Nenu hernia ni reduce cheyyalekapothunna manual ga ,kaani on lying down reduce avthundhi
Reading File
Finding Sources
Searching the Web
hernia reduces lying down but not manually standing reducible hernia management
Reading File
Reading File
Mee situation chala clearly explain chesanu - idi Telugu lo detailed ga answer istanu:
Mee Hernia Gurinchi - Reducible Hernia
Mee condition enti?
Mee hernia oka reducible hernia - idi dangerous kadu, kaani surgery avashyam.
- Padukunnappudu reduce avvadam - Gravity help cheyyadam valla, abdominal pressure takkuva avvadam valla hernia contents (intestine/fat) tama jagake veltai
- Nilu chukkunnappudu manual ga reduce cheyyalekavadam - Standing position lo intra-abdominal pressure ekkuva untundi, anduke manually push cheyyatam kashtam
Idi "reducible hernia" ki chala common finding - Bailey and Love's Surgery textbook lo cheppinatluga, idi still manageable but surgical repair avashyam.
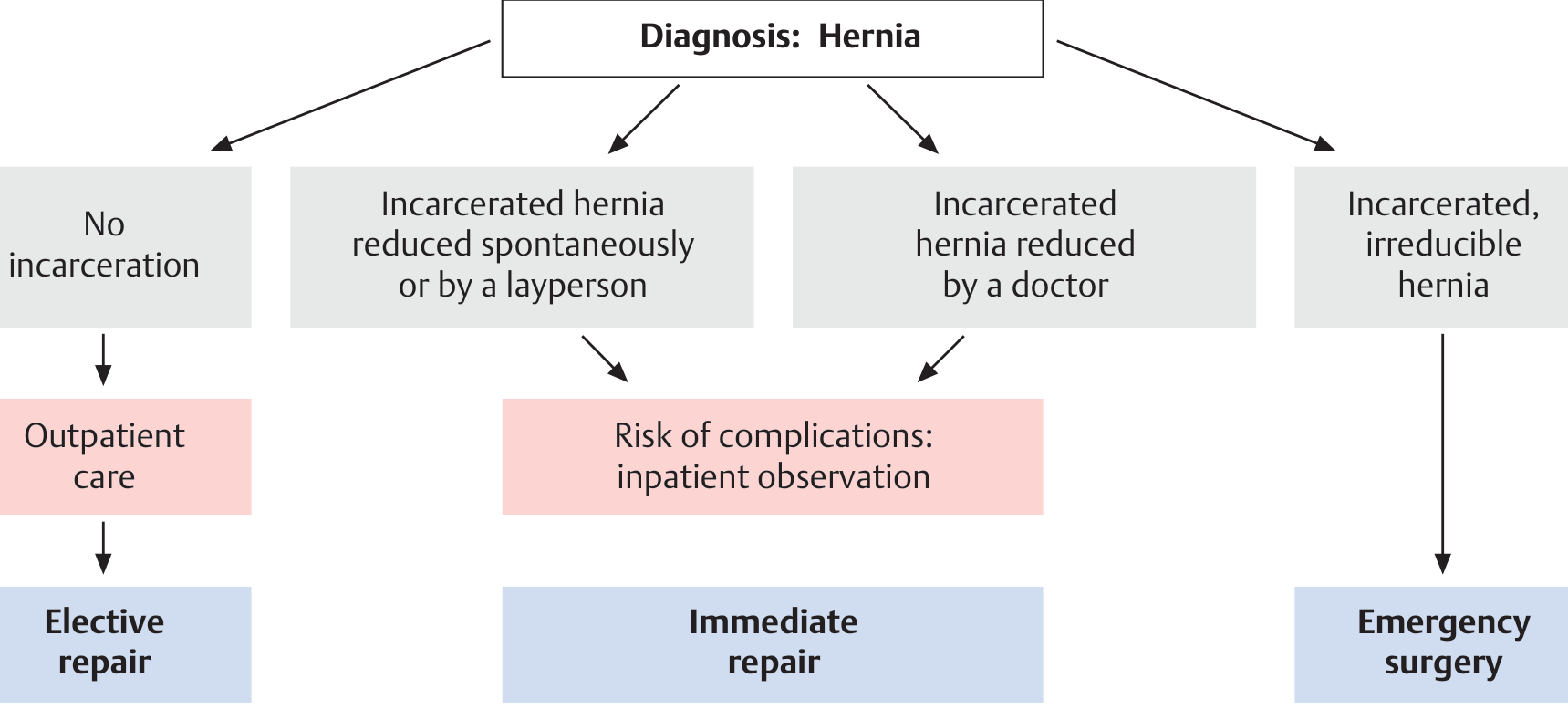
Hernia Rakalu - Meeru Eppudu Worry Cheyali?
| Type | Characteristics | Urgency |
|---|---|---|
| Reducible (Mee case) | Padukunnappudu/manually reduce avutundi | Elective surgery plan cheyyandi |
| Irreducible / Incarcerated | Empatikee reduce kaadu | Urgent surgery |
| Strangulated | Pain + fever + vomiting, reduce kaadu | Emergency surgery |
Warning Signs - Immediately Hospital ki Vellaali
Ivi emi vasthe twaraga hospital ki vellaali:
- Hernia spot lo sudden severe pain
- Hernia hard/firm ga feel avvadam (previously soft ga undevaru)
- Vomiting / Nausea
- Fever
- Hernia skin red/dark avvadam
- Hernia padukunnappudu kuda reduce kaakavadam
Ivvanni strangulation signs - blood supply cut avvadam valla bowel damage jarugatundi. Idi life-threatening emergency.
Ippudu Cheyaalsindi Enti?
Short term (ippudu):
- Hernia ki truss/support belt use cheyyavachu - kaani idi permanent solution kadu
- Heavy lifting avoid cheyyandi
- Constipation avoid cheyyandi (straining pressure ekkuva chestundi)
- Padukunnappudu reduce avutundhi kabatti ippudu stable ga unnaru
Long term:
- Surgical repair - Idi only permanent solution. Hernias conservative treatment tho completely cure kaadu (Bailey and Love's Surgery textbook lo clearly cheppinaru: "hernias do not respond definitively to conservative treatment, and a permanent reduction is achieved only by surgical closure")
- Surgery options: Open repair (Shouldice/Lichtenstein mesh) or Laparoscopic repair
Hernia Type Edi Untundi Meeru?
- Inguinal hernia (groin/thigh area - most common, especially men lo)
- Umbilical hernia (navel area)
- Incisional hernia (previous surgery scar lo)
- Femoral hernia (inner thigh)
Mee hernia exact location cheppite, specific ga oka surgeon ki chupiyatam best option.
Bottom line: Mee hernia reducible ga undi - idi good sign, immediate emergency kaadu. Kaani idi surgeon ki chupiyandi, elective surgery plan cheyyandi. Delay chesthe incarceration/strangulation risk untundi, especially first few years lo risk ekkuva ga untundi (Maingot's textbook data).
Disclaimer: Idi general medical information matrame. Proper diagnosis ki oka general surgeon ki consult cheyyandi - in-person examination chala important.
Hernia different operation
Finding Sources
Searching the Web
hernia surgery types open laparoscopic robotic techniques comparison 2024
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Hernia operations anni types lo detail ga explain chestanu - Bailey & Love's Surgery, Sabiston Surgery, and Fischer's Mastery of Surgery textbooks nundi.
Hernia Operations - Anni Types
Mee Hernia ki Surgery Eppudu?
Mee case la (reducible hernia) - idi "Elective Repair" category:
Operations - Rendu Main Categories
1. OPEN SURGERY (Pedda Cut)
A) Suture Repairs (Mesh lekundane, tissue tho repair)
| Operation | Ela Chestaru | Advantage |
|---|---|---|
| Bassini | Tissue layers ni tight ga suture chestaru | Old classic technique |
| Shouldice | 4-layer continuous suture repair | Low recurrence, no mesh |
| Desarda | Aponeurosis strip use chestaru | Mesh-free, physiological |
Ivi "tension repair" antaru - mesh vadaniki bayapadeyavallu ki, young patients ki suitable.
B) Mesh Repairs (Net lanti material vaddhi repair)
Lichtenstein Repair - Idi currently world lo most common operation!
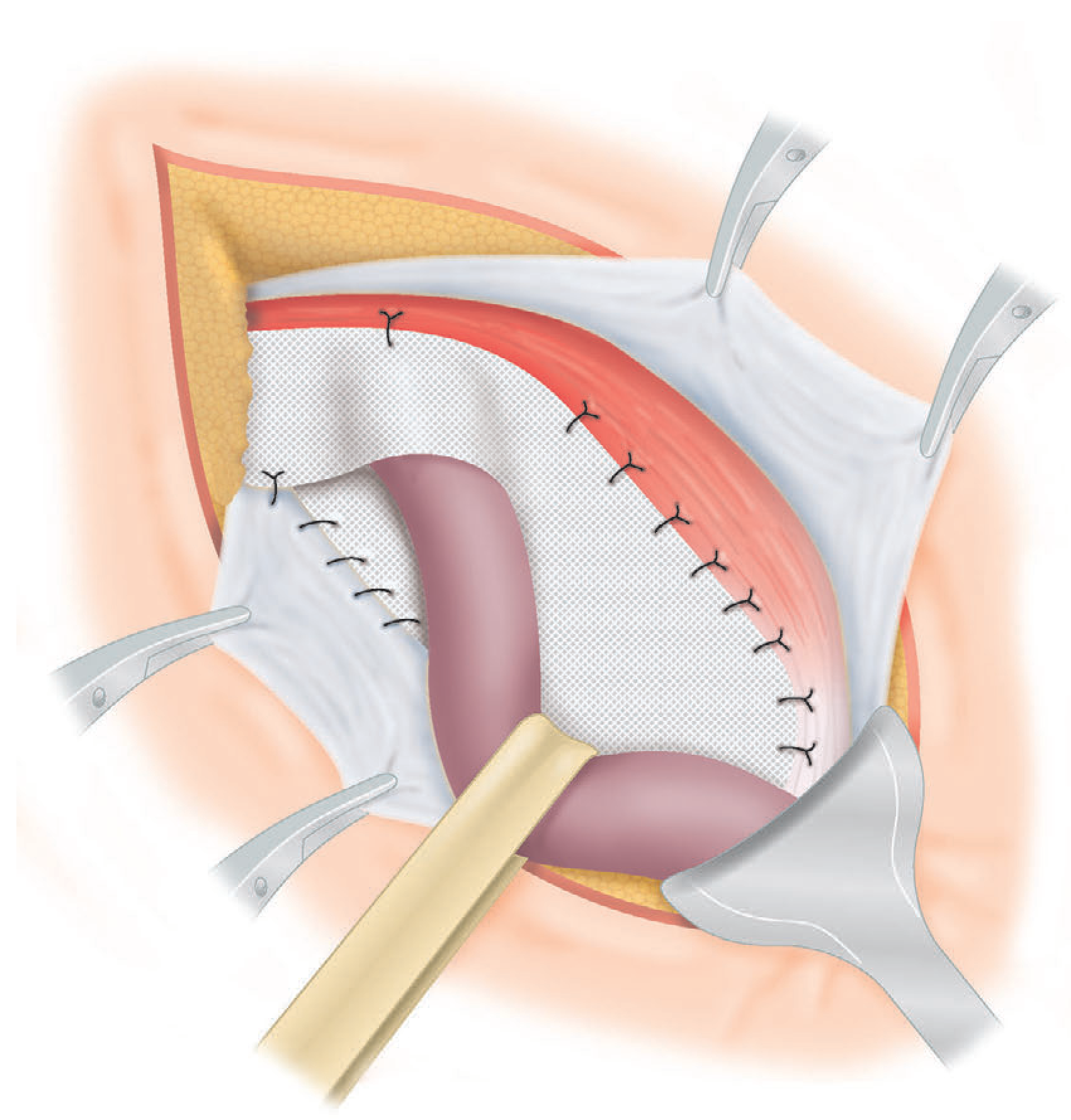
Above: Polypropylene mesh inguinal canal posterior wall paina place cheyyadam - Lichtenstein Repair
- 8x15 cm flat polypropylene mesh posterior wall paina place chestaru
- Spermatic cord chuttu slit chestaru mesh ki
- "Tension-free repair" - recurrence chala takkuva
- Recurrence rate: <1-2%
- Disadvantage: Chronic pain 20% lo vachindi reports lo
C) Plug Repair
- Cone-shaped mesh plug hernia defect lo pettadaru
- Simple, fast
- Risk: Plug migrate/erode avvachu - not recommended by European Hernia Society 2018 guidelines
D) Stoppa / Open Preperitoneal Repair
- Midline incision tho, mesh peri-peritoneal plane lo vesdaru
- Multiple recurrences ayyina patients ki useful
- Ippudu laparoscopic surgery tho largely replace ayyindi
2. LAPAROSCOPIC SURGERY (Keyhole / 3 Small Holes)
Idi modern, less painful approach. Rendu types unnai:
TEP - Totally Extraperitoneal Repair
- Peritoneal cavity enter kaadu
- Abdomen muscles vennakala space lo work chestaru
- Safer for bowel/internal organs
- Most preferred laparoscopic technique
TAPP - Transabdominal Preperitoneal Repair
- Peritoneal cavity ki enter avutaru first
- Peritoneum cut chesi preperitoneal space lo mesh vesdaru
- Bilateral hernias ki, recurrent hernias ki especially useful
Both TEP & TAPP lo:
- 10x15 cm mesh preperitoneal plane lo place chestaru
- Hesselbach's triangle + deep inguinal ring + femoral canal anni cover avutundi
3. ROBOTIC SURGERY (Robot-Assisted)
- Laparoscopic tho same principle, robot arms use chestaru
- Surgeon enhanced 3D view untundi
- Ergonomically comfortable for surgeon
- Patient benefit - laparoscopic tho compare chesthe significantly different kadu
- Cost ekkuva - simple hernia ki justify cheyyadam kashtam
Open vs Laparoscopic - Comparison
| Feature | Open (Lichtenstein) | Laparoscopic (TEP/TAPP) |
|---|---|---|
| Cut size | 5-8 cm | 3 small holes (5-10 mm) |
| Pain after surgery | Ekkuva | Takkuva |
| Recovery time | 2-4 weeks | 1-2 weeks |
| Return to work | Longer | Faster |
| Bilateral hernias | 2 separate cuts | Oka operation lo rendu fix |
| Recurrence ki best | Not ideal | Best option |
| Chronic pain risk | ~20% | Takkuva |
| Learning curve | Easy | Long learning curve |
| Cost | Takkuva | Ekkuva |
| Anesthesia | Local/General possible | General anesthesia must |
Mee Case ki Which Surgery Best?
Bailey & Love's Surgery lo cheppinatluga: "No one operation suits all hernias" - surgeon skills, hernia type, patient age anni consider chestaru.
Mee case ki likely Lichtenstein (open mesh) or TEP laparoscopic - surgeon decide chestadu.
Oka General Surgeon ni consult cheyyandi - mee hernia size, type, location chusi decide chestadu. Surgery simple, same-day / 1 day admission lo avutundi most cases lo.
Sources: Bailey and Love's Surgery 28th Ed, Sabiston Textbook of Surgery, Fischer's Mastery of Surgery 8th Ed, Current Surgical Therapy 14th Ed
Eye sign absent in graves
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Searching the Web
eye sign absent in Graves disease Mobius sign convergence loss ophthalmopathy
Finding Sources
Reading Web Page
https://morancore.utah.edu/section-07-orbit-eyelids-and-lacr…
Loading Image
Ippudu complete ga answer ivvagalanu - Harrison's Internal Medicine (2025) + Moran Eye Center source nundi.
Graves' Disease - Eye Signs
Absent Sign (Most Important Exam Answer)
Argyll Robertson Pupil sign - ABSENT in Graves' disease
Kaani exam question "eye sign absent" antే most likely answer:
✦ Möbius Sign - Graves lo PRESENT ayinappatiki IMPAIRED/LOST
Möbius Sign = Convergence weakness / failure
- Near object ni chustunnappudu rendu eyes converge cheyyalekavadam
- Graves' disease lo extraocular muscles weak avvadam valla convergence lose avutundi
- Patient ki double vision undadu, kaani convergence fail avutundi
- Absent/impaired convergence = Möbius sign
Graves' Disease - Complete Eye Signs List
📋 Named Signs (Eponyms)
| Sign | What it means |
|---|---|
| Dalrymple's sign | Upper lid retraction - palpebral fissure wide ga untundi (staring look) |
| Von Graefe's sign | Downward gaze lo upper lid lag - lid globe tho radu |
| Stellwag's sign | Infrequent / incomplete blinking |
| Möbius sign | Convergence weakness - near object focus fail |
| Joffroy's sign | Upward gaze lo forehead wrinkle absent |
| Kocher's sign | Upward gaze lo globe lid vennakala lag cheyyadu |
| Boston's sign | Downward gaze lo upper lid jerky movement |
| Enroth's sign | Upper lid edema near supraorbital margin |
| Gifford's sign | Upper lid evert cheyyatam difficult |
Harrison's (2025) - NO SPECS Classification

| Class | Finding |
|---|---|
| 0 | No signs or symptoms |
| 1 | Only signs - lid retraction or lag |
| 2 | Soft tissue - periorbital edema |
| 3 | Proptosis (>22 mm) |
| 4 | Extraocular muscle involvement - diplopia |
| 5 | Corneal involvement |
| 6 | Sight loss (optic nerve compression) |
Key Pathophysiology
- Lid retraction + lid lag - Sympathetic overactivity valla (any hyperthyroidism lo vachadu)
- Proptosis/Exophthalmos - Orbital fat + extraocular muscle GAG deposition (Graves' specific)
- Convergence weakness - Extraocular muscle involvement valla
- Diplopia - Inferior rectus most commonly affected (upgaze fail)
Exam Point - Absent Sign Memory Trick
"Argyll Robertson" sign - Graves lo absent (idi neurosyphilis sign)
Graves lo specifically NOT seen:
- Pupil abnormalities (pupils normal)
- Pain on eye movement (unless severe)
- Argyll Robertson pupil - absent
Most common MCQ trap: Möbius sign = convergence impaired/absent in Graves - idi sign's finding absent ga untundi (converge cheyyaleru), sign name positive ga cheppukunnadhe.
Sources: Harrison's Principles of Internal Medicine 22nd Ed (2025), Moran Eye Center - University of Utah, LITFL Medical Eponym Library
What is argyll robertson pupil sign
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Excellent sources dorikayi - ippudu complete detailed answer ivvagalanu.
Argyll Robertson Pupil
Core Definition - "Prostitute's Pupil"
"Accommodates but does not react" Light ki react kaadu - Accommodation ki react avutundi
This is called Light-Near Dissociation - idi key feature.
Features - Easy Memory
| Feature | Finding |
|---|---|
| Pupil size | Small (miotic) - < 2 mm, bilateral |
| Shape | Irregular |
| Light reflex | ABSENT - light vetchina constrict kaadu |
| Consensual reflex | ABSENT |
| Accommodation reflex | PRESENT and brisk - near object chusthe constrict avutundi |
| Bilaterality | Bilateral usually |
Memory Trick
"Prostitute's pupil" - oka famous medical mnemonic:
- Prostitute = Accommodates (adjust avutundi) ✅
- But does NOT react to light ❌
(Slightly crude, but medically widely used mnemonic)
Causes
Classic cause:
- Neurosyphilis (Tertiary syphilis) - most classic, original description
Modern cause (more common now):
- Diabetes mellitus - ippudu most common cause ga consider chestunnaru
- Kaani diabetic pupils miotic kaavu (AR pupils tho puri difference)
Other causes:
- Sarcoidosis
- Lyme disease
- Multiple sclerosis
- Alcoholic neuropathy
- Encephalitis
Mechanism / Pathophysiology
Lesion - Dorsal midbrain (pretectal area) lo:
Light → Retina → Optic nerve → Pretectal nucleus (DAMAGED)
↓ (blocked)
Edinger-Westphal nucleus
↓ (blocked)
Ciliary ganglion → Pupil constriction ❌
Near Response pathway → More VENTRAL → SPARED ✅
→ Accommodation + convergence → Pupil constricts normally ✅
- Dorsally located olivary pretectal nuclei (light reflex pathway) - damaged
- Ventrally located near-response fibers - spared
- Result: Light reflex gone, near reflex intact
Differentiation from Other Pupils
| Feature | AR Pupil | Adie's (Tonic) Pupil | Horner's Pupil |
|---|---|---|---|
| Size | Small, bilateral | Large, unilateral | Small, unilateral |
| Shape | Irregular | Irregular | Regular |
| Light reflex | Absent | Sluggish/absent | Normal |
| Near reflex | Brisk, normal | Slow, tonic, delayed | Normal |
| Cause | Syphilis/DM | Ciliary ganglion damage | Sympathetic chain |
| Associated | Neurosyphilis | Young women, absent DTRs | Ptosis, anhidrosis |
Key Exam Points
- Light-Near Dissociation = AR pupil ki hallmark
- Small + Irregular + Bilateral = AR pupil typical appearance
- Classic = Neurosyphilis, Common now = Diabetes
- Lesion = Dorsal midbrain / pretectal nucleus
- Graves' disease lo ABSENT - (Graves lo pupils normal, lid signs unnai)
- Near reflex brisk - idi Adie's tonic pupil tho differentiate cheyyadam ki help chestundi (Adie's lo near reflex slow/sustained)
Sources: Localization in Clinical Neurology 8th Ed, Bradley & Daroff's Neurology in Clinical Practice, Goldman-Cecil Medicine
Signs of hyper and hypo thyroiidism
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Harrison's Internal Medicine (2025) + Tietz Lab Medicine nundi complete data dorikayi. Ippudu detailed comparison ivvagalanu.
Hyper vs Hypothyroidism - Complete Signs & Symptoms
Simple Rule to Remember
| Hyperthyroidism | Hypothyroidism | |
|---|---|---|
| Body | Everything FAST / HOT / UP | Everything SLOW / COLD / DOWN |
| Metabolism | Ekkuva | Takkuva |
🔥 HYPERTHYROIDISM (Thyrotoxicosis)
Symptoms (Patient cheppedhi)
| System | Symptoms |
|---|---|
| General | Weight loss (ekkuva tintunnaro kuda), heat intolerance (heat lo uncomfortable), excess sweating |
| Heart | Palpitations, breathlessness on exertion, chest pain |
| Gut | Increased appetite, frequent stools/diarrhea, nausea |
| Neuro/Mind | Anxiety, irritability, restlessness, insomnia, tremor |
| Muscles | Weakness, fatigue (proximal myopathy) |
| Menstrual | Oligomenorrhea (periods takkuva avvadam) |
| Eyes | (Graves' specific) - grittiness, tearing, bulging |
Signs (Doctor chusedhi)
| System | Signs |
|---|---|
| Vital signs | Tachycardia (fast pulse), systolic hypertension, wide pulse pressure |
| Skin | Warm, moist, smooth skin; fine hair; onycholysis (nail separation - Plummer's nail) |
| Eyes | Lid retraction (staring look), lid lag (Von Graefe's), exophthalmos/proptosis (Graves') |
| Thyroid | Goiter, bruit over thyroid |
| Neuro | Fine tremor of outstretched hands, hyperreflexia |
| Heart | AF (atrial fibrillation), cardiac failure in elderly |
| Muscles | Proximal muscle wasting |
Graves' Specific (Only in Graves' disease)
- Exophthalmos / Proptosis - eye bulging
- Pretibial myxedema - shin lo orange-peel skin (< 5% patients)
- Thyroid acropachy - clubbing (< 1% patients)
🧊 HYPOTHYROIDISM (Myxedema)
Symptoms (Harrison's 2025 - Descending frequency)
| Symptoms | Signs |
|---|---|
| Tiredness, weakness | Dry, coarse skin; cool peripheries |
| Dry skin | Puffy face, hands, feet (myxedema) |
| Feeling cold (cold intolerance) | Diffuse alopecia (hair loss) |
| Hair loss | Bradycardia |
| Poor concentration, poor memory | Peripheral edema |
| Constipation | Delayed tendon reflex relaxation |
| Weight gain (poor appetite tho) | Carpal tunnel syndrome |
| Dyspnea (breathlessness) | Serous cavity effusions (pericardial/pleural) |
| Hoarse voice | |
| Menorrhagia (heavy periods - later amenorrhea) | |
| Paresthesia (tingling) | |
| Impaired hearing |
Side-by-Side Comparison - System by System
| System | Hyperthyroidism | Hypothyroidism |
|---|---|---|
| Weight | Loss ↓ | Gain ↑ |
| Appetite | Increased | Decreased |
| Temperature | Heat intolerance, sweating | Cold intolerance |
| Heart rate | Tachycardia (fast) | Bradycardia (slow) |
| BP | Systolic high, wide pulse pressure | Diastolic high |
| Bowels | Diarrhea / frequent stools | Constipation |
| Skin | Warm, moist, smooth | Dry, coarse, cool |
| Hair | Fine, thinning | Coarse, loss (outer 1/3 eyebrow) |
| Reflexes | Hyperreflexia | Delayed relaxation (Woltman sign) |
| Menstruation | Oligomenorrhea | Menorrhagia (then amenorrhea) |
| Mood | Anxious, irritable | Depressed, slow |
| Memory | Restless, poor focus | Slow cognition, poor memory |
| Voice | Normal | Hoarse |
| Tongue | Normal | Macroglossia (large tongue) |
| Edema | None (usually) | Non-pitting myxedema |
Key Exam Signs - Easy Memory
Hypothyroidism Unique Signs
- Woltman sign = Delayed relaxation of ankle jerk reflex - most specific sign
- Myxedema = Non-pitting edema (GAG deposition) - face, hands, legs
- Outer 1/3 eyebrow loss (Hertoghe's sign)
- Macroglossia - large tongue
- Dry, coarse "dough-like" skin
Hyperthyroidism Unique Signs
- Plummer's nails = Onycholysis - nail bed separation from distal end
- Fine tremor of outstretched hands
- AF in elderly - common presentation
- Thyroid bruit - increased vascularity
TSH / T4 Values (Quick Reference)
| Condition | TSH | Free T4 |
|---|---|---|
| Hyperthyroidism (primary) | ↓ Low | ↑ High |
| Hypothyroidism (primary) | ↑ High | ↓ Low |
| Subclinical Hyper | ↓ Low | Normal |
| Subclinical Hypo | ↑ High | Normal |
Sources: Harrison's Principles of Internal Medicine 22nd Ed (2025), Tietz Textbook of Laboratory Medicine 7th Ed
This is a shared conversation. Sign in to Orris to start your own chat.