How to perform open heart surgery
open heart surgery steps procedure overview cardiothoracic
Open Heart Surgery: Principles, Technique & Steps
1. Indications
- Coronary artery disease requiring CABG
- Valvular disease (aortic stenosis/regurgitation, mitral disease)
- Congenital heart defects (ASD, VSD, tetralogy of Fallot, etc.)
- Aortic aneurysm / dissection
- Heart transplantation
- Cardiac tumours (e.g. myxoma)
2. Pre-operative Preparation
- Full cardiac workup: echocardiogram, coronary angiography, ECG, CXR, lung function
- Anaesthetic assessment and blood typing / cross-matching
- Optimisation of comorbidities (diabetes, renal function, anticoagulants)
- Informed consent covering risks: stroke, bleeding, infection, sternal dehiscence, death
- A detailed preoperative discussion with the patient and family is essential - "Time spent at this stage is always richly rewarded later" - Pye's Surgical Handicraft
3. Anaesthesia
4. Surgical Access - Median Sternotomy
- A vertical skin incision from the suprasternal notch to the xiphisternum
- The sternum is divided in the midline with a sternal saw
- A retractor spreads the sternum, exposing the thymus superiorly and pericardium inferiorly
- The thymus and pleurae are dissected from the pericardium
- The pericardium is opened and stay sutures are placed to create a cradle for the heart
- Bailey & Love's Short Practice of Surgery, 28th ed.
5. Heparinisation
6. Cardiopulmonary Bypass (CPB) - Setting Up
Arterial Cannulation
- A purse-string suture is placed in the ascending aorta (after epiaortic ultrasound to check for calcification/atherosclerosis)
- The aortic cannula is inserted and connected to the arterial limb of the CPB circuit
- Alternative sites (if aorta is unsuitable): femoral artery, axillary artery (preferred - provides antegrade flow, reduces thromboembolic risk)
Venous Cannulation
- A single two-stage venous cannula is placed via the right atrial appendage, with end-holes in the inferior vena cava and side-holes in the right atrium
- Alternatively, bicaval cannulation (separate IVC + SVC cannulae) for operations inside the right heart
- Femoral vein cannulation is an option for minimally invasive or thoracic aortic procedures
The CPB Circuit (Four Key Functions)
- Oxygenation - Blood passes through a membrane oxygenator (CO2 removed, O2 added)
- Pumping - A roller pump (or centrifugal pump) returns oxygenated blood to the patient via the aortic cannula
- Temperature control - A heat exchanger cools the blood (reducing metabolic demands) or rewarms it at the end of bypass
- Filtration - A microfilter (20-30 μm pore size) removes debris and micro-emboli from the arterial line
- Bailey & Love's Short Practice of Surgery, 28th ed.; Pye's Surgical Handicraft, 22nd ed.
7. Myocardial Protection
Cardioplegia (most common method)
- Cardioplegic solution is infused into the coronary circulation
- Antegrade (into the aortic root / coronary ostia) - most common
- Retrograde (via coronary sinus catheter) - used when antegrade access is difficult
- Potassium is the standard arresting agent - causes diastolic arrest by depolarising the cardiac myocyte membrane
- Solutions are cold (4-10°C crystalloid or blood) for hypothermic protection, reducing metabolic needs
- Warm cardioplegia solutions may improve myocardial enzyme activity and recovery
- Must be re-dosed every 15-20 minutes during aortic cross-clamp
Other methods
- Intermittent cross-clamp fibrillation - electrically induced VF stops ejection; heart tolerates 10-20 min ischaemia cycles with reperfusion between
- Deep hypothermic circulatory arrest (DHCA) - body cooled to 15-20°C, allowing up to 60 min of total circulatory arrest; mainly used in infants with congenital defects and complex aortic arch surgery
8. The Operative Repair
| Operation | What is done |
|---|---|
| CABG | Saphenous vein grafts or internal thoracic (mammary) artery anastomosed to coronary arteries distal to obstructions |
| Valve surgery | Valve repaired or replaced (biological or mechanical prosthesis) via atriotomy or aortotomy |
| Septal defect repair | Patch closure (Dacron/pericardium) of ASD or VSD |
| Aortic root surgery | Bentall procedure (composite graft + valve replacement + coronary reimplantation) or valve-sparing root replacement |
| Heart transplant | Recipient cardiectomy + donor heart implantation (bicaval or biatrial anastomosis) |
9. Weaning from CPB & Closure
- The surgical repair is completed and the heart is de-aired (a critical step to prevent air embolism)
- The aortic cross-clamp is removed - coronary flow resumes
- The heart typically resumes beating spontaneously (or is defibrillated if in VF)
- The patient is gradually rewarmed to 37°C via the heat exchanger
- Cardiac function is assessed by TOE and haemodynamic monitoring
- Once adequate cardiac function is confirmed, CPB flow is gradually reduced and stopped
- Protamine is given to reverse heparin
- Cannulae are removed; cannulation sites are sutured
- Haemostasis is meticulously achieved (coagulopathy is common post-CPB)
- Mediastinal and pleural drains are placed
- The sternum is closed with stainless steel wires (sternal wires)
- Subcutaneous and skin layers are closed
10. Post-operative Complications of CPB
| Complication | Mechanism |
|---|---|
| Haemorrhage / coagulopathy | Heparin/protamine imbalance, platelet dysfunction, clotting factor consumption, protein degradation from O2 bubbles |
| Neurological injury / stroke | Microemboli (air, calcific debris, fat), hypoperfusion |
| Renal impairment | Non-pulsatile flow, haemolysis, inflammatory mediators |
| Systemic inflammatory response (SIRS) | Blood contact with non-physiological CPB circuit surfaces activates complement and inflammatory cascades; can progress to multiorgan failure |
| Pulmonary dysfunction | Fluid accumulation, surfactant loss during bypass |
| Low cardiac output syndrome | Myocardial stunning, inadequate protection, pre-existing LV dysfunction |
| Sternal wound infection / mediastinitis | More common in diabetics, obese patients, bilateral ITA harvest |
11. Off-Pump Surgery
Important note: Open heart surgery is one of the most technically demanding procedures in all of surgery, performed only by trained cardiothoracic surgeons with a dedicated team including cardiac anaesthetists, perfusionists, and scrub nurses in a fully equipped cardiac theatre. The above is an educational overview of the principles and steps, not a substitute for formal cardiothoracic surgical training.
Create a visual summary infographic of CPB circuit components
Medical educational infographic showing the Cardiopulmonary Bypass (CPB) circuit components. The diagram should show a clear flow diagram with labeled components connected by arrows indicating blood flow direction. Include: 1) Patient heart with venous cannula in right atrium drawing deoxygenated blood out, 2) Venous reservoir collecting deoxygenated blood, 3) Membrane oxygenator adding oxygen and removing CO2, 4) Heat exchanger for temperature control (cooling/warming), 5) Roller pump driving blood back to patient, 6) Arterial microfilter (20-30 micron) removing debris, 7) Aortic cannula returning oxygenated blood to ascending aorta, 8) Cardioplegia delivery line to coronary ostia, 9) Suction/vent lines returning blood from surgical field. Use blue color for deoxygenated blood flow and red for oxygenated blood flow. Include a legend, title "Cardiopulmonary Bypass Circuit", and small annotations explaining each component's function. Clean, professional medical illustration style on white background.
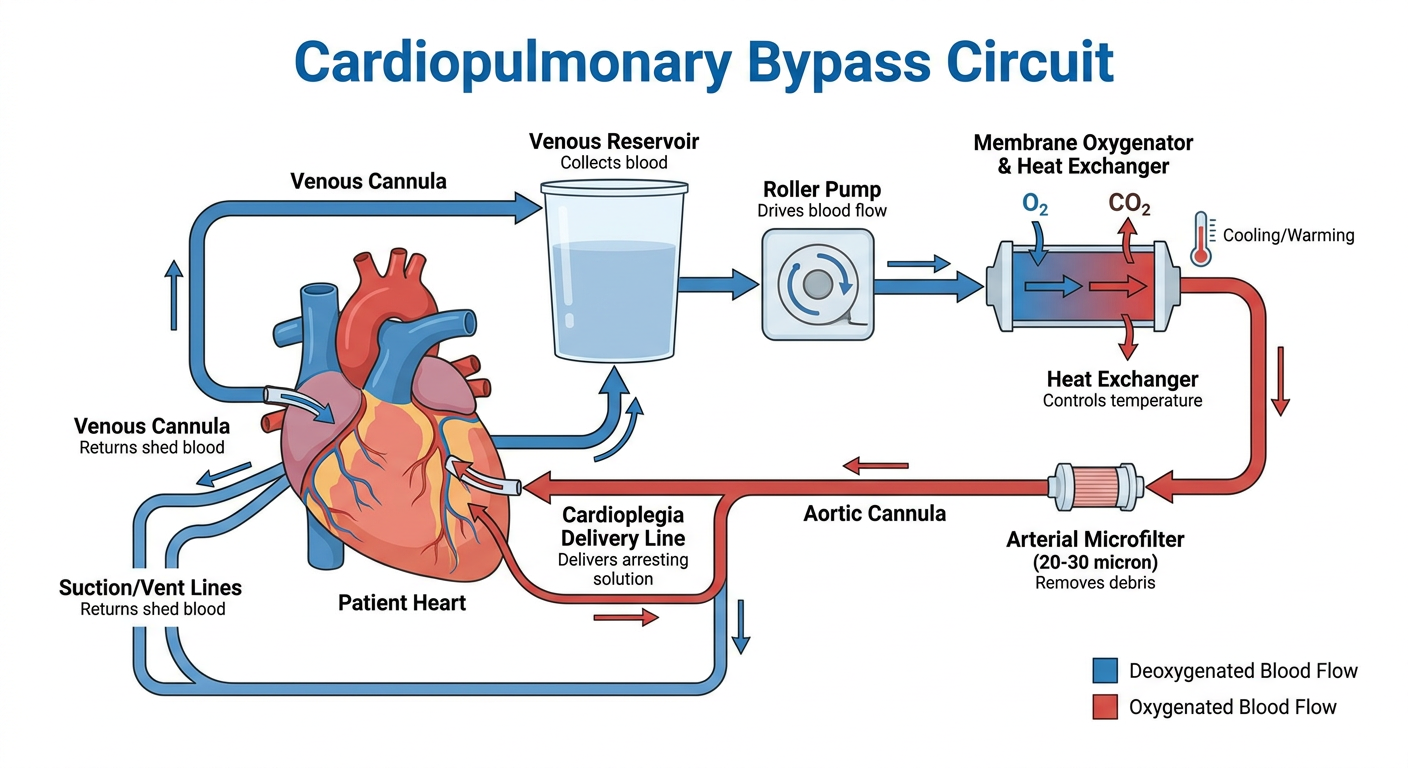
- Venous cannula in the right atrium / IVC
- Gravity siphon drainage to the venous reservoir
- Membrane oxygenator - gas exchange (O2 in, CO2 out)
- Heat exchanger - cools blood to reduce metabolic demand or rewarms at end of bypass
- Roller pump - drives blood back to the patient
- Arterial microfilter (20-30 µm) - removes micro-emboli and debris
- Aortic cannula returning blood to the ascending aorta
- Cardioplegia delivery line to coronary ostia (arrests the heart in diastole)
- Suction/vent lines recovering blood from the operative field back to the reservoir