pneumonia
- Right/left diaphragm obscured → right/left lower lobe pneumonia
- Aortic knuckle obscured → left upper lobe pneumonia
Special Patterns
Round Pneumonia
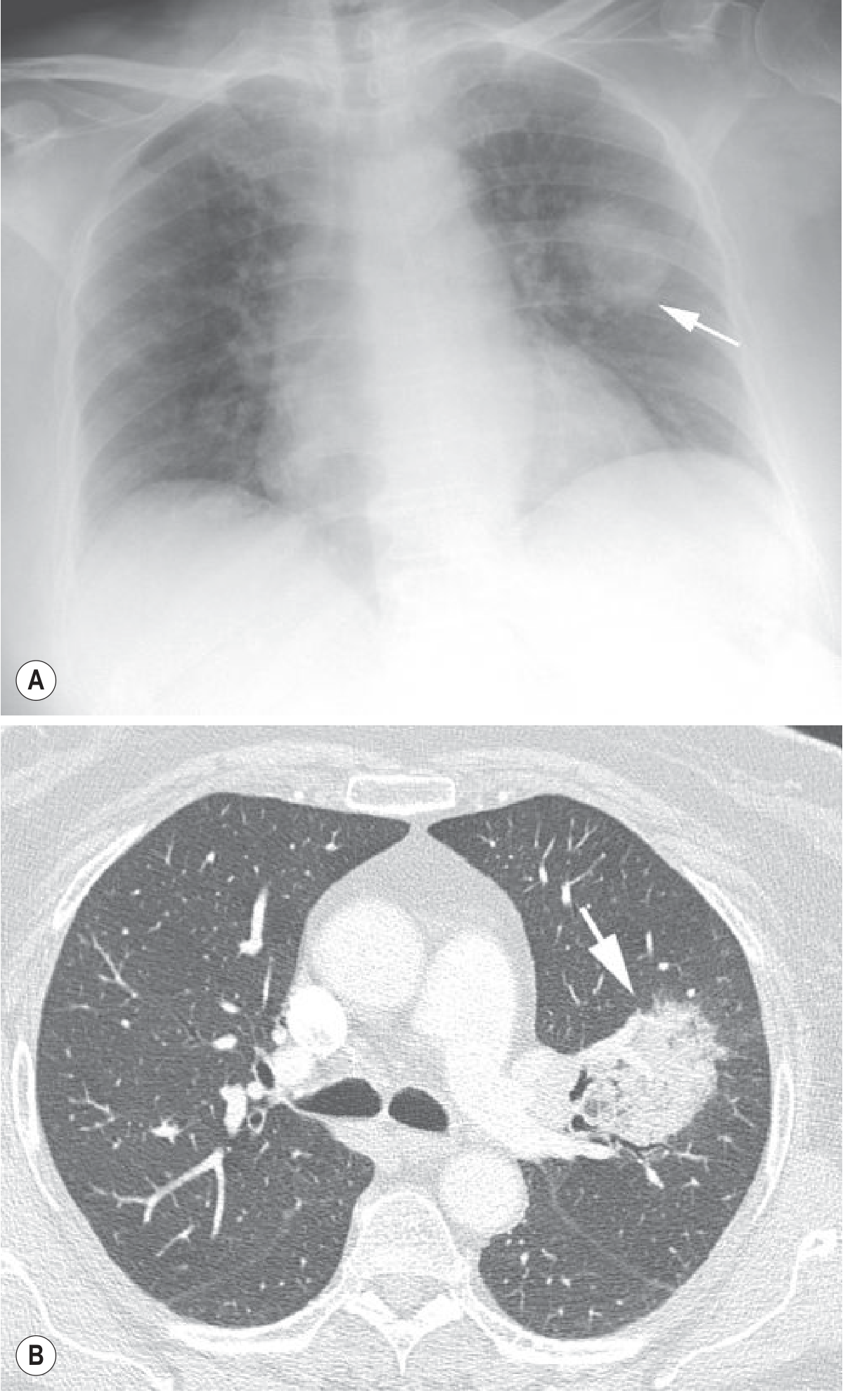
- A spherical/ball-like area of consolidation
- Can mimic a lung tumor
- More common in children; resolves with antibiotics
Cavitating Pneumonia
- Consolidation with an air-fluid level or internal lucency inside
- Caused by: S. aureus (MRSA), Klebsiella, anaerobes, TB
- Indicates necrosis/abscess formation
Bilateral Consolidation Patterns
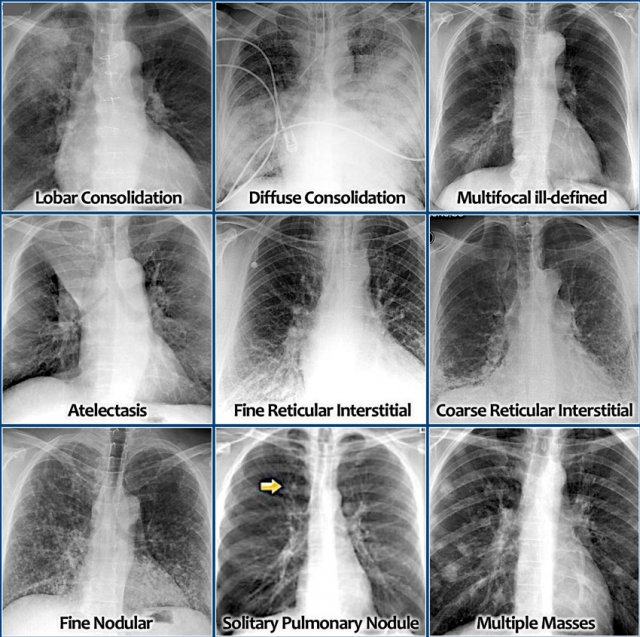
The image above shows the range of lung densities you may encounter on a CXR, from lobar consolidation to fine reticular interstitial patterns.
Practical Approach Summary
- Is there an opacity? - Compare both lungs systematically
- Is it dense and homogeneous (lobar) or patchy (bronchopneumonia)?
- Look for air bronchograms - confirms consolidation, not collapse
- Apply the silhouette sign - which heart/diaphragm border is lost?
- Any pleural effusion? - blunted costophrenic angle
- Any cavitation? - suggests abscess (MRSA, Klebsiella, anaerobes)
- Bilateral diffuse hazy opacities? - think atypical organisms, viral, PCP
- Always correlate with clinical findings - fever, cough, pleuritic chest pain, sputum
Important note: The CXR cannot reliably identify the specific organism. The radiological pattern narrows the differential but microbiologic confirmation (sputum culture, urine antigen) is required for definitive diagnosis. The CXR may also lag behind clinical improvement by several weeks.
Sources: Grainger & Allison's Diagnostic Radiology; Murray & Nadel's Textbook of Respiratory Medicine, 2-Volume Set
This is a shared conversation. Sign in to Orris to start your own chat.