Define RCT
A Randomized Controlled Trial (RCT) is a study design where participants are randomly assigned to either an intervention group (receives the treatment being tested) or a control group (receives a placebo, standard care, or no treatment). Random assignment minimizes selection bias and confounding, making RCTs the gold standard for establishing cause-and-effect relationships in clinical research.
Key features:
- Randomization - participants are allocated by chance, balancing known and unknown confounders
- Control group - provides a baseline for comparison
- Blinding - single-blind (participant unaware) or double-blind (both participant and investigator unaware) reduces measurement bias
- Prospective - participants are followed forward in time after the intervention
Why it matters:
RCTs sit at the top of the evidence hierarchy for evaluating treatment efficacy and safety. They are required by regulatory agencies (e.g., FDA, EMA) before approving most new drugs or devices.
Limitations:
- Expensive and time-consuming
- May have strict inclusion/exclusion criteria, limiting generalizability (external validity)
- Ethical constraints may prevent randomization in some scenarios (e.g., you cannot randomize someone to smoke)
- Short follow-up periods may miss long-term effects
In short, an RCT answers: "Does this intervention work, compared to not having it?" - under controlled conditions.
Root canal treatment
Reading File
Finding Sources
Searching the Web
root canal treatment procedure steps indications 2024
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Here is a comprehensive overview of Root Canal Treatment (RCT):
Root Canal Treatment (Endodontic Treatment)
What Is It?
Root canal treatment (RCT), also called endodontic treatment, is a dental procedure in which the pulp - the soft tissue inside the tooth containing nerves, blood vessels, and connective tissue - is removed, the root canals are cleaned, shaped, and disinfected, and then filled and sealed. The goal is to eliminate infection and save the natural tooth from extraction.
Relevant Anatomy
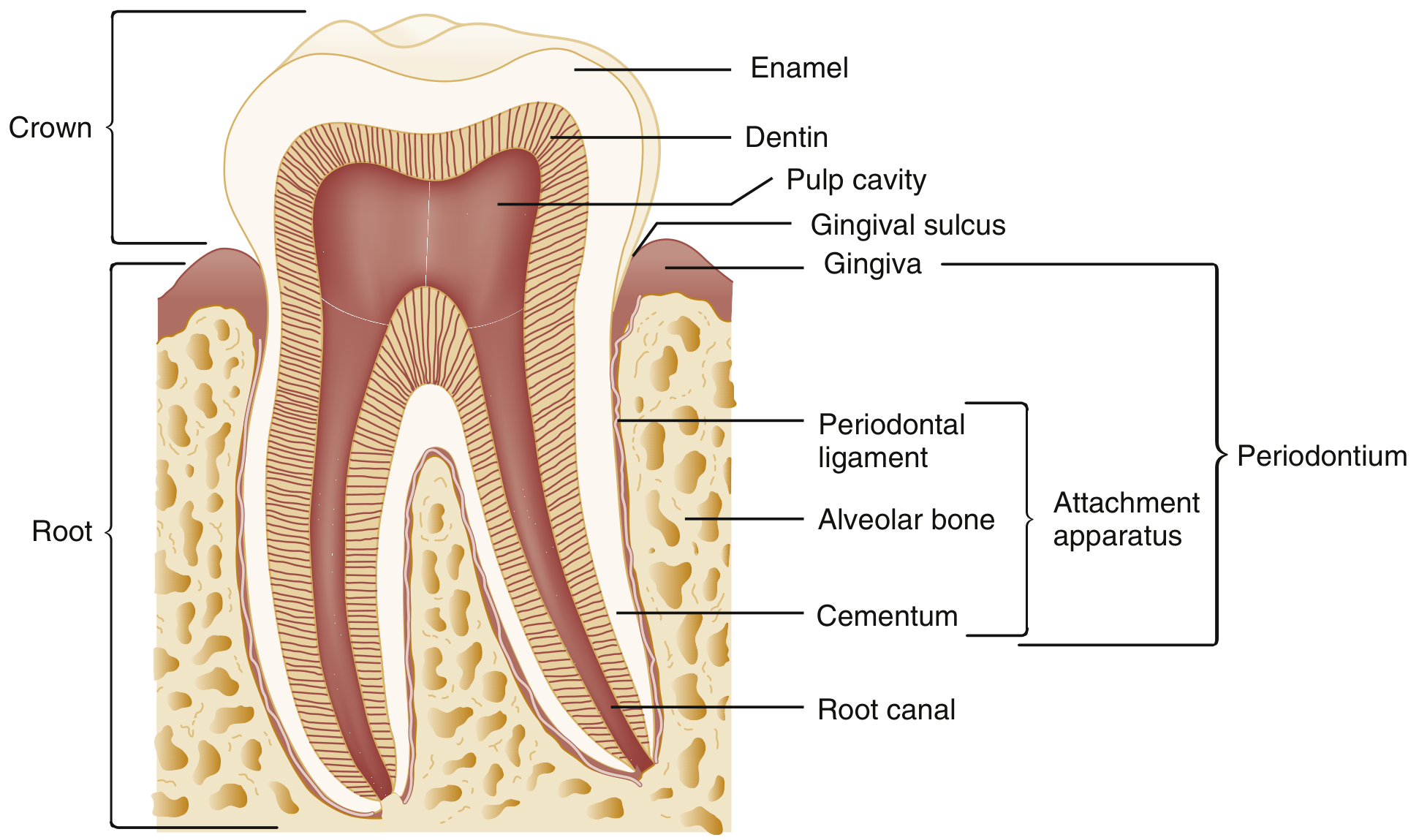
As shown in the diagram above:
- Crown - the visible part of the tooth, covered by enamel
- Dentin - the layer beneath enamel; microporous, can transmit bacteria and their byproducts to the pulp
- Pulp cavity / Root canal - the hollow space running through the crown and root, housing the dental pulp
- Apical foramen - the opening at the root tip, where nerves and blood vessels enter/exit
- Periodontal ligament, alveolar bone, cementum - the attachment apparatus anchoring the tooth in the jaw
Why It Is Needed - Pathological Progression
As explained in Rosen's Emergency Medicine:
- Dental caries - bacteria (primarily Streptococcus mutans, then lactobacilli) produce acid that demineralizes enamel and penetrates dentin
- Reversible pulpitis - early inflammation; pulp reacts with hyperemia; pain triggered by temperature/pressure changes, which resolves with stimulus removal
- Irreversible pulpitis - continued bacterial invasion; pulp cannot repair itself; pain becomes spontaneous, dull, throbbing, and persistent - even without any stimulus
- Pulp necrosis - total degeneration of pulp tissue; an anaerobic bacterial biofilm colonizes the necrotic root canals
- Apical periodontitis / Periapical abscess - infection spreads beyond the root tip (apical foramen) into periapical tissues, causing tenderness on percussion, swelling, and suppuration
As Scott-Brown's Otorhinolaryngology notes, chronic spread leads to a periapical granuloma - a well-circumscribed radiolucency visible on X-ray at the root apex, often asymptomatic.
Indications for RCT
- Irreversible pulpitis (spontaneous, severe, or persistent tooth pain)
- Pulp necrosis
- Periapical abscess or periodontitis
- Deep carious lesion with pulp exposure
- Tooth fracture reaching the pulp
- Before placing a crown over a severely compromised tooth
Alternative: Tooth extraction - but RCT is preferred to preserve the natural tooth.
Procedure - Step by Step
| Step | What Happens |
|---|---|
| 1. Diagnosis | Clinical exam + periapical X-ray to confirm pulp involvement |
| 2. Anesthesia | Local anesthetic to numb the tooth |
| 3. Isolation | Rubber dam placed to keep the field dry and sterile |
| 4. Access opening | A hole is drilled through the crown to reach the pulp chamber |
| 5. Pulp removal | Infected/necrotic pulp is removed with endodontic files |
| 6. Canal shaping | Root canals are mechanically shaped using sequential files |
| 7. Irrigation | Canals flushed (typically with sodium hypochlorite) to disinfect |
| 8. Medication | Calcium hydroxide or antimicrobial paste may be placed between visits for severely infected teeth |
| 9. Obturation | Canals are filled with gutta-percha (a rubber-like material) and sealer |
| 10. Restoration | The crown opening is sealed; a dental crown is usually placed afterward to restore function and prevent fracture |
If infection is severe, the tooth may be left open to drain for 1-2 days before the canal is sealed, requiring a second appointment.
Key Points on Antibiotics
As noted in Scott-Brown's Otorhinolaryngology: systemic antibiotics are NOT routinely prescribed for pulpitis or apical periodontitis. Antibiotics are reserved for spreading infections or severe cases requiring hospital admission. The definitive treatment is surgical - drainage, root canal, or extraction.
Complications of Untreated Pulp Infection
- Periapical abscess with facial swelling
- Spread to deep neck spaces (Ludwig's angina - a life-threatening emergency)
- Osteomyelitis of the jaw
- Cavernous sinus thrombosis (rare)
- As Dermatology 2-Volume Set notes: odontogenic infections can present with skin manifestations requiring incision, drainage, and endodontic therapy or extraction
Prognosis
RCT has an excellent long-term success rate (>90% at 8-10 years) when properly performed and restored with a crown. The treated tooth has no living pulp but remains functional within the jaw, supported by the periodontal ligament and alveolar bone.
Sources: Rosen's Emergency Medicine; Scott-Brown's Otorhinolaryngology, Head & Neck Surgery; Histology: A Text and Atlas; Tintinalli's Emergency Medicine; Harrison's Principles of Internal Medicine 22e
Make it for 5 mark questions
Root Canal Treatment (RCT)
Definition:
Root canal treatment (endodontic treatment) is a dental procedure in which the infected or necrotic pulp is removed from the pulp chamber and root canals, followed by cleaning, shaping, and obturation of the canals to eliminate infection and save the tooth from extraction.
Indications
- Irreversible pulpitis
- Pulp necrosis
- Periapical abscess / apical periodontitis
- Deep carious lesion with pulp exposure
- Tooth fracture extending to the pulp
Steps of RCT
- Diagnosis - Clinical exam + periapical X-ray
- Local anesthesia and rubber dam isolation
- Access cavity preparation through the crown
- Pulp extirpation using endodontic files
- Canal shaping and irrigation (sodium hypochlorite)
- Obturation - filling with gutta-percha and sealer
- Restoration - permanent filling or crown placement
Pathological Basis
Bacteria breach enamel → invade dentin → reach pulp → reversible pulpitis → irreversible pulpitis (spontaneous, persistent pain) → pulp necrosis → periapical infection via apical foramen.
Key Points
- Antibiotics are NOT routinely prescribed; RCT/extraction is the definitive treatment
- A crown is placed post-RCT to prevent tooth fracture
- Success rate: >90% at 10 years
Make it for 10 mark
Root Canal Treatment (RCT) / Endodontic Treatment
Definition
Root canal treatment (RCT), also called endodontic treatment, is a dental procedure in which the infected, inflamed, or necrotic pulp tissue is removed from the pulp chamber and root canals, followed by thorough cleaning, shaping, disinfection, and three-dimensional obturation of the canal system, to eliminate infection and preserve the natural tooth.
Relevant Anatomy
A tooth consists of:
- Enamel - outermost hard layer covering the crown
- Dentin - microporous layer beneath enamel; transmits bacteria and their byproducts to the pulp
- Pulp cavity - contains the dental pulp (nerves, blood vessels, connective tissue)
- Root canal - the channel running through the root, continuous with the pulp cavity
- Apical foramen - opening at the root tip; entry/exit point for neurovascular supply
- Periodontal ligament + alveolar bone + cementum - the attachment apparatus anchoring the tooth
Etiology and Pathological Basis
The most common cause is dental caries (tooth decay). Other causes include tooth fracture and retrograde infection via the apical foramen.
Progression of disease:
| Stage | Features |
|---|---|
| Dental caries | S. mutans and lactobacilli produce acid → enamel demineralization → dentin invasion |
| Reversible pulpitis | Hyperemic pulp response; pain on hot/cold stimuli that resolves on removal |
| Irreversible pulpitis | Pulp unable to repair; spontaneous, dull, throbbing, persistent pain even without stimulus |
| Pulp necrosis | Total pulp degeneration; anaerobic biofilm colonizes root canal walls |
| Apical periodontitis | Infection spreads through apical foramen into periapical tissues; tenderness on percussion |
| Periapical abscess | Frank pus formation; pain, swelling, erythema, suppuration around the affected tooth |
| Periapical granuloma | Chronic host response (T cells + macrophages); asymptomatic; seen as radiolucency on X-ray |
Indications for RCT
- Irreversible pulpitis
- Pulp necrosis
- Periapical abscess / apical periodontitis
- Deep carious lesion with pulp exposure
- Tooth fracture reaching the pulp
- Heavily compromised tooth requiring crown placement
- Symptomatic tooth that fails to respond to conservative management
Contraindication to RCT: Unrestorable tooth - extraction is preferred.
Clinical Features Suggesting Need for RCT
- Spontaneous, severe, persistent toothache (irreversible pulpitis)
- Pain worse on lying down
- Tenderness on percussion of the tooth (periapical involvement)
- Facial swelling or sinus tract (abscess)
- Well-circumscribed periapical radiolucency on X-ray (granuloma/cyst)
- Non-response to analgesics
Procedure - Step by Step
Step 1 - Diagnosis
- Clinical examination + periapical radiograph
- Vitality testing (cold/electric pulp test)
- Percussion and palpation
Step 2 - Anesthesia and Isolation
- Local anesthetic (e.g., lidocaine with epinephrine)
- Rubber dam placed to maintain a sterile, dry operating field
Step 3 - Access Cavity Preparation
- A hole is drilled through the crown to reach the pulp chamber
- Roof of the pulp chamber is removed to gain straight-line access to canals
Step 4 - Working Length Determination
- Electronic apex locator and/or periapical X-ray to determine the exact length of each root canal
Step 5 - Pulp Extirpation and Canal Shaping
- Infected/necrotic pulp removed using endodontic files (hand/rotary)
- Canals progressively shaped in a crown-down technique
Step 6 - Irrigation and Disinfection
- Copious irrigation with sodium hypochlorite (NaOCl) - main irrigant
- EDTA used to remove the smear layer
- Final rinse with chlorhexidine or saline
Step 7 - Inter-appointment Medication (if needed)
- Calcium hydroxide paste placed in canals between visits for severely infected teeth
- Tooth may be left open to drain for 1-2 days if infection is severe
Step 8 - Obturation
- Canals dried with paper points
- Filled with gutta-percha cones + root canal sealer (e.g., zinc oxide eugenol)
- Lateral condensation or warm vertical compaction technique
Step 9 - Coronal Restoration
- Temporary or permanent filling placed
- A dental crown is strongly recommended to restore function and prevent fracture of the brittle, non-vital tooth
Post-operative Care
- Mild pain and sensitivity for a few days - managed with NSAIDs (ibuprofen)
- Avoid chewing on the treated tooth until crown is placed
- Follow-up X-ray at 6-12 months to confirm periapical healing
Role of Antibiotics
Antibiotics are NOT routinely prescribed for pulpitis or localized periapical abscess. They are reserved for:
- Spreading infections (cellulitis, fascial space involvement)
- Systemic signs (fever, trismus, lymphadenopathy)
- Immunocompromised patients
Definitive treatment is always surgical - RCT or extraction.
Complications of Untreated Pulp Infection
- Periapical cyst
- Osteomyelitis of the jaw
- Deep neck space infections (e.g., Ludwig's angina - life-threatening)
- Cavernous sinus thrombosis (rare)
- Bacteremia and systemic spread in susceptible individuals
Complications of RCT Itself
- Instrument fracture inside canal
- Ledging or perforation of root
- Underfilling or overfilling
- Missed canals
- Post-operative flare-up
- Reinfection requiring retreatment or apicoectomy
Prognosis
- Success rate: >90% at 8-10 years when properly performed and restored
- Key factors for success: complete canal debridement, tight obturation, and good coronal seal
- Failed RCT can be retreated endodontically or managed with periapical surgery (apicoectomy)
Sources: Rosen's Emergency Medicine; Scott-Brown's Otorhinolaryngology, Head & Neck Surgery; Histology: A Text and Atlas (Pawlina); Tintinalli's Emergency Medicine; Harrison's Principles of Internal Medicine 22e
Sort note on PTA
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
I have all the content needed for a well-structured short note.
Short Note on Peritonsillar Abscess (PTA) / Quinsy
Definition
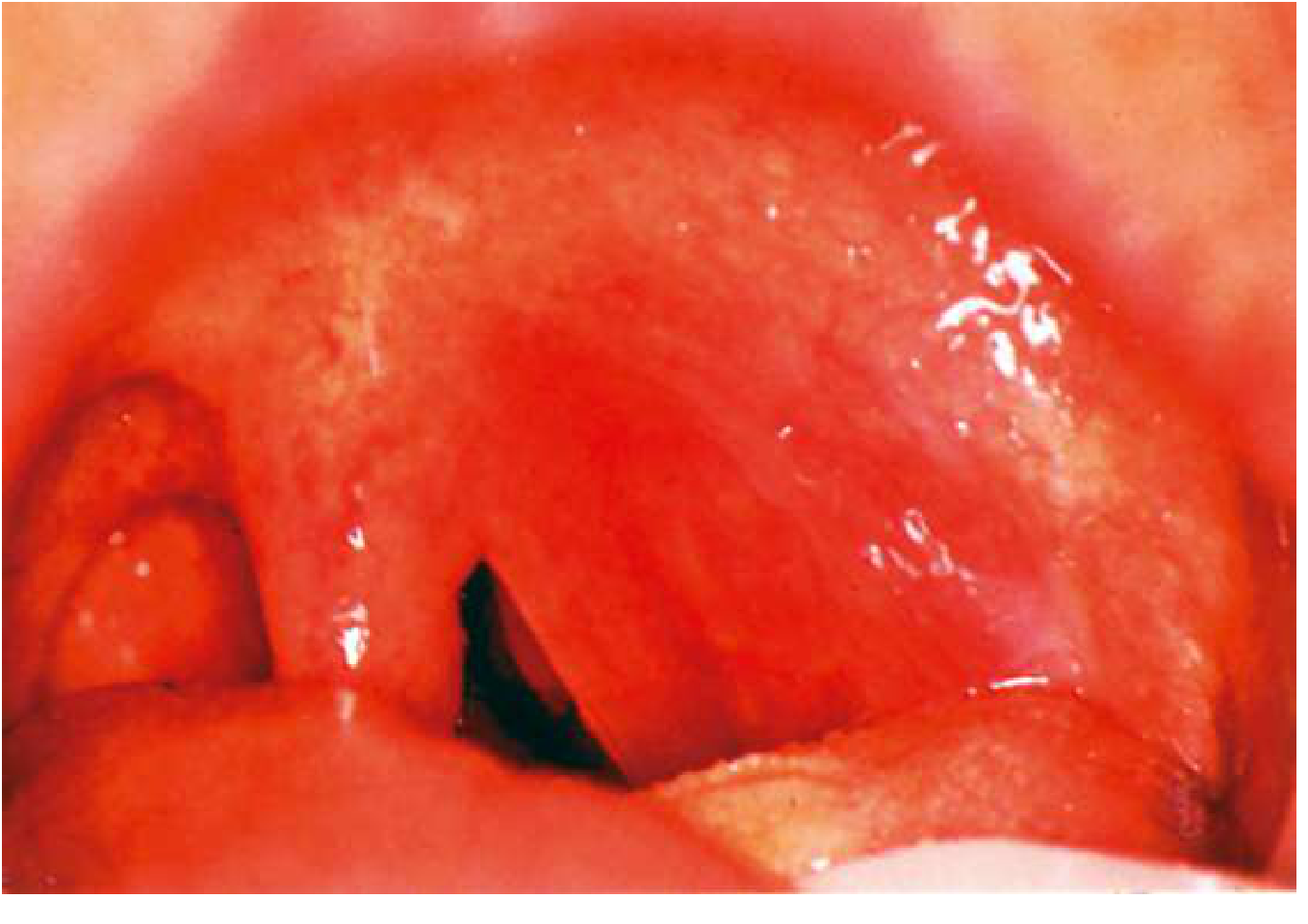
A peritonsillar abscess (PTA), also called quinsy, is a collection of pus in the peritonsillar space - between the palatine tonsillar capsule and the superior pharyngeal constrictor muscle. It is the most common deep neck space infection.
Anatomy of the Space
- Pus collects in the potential space between the tonsillar capsule and the superior constrictor/palatopharyngeus muscle
- Fibrous septa direct the infection anteriorly and superiorly
- Infection originates from the Weber glands (minor salivary glands in the superior pole)
Etiology / Microbiology
- Typically polymicrobial (mixed aerobic + anaerobic)
- Most common isolate: Streptococcus pyogenes (Group A Strep)
- Recurrent PTA: high incidence of Fusobacterium
- Preceded by: streptococcal tonsillitis, infectious mononucleosis, dental/periodontal disease, smoking
Clinical Features
| Symptom | Sign |
|---|---|
| Severe unilateral sore throat | Tense, erythematous, bulging anterior tonsillar pillar |
| Odynophagia / dysphagia | Uvula deviated to contralateral side |
| Trismus (best indicator) | Tonsillar + peritonsillar edema with exudate |
| Muffled / "hot potato" voice | Tender ipsilateral cervical lymphadenopathy |
| Ipsilateral otalgia (referred) | |
| Drooling, fever, malaise |
Trismus (inability to open mouth) is the hallmark - caused by spasm of the pterygoid muscles, distinguishing PTA from simple tonsillitis.
Diagnosis
- Primarily clinical - bulging anterior pillar + uvular deviation + trismus
- Needle aspiration - both diagnostic and therapeutic (confirms pus vs. cellulitis)
- CT neck with contrast - not routinely needed; indicated if clinical picture is unclear or deep space spread is suspected
Treatment
1. Drainage (mainstay)
- Needle aspiration - first choice; wide-bore needle at the point of maximal fluctuation (superior pole)
- Incision and Drainage (I&D) - if aspiration fails or recurrence
- Quinsy tonsillectomy (tonsillectomy during acute attack) - not popular due to risk of pus aspiration
2. Antibiotics
- IV high-dose penicillin or cephalosporin (first line)
- Alternatives: clindamycin (300-450 mg QID x 14 days) or amoxicillin-clavulanate (875 mg BD x 10 days)
- Metronidazole does NOT add benefit in otherwise healthy adults treated with I&D
3. Corticosteroids
- IV steroids as adjunct - reduce inflammation, pain, and trismus
4. Supportive
- Adequate hydration, analgesics, antipyretics
Interval Tonsillectomy
Recommended after:
- Two or more episodes of PTA on the same side
- Background history of recurrent tonsillitis
- Recurrence rate after first PTA: ~17%
Complications
- Rupture - spontaneous pus release into airway (aspiration risk)
- Parapharyngeal abscess - spread to parapharyngeal space; trismus + airway compromise
- Retropharyngeal abscess - posterior spread; mainly in children
- Deep neck space infection / Mediastinitis - life-threatening
- Lemierre's syndrome - septic thrombophlebitis of the internal jugular vein (rare but fatal); caused by Fusobacterium necrophorum; presents with fever, neck mass, septic pulmonary emboli
Sources: Scott-Brown's Otorhinolaryngology, Head & Neck Surgery; K.J. Lee's Essential Otolaryngology; Rosen's Emergency Medicine; Goldman-Cecil Medicine
Short note on pure tone audiometry
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Loading Image
I have comprehensive content from multiple ENT textbooks. Here is the complete short note:
Short Note on Pure Tone Audiometry (PTA)
Definition
Pure tone audiometry is a subjective, behavioural hearing test that measures an individual's hearing sensitivity thresholds to pure tones (sinusoidal signals with a single defined frequency and amplitude) across a range of frequencies important for human communication. Thresholds are plotted on an audiogram to determine the type, degree, and configuration of hearing loss.
Principle
- A pure tone is presented to the ear at varying intensity levels
- The threshold = the lowest intensity level at which the patient responds correctly at least 50% of the time
- Testing is done by air conduction (AC) and bone conduction (BC)
- Comparison of AC and BC thresholds determines the type of hearing loss
Equipment
- Audiometer - generates calibrated pure tones; types include screening, clinical, and diagnostic
- Earphones (supra-aural or insert) for air conduction
- Bone oscillator - placed on the mastoid process for bone conduction
- Sound-treated booth - required to measure thresholds as low as 0 dB HL
- Calibration must be done at least annually
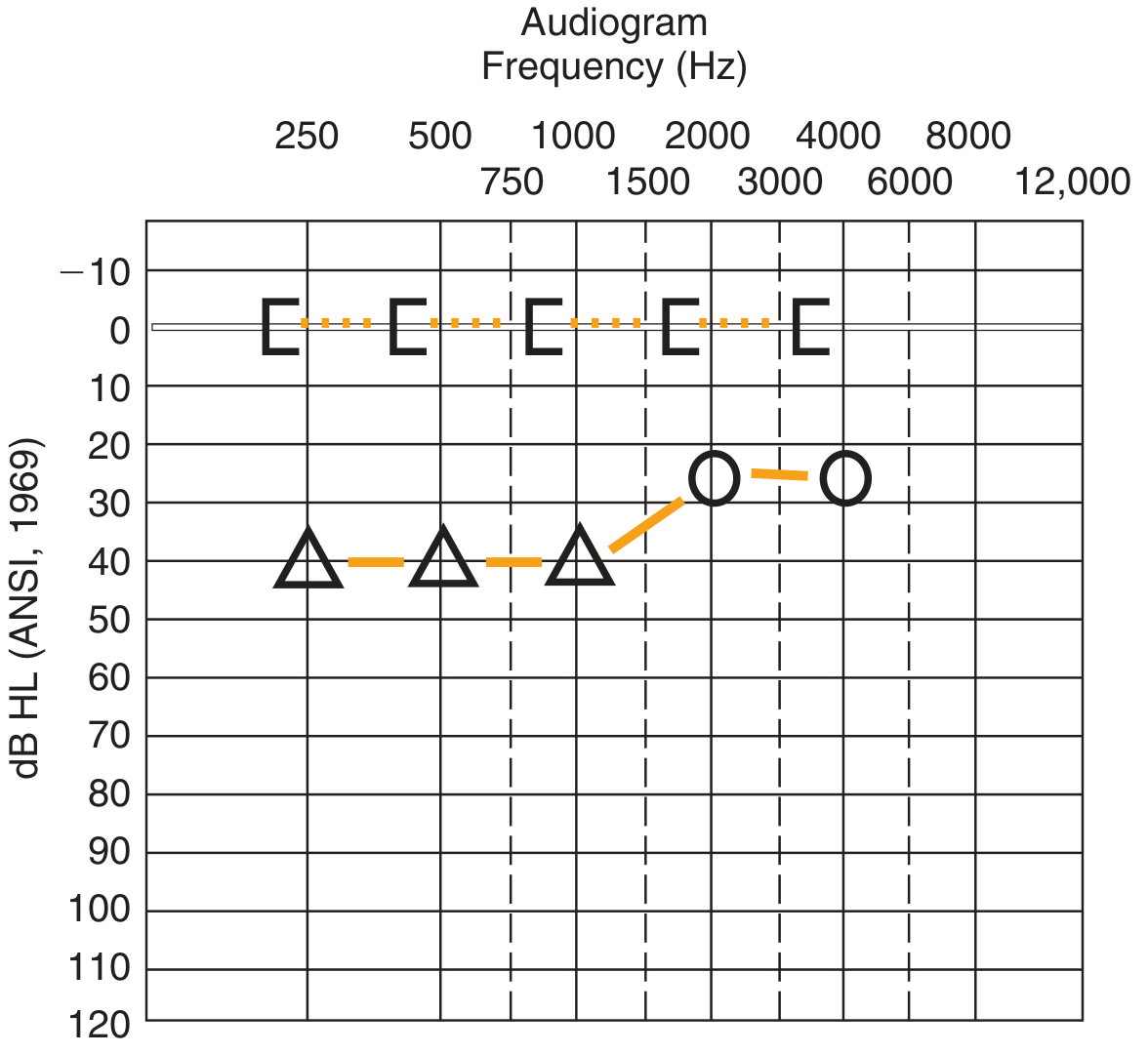
Audiogram - The Recording Chart
| Parameter | Detail |
|---|---|
| X-axis | Frequency in Hz (250, 500, 1000, 2000, 4000, 8000 Hz) |
| Y-axis | Hearing level in dB HL (0 at top; worse hearing going down) |
| 0 dB HL | Audiometric zero = average normal hearing |
| Right ear AC | Circle (O), red |
| Left ear AC | Cross (X), blue |
| Right ear BC (unmasked) | Right-facing bracket |
| Left ear BC (unmasked) | Left-facing bracket |
| Masked BC | Square brackets |
Inter-octave frequencies (e.g., 1500 Hz) are tested when there is a ≥25 dB difference between adjacent octave thresholds.
Procedure (Hughson-Westlake Method)
- Explain the test to the patient; conduct otoscopy first
- Present a tone well above threshold so patient knows what to listen for
- Decrease in 10 dB steps until no response
- Increase in 5 dB steps until response is obtained
- Threshold = level at which response is obtained on 3 out of 5 (≥50%) ascending trials
- Test AC first (250-8000 Hz), then BC if AC thresholds ≥15 dB HL
Masking
- Noise introduced into the non-test ear to prevent it from detecting signals intended for the test ear (called crossover)
- The spread of sound energy across the skull is called interaural attenuation
- AC with supra-aural headphones: 40-65 dB
- BC: only 0-10 dB (masking almost always needed for BC)
- Insert earphones: up to 70-90 dB (less crossover risk)
- Masker used: narrow-band noise centred around the test frequency
Grading of Hearing Loss (Shambaugh Classification)
| Threshold (dB HL) | Grade |
|---|---|
| 0-25 | Normal |
| 15-25 | Minimal |
| 25-40 | Mild |
| 40-55 | Moderate |
| 55-70 | Moderately severe |
| 70-90 | Severe |
| >90 | Profound |
Types of Hearing Loss on Audiogram
| Type | AC Threshold | BC Threshold | Air-Bone Gap |
|---|---|---|---|
| Normal | ≤25 dB | ≤25 dB | None |
| Conductive | Elevated | Normal | Present (>10 dB) |
| Sensorineural (SNHL) | Elevated | Elevated equally | Absent |
| Mixed | Elevated | Elevated (less than AC) | Present |
Air-Bone Gap = difference between AC and BC thresholds. Indicates a conductive component (outer/middle ear pathology).
Audiometric Configurations (Patterns of Loss)
- Flat - equal loss across all frequencies (e.g., otosclerosis)
- High-frequency sloping - worse at high frequencies (e.g., noise-induced, presbycusis)
- Low-frequency loss - worse at low frequencies (e.g., Meniere's disease - early)
- Cookie-bite / U-shaped - mid-frequency loss (hereditary causes)
- Notch at 4000 Hz - classic pattern in noise-induced hearing loss
Pure Tone Average (PTA)
PTA = average of AC thresholds at 500, 1000, 2000 Hz (speech frequencies).
Used for medico-legal purposes and hearing aid fitting.
Limitations
- Subjective - requires patient cooperation and reliable responses
- Not suitable for infants (<3 years) - alternative methods used:
- 0-6 months: Behavioral Observation Audiometry (BOA)
- 6 months - 2 years: Visual Reinforcement Audiometry (VRA)
- 2-5 years: Conditioned Play Audiometry (CPA)
- Cannot differentiate cochlear from retrocochlear SNHL - needs ABR/BERA
Clinical Significance
PTA is the foundation of the audiological evaluation. It:
- Quantifies degree and type of hearing loss
- Guides hearing aid selection and fitting
- Monitors ototoxicity (serial audiograms at 3000, 6000 Hz)
- Provides medico-legal documentation
- Cross-checks speech audiometry results
Sources: Cummings Otolaryngology Head and Neck Surgery; Scott-Brown's Otorhinolaryngology; K.J. Lee's Essential Otolaryngology; Shambaugh Surgery of the Ear
This is a shared conversation. Sign in to Orris to start your own chat.