Labour analgesia 30 mark Question for anaesthesia MD Exam
Reading File
Finding Sources
Finding Sources
Searching the Web
labour analgesia 30 marks anaesthesia MD exam question answer 2024
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
I now have comprehensive data from Miller's Anesthesia (10e) and Morgan & Mikhail. Let me compose the full 30-mark exam answer.
Labour Analgesia — 30-Mark Model Answer (Anaesthesia MD Examination)
Introduction
Labour pain is one of the most intense pains a human can experience. It arises from complex physiological mechanisms and carries significant maternal and fetal consequences when undertreated. Optimal labour analgesia reduces maternal catecholamine surges, prevents fetal hypoxia from hyperventilation-driven hypocapnia, and improves the birth experience without compromising labour progress or neonatal outcome. (Miller's Anesthesia, 10e)
1. Physiology and Pathways of Labour Pain (5 marks)
First Stage of Labour
- Pain is visceral in origin - from uterine contractions, cervical dilation, and lower uterine segment distension.
- Afferent impulses travel via the uterine and cervical plexuses through sympathetic nerves, entering the spinal cord at T10-L1.
- Character: crampy, poorly localised, referred to the umbilicus, lower abdomen, and lumbar region.
Second Stage of Labour
- Pain becomes somatic as the presenting part descends and distends the vagina, perineum, and pelvic floor.
- Afferent impulses travel via the pudendal nerve (S2-S4) and posterior cutaneous nerve of the thigh.
- Sensory block must extend from T10 to S4 to cover both stages.
Physiological Consequences of Untreated Labour Pain
| System | Effect |
|---|---|
| Respiratory | Minute ventilation increases up to 300%; PaCO2 may fall below 20 mmHg, causing fetal hypoxia between contractions |
| Cardiovascular | Cardiac output rises 45% above third-trimester values per contraction; surges to 80% above baseline immediately postpartum |
| Neuroendocrine | Catecholamine surge causes uterine vasoconstriction, reduced uteroplacental perfusion, fetal acidosis |
| Uterine | Extreme hyperventilation reduces uterine blood flow and promotes fetal acidosis |
(Morgan & Mikhail, 7e; Miller's Anesthesia, 10e)
2. Non-Pharmacological Methods (3 marks)
These are safe, widely available, and do not affect the fetus. They are often used as adjuncts or first-line measures in mild pain:
- Breathing techniques - Lamaze, Bradley method, LeBoyer technique
- Continuous labour support - doula or partner presence; Cochrane review of 26 trials (n=15,858) showed shorter labour, more spontaneous vaginal deliveries, less pharmacological analgesia
- Hydrotherapy (water immersion / warm bath)
- TENS (Transcutaneous Electrical Nerve Stimulation) - stimulates Aβ fibres, activates gate control mechanism
- Acupuncture/acupressure - Cochrane review of 28 RCTs (n=3,960): acupuncture minimally reduces labour pain and increases maternal satisfaction; acupressure showed no clear benefit over sham
- Massage - Cochrane review of 10 RCTs: reduces pain in first stage; increases sense of control
- Hypnosis - Cochrane review of 9 trials (n=2,954): reduced systemic analgesia use; no clear difference in neuraxial use
- Intradermal sterile water injections, aromatherapy, biofeedback
(Miller's Anesthesia, 10e)
3. Pharmacological Methods
3a. Systemic Analgesics (4 marks)
Opioids
All opioids cross the placenta readily and can cause fetal respiratory depression, decreased FHR variability, and neonatal respiratory depression.
| Drug | Route | Dose | Notes |
|---|---|---|---|
| Meperidine (Pethidine) | IV / IM | 50 mg IV; 50–100 mg IM | Historically most used; active metabolite normeperidine half-life 13–23h (3x longer in fetus); lower Apgar scores; now rarely used |
| Morphine | IM | Latent labour | Significant sedation; active metabolite M6G prolonged in neonate |
| Fentanyl | IV PCA | 25–50 mcg bolus | Short-acting; better side effect profile; can cause transient FHR changes |
| Remifentanil | IV PCA | 20–40 mcg bolus | Ultra-short-acting; most suitable systemic opioid for PCA; risk of maternal apnoea - 1:1 nurse monitoring mandatory |
| Nalbuphine | IV/IM/SC | 10–20 mg q4-6h | Mixed agonist-antagonist; analgesic potency similar to morphine |
| Butorphanol | IV/IM | 1–2 mg | 5x more potent than morphine; 40x more than meperidine |
Remifentanil PCA has emerged as the best systemic opioid option. A BMJ 2015 RCT showed it was equivalent to epidural analgesia in some settings, but requires continuous 1:1 nursing monitoring due to risk of maternal apnoea.
Non-opioid Systemic Agents
- Nitrous oxide (Entonox - 50% N2O + 50% O2) - self-administered via facemask at onset of contraction; rapid onset/offset; minimal uterine effects; provides mild-moderate analgesia; safe for fetus; widely used in the UK
- Low-dose ketamine (10–15 mg IV) - excellent analgesia in 2–5 min without loss of consciousness; most useful just prior to delivery or as adjuvant to regional; doses >1 mg/kg cause hypertonic uterine contractions
- Midazolam (≤2 mg IV) - anxiolytic adjunct to neuraxial blockade; chronic diazepam use associated with fetal depression
- NSAIDs - avoid in labour (premature closure of ductus arteriosus)
(Morgan & Mikhail, 7e; Miller's Anesthesia, 10e)
3b. Regional (Neuraxial) Techniques (12 marks)
Regional neuraxial analgesia is the gold standard for labour pain management. The combination of a local anaesthetic (LA) and an opioid produces synergy, reducing dose requirements of both agents while minimising side effects.
"Using a local anaesthetic-opioid mixture for lumbar epidural analgesia during labor significantly reduces drug requirements when compared with using either agent alone." - Morgan & Mikhail, 7e
I. Epidural Analgesia
Most versatile technique - can be used for first stage, second stage, and converted to surgical anaesthesia for instrumental delivery or caesarean section.
Technique:
- Patient positioned sitting or left lateral; sterile technique
- Identify L3-L4 or L2-L3 interspace; loss of resistance technique (saline or air) for epidural space identification
- Test dose - 3 mL of 1.5% lidocaine + epinephrine 1:200,000; wait 5 minutes
- Tachycardia (+20-30 bpm) = intravascular placement
- Rapid dense motor/sensory block = intrathecal placement
- If test dose negative: administer 10-15 mL of LA-opioid mixture in 5 mL increments
- Place supine with left uterine displacement; monitor BP every 1-2 min for 15 min
Drug choices (dilute LA + opioid):
- Bupivacaine 0.0625–0.1% + fentanyl 2 mcg/mL
- Ropivacaine 0.1% + fentanyl 2 mcg/mL (less motor block, safer cardiac profile than bupivacaine)
- Bupivacaine 0.125% + sufentanil 0.5–1 mcg/mL
Sensory levels required:
- First stage: T10–L1
- Second stage: T10–S4
Administration modes:
| Mode | Description | Advantage |
|---|---|---|
| Continuous Epidural Infusion (CEI) | Steady infusion | Stable block level |
| PCEA (Patient-Controlled Epidural Analgesia) | Patient self-delivers bolus | Reduced LA consumption, less motor block |
| PIEB (Programmed Intermittent Epidural Bolus) | Automated boluses at intervals | Better spread, less breakthrough pain; meta-analysis of 27 studies (n=3,133) showed reduced breakthrough pain, improved maternal satisfaction, decreased motor block |
| PCEA + PIEB | Combined | Best overall control |
Effect on labour progress: Dilute LA-opioid mixtures do NOT prolong labour or increase operative delivery rate (Morgan & Mikhail, 7e; well-established evidence)
Adjuvants: Dexmedetomidine (α2-agonist, not FDA-approved neuraxially in the US) has been shown to be efficacious adjunct to epidural bupivacaine/ropivacaine for labour analgesia.
II. Combined Spinal-Epidural (CSE) Analgesia
Best for: Severe pain early in labour; patients close to delivery; rapid onset required.
Technique (Needle-through-Needle):
- Epidural needle placed in epidural space as standard
- Spinal needle (25G Whitacre or Sprotte pencil-point) passed through epidural needle until dural puncture confirmed by CSF
- Intrathecal injection of opioid ± low-dose LA
- Spinal needle withdrawn; epidural catheter threaded and secured
Intrathecal drugs:
- Fentanyl 15–25 mcg (opioid alone - no motor block; "walking epidural")
- Sufentanil 5–7.5 mcg
- Bupivacaine 2.5 mg + fentanyl 15 mcg (excellent initial analgesia)
Advantages of CSE over standard epidural:
- Faster onset (2–5 minutes vs 20 min for epidural)
- Dense analgesia; particularly useful for advanced labour
- Low-dose intrathecal component preserves ambulation ("walking epidural")
- Epidural catheter allows top-up for prolonged labour or operative delivery
Caution: Epidural catheter remains untested initially; drug spread from dural hole may potentiate epidural doses.
III. Spinal (Intrathecal) Analgesia
- Single-shot intrathecal opioid ± LA
- Provides rapid but time-limited analgesia (1.5–3 hours)
- "Saddle block" - hyperbaric tetracaine 3–4 mg or bupivacaine 2.5–5 mg + fentanyl 12.5–25 mcg for second stage/operative vaginal delivery
- Continuous spinal analgesia via intrathecal catheter: used after accidental dural puncture; provides excellent analgesia and utilises the wet tap
IV. Other Regional Techniques
Pudendal Nerve Block:
- Blocks S2-S4 (pudendal nerve), covering perineum/vaginal outlet
- Technique: transvaginal injection beneath ischial spine through sacrospinous ligament, using Koback needle/Iowa trumpet guide; 10 mL of 1% lidocaine or 2% chloroprocaine per side
- Useful for second stage and perineal repair
- Complications: intravascular injection, retroperitoneal haematoma, retropsoas/subgluteal abscess
Paracervical Block:
- Injections at 4 o'clock and 10 o'clock lateral to cervix
- Controls first-stage pain only
- No longer used for viable fetuses - high rate of transient fetal bradycardia (uterine artery proximity, direct fetal drug absorption); risk of injecting into fetal head
- Still used for intrauterine fetal demise, D&C, D&E procedures
4. Complications of Neuraxial Analgesia (4 marks)
| Complication | Incidence | Management |
|---|---|---|
| Hypotension (systolic <100 mmHg or >20% drop) | Most common | Phenylephrine 40–120 mcg IV bolus (first choice); ephedrine if bradycardia; left uterine displacement; IV fluid bolus; supplemental O2 |
| Inadvertent intravascular injection | Epidural catheter misplacement 5–15% | Epinephrine test dose; slow incremental dosing ≤5 mL; stop injection at first CNS signs (tinnitus, metallic taste, circumoral numbness) |
| Total spinal / High spinal | Inadvertent intrathecal injection | ABCDE resuscitation; RSI and intubation; vasopressors; left lateral tilt |
| Post-dural Puncture Headache (PDPH) | 0.5–2.5% | Conservative (caffeine, hydration, analgesics); epidural blood patch (gold standard) if not settling in 24-48h |
| Epidural haematoma | Rare | Avoid in coagulopathy; urgent MRI; neurosurgical decompression |
| Epidural abscess | Rare | Strict asepsis; IV antibiotics; surgical drainage |
| Fever/pyrexia | Epidural-associated fever | Acetaminophen; fever workup to exclude sepsis; neonatal sepsis workup if fever ≥38°C |
| Pruritus | Opioid-related | Naloxone 40–80 mcg IV (small doses); nalbuphine; ondansetron |
| Urinary retention | Common | Bladder catheterisation if needed |
| Motor block | LA dose-dependent | Use dilute LA solutions; PCEA/PIEB |
| Fetal bradycardia | CSE - transient | Usually resolves; repositioning; tocolysis (terbutaline) if persistent; prepare for emergency LSCS |
5. Effect on Labour and the Neonate (2 marks)
- Labour progress: Dilute LA-opioid combinations do NOT prolong labour or increase operative (caesarean or instrumental) delivery rates - this is a Class A evidence finding (Morgan & Mikhail, 7e)
- Fetus/Neonate: Neuraxial analgesia is vastly superior to systemic opioids for fetal safety; systemic opioids (especially meperidine/morphine) cross placenta and cause neonatal respiratory depression, lower Apgar scores, and neurobehavioural depression; neuraxial drugs - being highly dilute - have minimal neonatal effects
- Maternal catecholamines: Effective analgesia reduces catecholamines, improving uteroplacental perfusion
6. Contraindications to Neuraxial Analgesia
| Absolute | Relative |
|---|---|
| Patient refusal | Systemic infection/sepsis |
| Coagulopathy (INR >1.5, platelets <80,000) | Pre-existing neurological disease |
| Infection at injection site | Severe aortic/mitral stenosis |
| Hypovolaemic shock | Pharmacological anticoagulation |
| Raised intracranial pressure (mass effect) | Platelet 80,000-100,000 (individualised) |
| Inadequate expertise/resources | Uncorrected hypovolaemia |
Summary Table
| Technique | Level Blocked | Onset | Duration | Best For |
|---|---|---|---|---|
| Epidural (continuous) | T10–S4 | 20 min | Indefinite | Full labour + LSCS conversion |
| CSE | T10–S4 | 2–5 min | Indefinite (epidural) | Severe early pain; near delivery |
| Single-shot spinal | Saddle (S2–S5) | 3–5 min | 1.5–3 h | Second stage, instrumental delivery |
| Pudendal nerve block | S2–S4 | 5–10 min | 1–2 h | Perineal pain, second stage |
| IV Remifentanil PCA | Systemic | Immediate | Continuous | Neuraxial refused/contraindicated |
| Entonox (N2O/O2) | Systemic | 30–60 sec | Minutes | Mild-moderate, bridging |
Conclusion
Continuous lumbar epidural analgesia remains the most versatile, effective, and commonly used technique for labour pain, combining a dilute local anaesthetic with an opioid administered via PCEA or PIEB. The CSE technique combines the advantages of rapid spinal onset with epidural flexibility. Non-pharmacological methods are valuable adjuncts or alternatives for women preferring to avoid pharmacological intervention. The key clinical principle is that adequate labour analgesia, when properly administered, improves maternal well-being, optimises uteroplacental perfusion, does not adversely affect labour progress, and is not associated with increased operative delivery rates.
Sources:
- Miller's Anesthesia, 2-Volume Set, 10th Edition (Elsevier, 2023)
- Morgan & Mikhail's Clinical Anesthesiology, 7th Edition (McGraw Hill, 2022)
- Barash, Cullen & Stoelting's Clinical Anesthesia, 9th Edition
Anaesthesia for awake craniotomy
Reading File
Finding Sources
Finding Sources
Searching the Web
awake craniotomy anaesthesia technique asleep awake asleep dexmedetomidine 2024
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Loading Image
Finding Sources
Excellent - I now have comprehensive content from both textbooks plus the scalp nerve diagram. Let me compile the complete answer:
Anaesthesia for Awake Craniotomy — Comprehensive MD Exam Answer
1. Introduction and Rationale
Awake craniotomy is a neurosurgical procedure performed under monitored anaesthesia care (MAC) that allows intraoperative neurological testing while the patient remains conscious during the critical mapping phase. It has gained increasing popularity worldwide as it permits real-time cortical and subcortical mapping, enabling surgeons to resect tumours or epileptic foci more aggressively while minimising the risk of permanent neurological deficit.
The central principle is: the brain parenchyma is insensate - pain arises only from the scalp, pericranium, dura, and vascular structures. A well-executed scalp nerve block, therefore, is the cornerstone of the technique; sedation cannot substitute for inadequate local anaesthesia.
(Miller's Anesthesia, 10e)
2. Indications
| Indication | Rationale |
|---|---|
| Tumours adjacent to eloquent cortex (primary motor/sensory, speech/language areas) | Allows real-time motor or speech mapping for safe maximal resection |
| Epilepsy surgery (temporal lobe epilepsy, cortical dysplasia) | Electrocorticography (ECoG), seizure focus localisation |
| Tumours near mesial temporal structures | Short-term memory mapping; Wada test alternatives |
| Arteriovenous malformations (AVMs) near eloquent cortex | Functional mapping before occlusion |
| Deep brain stimulation (DBS) electrode placement | Microelectrode recording and clinical response assessment |
| Stereotactic biopsy of eloquent regions | Neurological monitoring |
Awake craniotomy is particularly indicated when the tumour lies within or adjacent to Broca's area (inferior frontal gyrus, dominant hemisphere), Wernicke's area (posterior temporal gyrus), or the primary motor strip - where general anaesthesia-based monitoring techniques cannot assess language function. (Miller's Anesthesia, 10e; Barash, 9e)
3. Presurgical Evaluation
Preoperative Neurological Workup
Before surgery, most patients undergo:
- Wada test (intracarotid sodium amobarbital test) - selective hemisphere anaesthesia to lateralise speech dominance and test bilateral memory representation
- Video-telemetry with EEG electrode placement - for epilepsy surgery, to record and localise ictal events
- Functional MRI (fMRI) / PET scan - non-invasive cortical mapping
- Neuropsychological baseline assessment - establishes cognitive/language function for intraoperative comparison
(Miller's Anesthesia, 10e)
Patient Selection Criteria
Ideal candidate:
- Motivated, cooperative, psychologically prepared patient
- Able to follow commands and communicate during testing
- No severe anxiety, claustrophobia, or panic disorder
- No obstructive sleep apnoea (high sedation risk with prone/lateral positions)
- No significant language barrier
- No uncontrolled cough, nausea, or movement disorders
Contraindications:
- Severe anxiety or inability to cooperate (relative)
- Morbid obesity (airway management challenges with inaccessible airway)
- Obstructive sleep apnoea
- Uncontrolled cough or movement disorder
- Severe nausea or GERD
- Raised intracranial pressure with risk of herniation
- Children (generally not suitable; poor cooperation)
- Patients unable to understand the procedure
Preoperative preparation:
- Detailed explanation of all phases (most important - reduces anxiety and intraoperative failure)
- Psychological rehearsal ("walk-through") of the awake testing phase
- Consider anxiolytic premedication carefully - avoid benzodiazepines if ECoG-based seizure focus localisation is planned (anticonvulsant effect masks EEG activity)
- Anti-emetics (ondansetron, dexamethasone) - routine, especially if opioids are planned
- Anticonvulsants: continue or reduce by half depending on whether intraoperative EEG activation is needed
- NPO as per standard guidelines; IV access, arterial line
(Miller's Anesthesia, 10e)
4. Anaesthetic Techniques
Three broad approaches exist, each with variations:
Technique 1: Monitored Anaesthesia Care (MAC) / Sedation Throughout ("Awake-Awake-Awake")
- Patient is sedated at a light-to-moderate level throughout
- Spontaneous ventilation maintained with unprotected airway
- Titrated sedation reduced during mapping phase
- Best for cooperative patients with good tolerance
Technique 2: Asleep-Awake-Asleep (AAA) with Supraglottic Airway (LMA)
- Most widely practiced technique
- Three distinct phases:
| Phase | Technique |
|---|---|
| Phase 1 - Asleep | GA induced; LMA inserted; controlled or spontaneous ventilation; craniotomy performed under GA |
| Phase 2 - Awake | Anaesthesia stopped; LMA removed when patient responsive; cortical mapping performed |
| Phase 3 - Asleep | LMA reinserted; anaesthesia resumed; tumour resection and wound closure |
- During the awake phase, the patient communicates with the neuropsychologist/surgeon
- LMA is preferred over ETT for easier removal and less stimulation
Technique 3: Asleep-Awake-Asleep with Endotracheal Tube (ETT)
- Customised ETTs with local anaesthetic installation in glottis/trachea allow awake extubation without cough
- Used when airway concerns preclude LMA
- More stimulating; technically demanding
- Reported but less commonly used than LMA technique
(Miller's Anesthesia, 10e)
5. Scalp Nerve Block - The Cornerstone
The scalp nerve block provides analgesia for the painful phases: pin-holder placement, skin incision, craniotomy, and dural manipulation. The brain parenchyma itself is insensate.
Six nerves innervating the scalp and dura must be blocked:
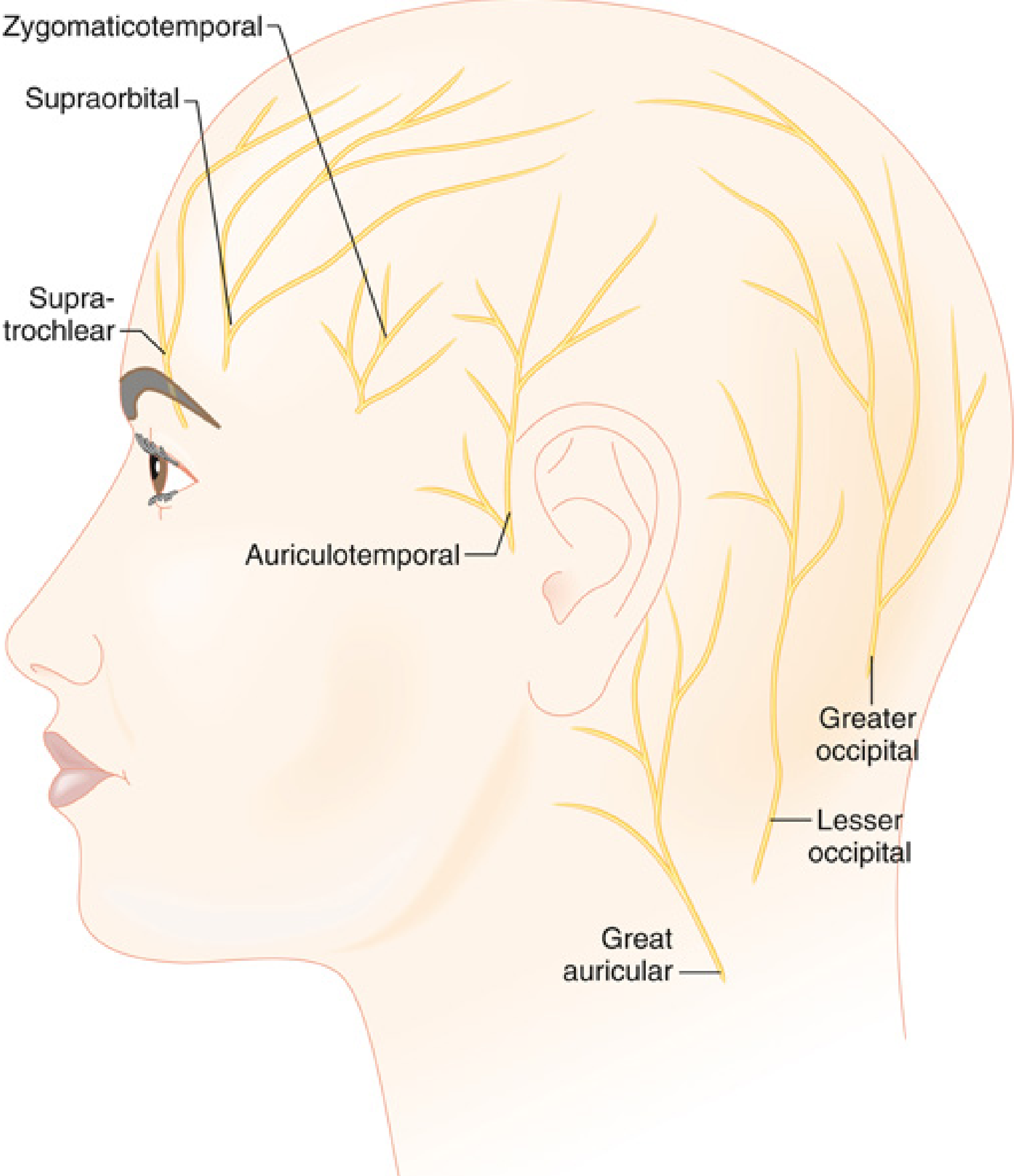
| Nerve | Origin | Area covered |
|---|---|---|
| Supratrochlear | V1 (ophthalmic) | Forehead medially |
| Supraorbital | V1 (ophthalmic) | Forehead laterally, anterior scalp |
| Zygomaticotemporal | V2 (maxillary) | Temporal region anteriorly |
| Auriculotemporal | V3 (mandibular) | Temporal region, lateral scalp |
| Lesser occipital | C2 | Posterior lateral scalp |
| Greater occipital (Great auricular) | C2-C3 | Posterior scalp, occiput |
Technique:
- Unilateral (ipsilateral to craniotomy) or bilateral depending on incision
- Local anaesthetic: ropivacaine 0.5-0.75% or bupivacaine 0.25-0.5% with or without adrenaline
- Maximum dose calculations mandatory - volumes can be substantial when combined with surgeon's pin-site infiltration and dural infiltration
- Surgeon supplements with local infiltration of pin sites, skin incision, and dura (especially subtemporal dura - most painful area)
- The anesthesiologist must track cumulative LA dose to prevent toxicity
(Miller's Anesthesia, 10e; Barash, 9e)
6. Sedation and Drug Regimens
The goals of sedation are:
- Minimise patient discomfort during painful phases (positioning, pinning, craniotomy)
- Ensure patient responsiveness and cooperation during mapping
- Minimal respiratory depression - airway inaccessible in pin fixation
- Minimal suppression of EEG activity (if ECoG planned)
- Rapid offset to allow prompt awakening for testing
Drug Options
A. Propofol-Based Regimens
- Propofol infusion (50-150 mcg/kg/min) - most widely used; rapid offset; excellent titrability
- Often combined with remifentanil (0.02-0.05 mcg/kg/min) for analgesia during painful phases
- Or combined with dexmedetomidine (0.2 mcg/kg/h)
- Critical limitation: Propofol must be discontinued at least 15 minutes before EEG/ECoG recording - it leaves a residual high-frequency, high-amplitude beta activity footprint that can obscure seizure activity
- Propofol + remifentanil: synergistic respiratory depression - great caution in pin-fixed patient
B. Dexmedetomidine-Based Regimens
- Dexmedetomidine (α2-adrenergic agonist): loading dose 0.5-1 mcg/kg over 10-20 min, then infusion 0.2-0.7 mcg/kg/h
- Key advantages:
- Sedation AND analgesia with minimal respiratory depression - safest agent for spontaneous ventilation
- Cooperative, arousable sedation - patients respond to verbal commands
- Does not suppress EEG - can be maintained during ECoG recording (0.1-0.5 mcg/kg/h during testing)
- Anxiolytic without full amnesia - patients remain cooperative
- Disadvantage: Bradycardia, hypotension; slower onset; occasional delays in arousal; less analgesic than opioid combinations
- Comparative study (Barash, 9e): propofol-remifentanil vs dexmedetomidine - similar sedation and mapping efficacy but lower rates of respiratory depression with dexmedetomidine
- Functional testing has been successfully performed with dexmedetomidine 0.1-0.2 mcg/kg/h during neurocognitive testing
C. Remifentanil Alone or Combinations
- Remifentanil infusion: excellent analgesia with rapid offset (context-sensitive half-life ~3 min); risk of respiratory depression and chest wall rigidity; requires vigilant monitoring
- Combination options:
- Propofol + remifentanil (most commonly used for MAC)
- Dexmedetomidine + remifentanil (excellent; minimal respiratory depression)
- Propofol + fentanyl + dexmedetomidine
D. Drugs to Avoid
| Drug | Reason |
|---|---|
| Benzodiazepines | Suppress EEG activity; interfere with seizure localisation; anticonvulsant; prolonged effect |
| Ketamine (high dose) | Psychomimetic effects; uncooperative patient; risk during mapping |
| Barbiturates (except therapeutic) | Suppress EEG; risk of apnoea |
| Nitrous oxide | Increases ICP; emesis; limited added benefit |
(Miller's Anesthesia, 10e; Barash, 9e)
7. Monitoring
| Monitor | Rationale |
|---|---|
| Standard ASA monitors (SpO2, ECG, NIBP) | Baseline safety monitoring |
| Capnography (ETCO2) | Essential - breath-by-breath confirmation of airway patency and respiratory drive; detects apnoea before SpO2 falls, especially with deep sedation |
| Arterial line | Beat-to-beat BP monitoring; blood sampling; required when vasoactive drugs used |
| EEG/ECoG | Seizure focus localisation in epilepsy surgery |
| Neuropsychological testing | Continuous speech, motor, sensory assessment during cortical stimulation |
| Temperature | Procedures are lengthy; hypothermia possible |
| Urinary catheter | For long procedures |
| Peripheral nerve stimulator | If neuromuscular blockade used in AAA technique |
"Reliable capnography... is essential if deep sedation is intended for any portion of the procedure." - Miller's Anesthesia, 10e
8. Intraoperative Phases and Management
Phase 1: Positioning and Pin Fixation
- Most painful phase (pericranium)
- Adequate scalp block before pin application
- Bolus sedation/analgesia at time of pinning
- Patient positioning critical: maximise neck extension and atlanto-occipital positioning before final head holder lockdown - this widens the airway and allows more latitude for sedation
- Visual access to patient's face must be maintained throughout - for speech testing (naming objects) and detecting motor responses during mapping
- Temperature management, pressure-area padding
Phase 2: Skin Incision and Craniotomy
- Moderately to deeply sedated
- Scalp block analgesia covering the incision
- Surgeon infiltrates incision line additionally
- Monitoring SpO2 and ETCO2 continuously
Phase 3: Dural Opening
- Subtemporal dura traction is particularly painful - ensure adequate dural infiltration with LA
- Commence reducing sedation in preparation for awake phase
- If LMA-based AAA: commence waking patient; remove LMA when responsive
Phase 4: Awake Cortical Mapping (Critical Phase)
- Patient fully awake and cooperative
- Electrocorticography (ECoG): cortical surface EEG to localise seizure foci
- If no spontaneous activity: provocative agents used
- Methohexital 0.3 mg/kg - safe, effective seizure activation agent
- Etomidate 0.05-0.1 mg/kg - alternative
- Alfentanil bolus 30-50 mcg/kg; Remifentanil 2.5 mcg/kg - under GA
- Hyperventilation - helps activate foci
- Direct cortical stimulation mapping: bipolar stimulator applied to brain surface
- Motor mapping: observe for movement in contralateral limbs/face
- Speech mapping: naming task (patient asked to name images) - speech arrest or errors indicate language cortex
- Sensory mapping: patient reports tingling/paraesthesia
- Dexmedetomidine can be maintained at low rates (0.1-0.2 mcg/kg/h) during mapping without interfering with testing
Phase 5: Tumour Resection and Closure
- Sedation resumed; LMA reinserted if AAA technique
- Anaesthesia for closure
9. Complications and Management
| Complication | Incidence | Management |
|---|---|---|
| Intraoperative seizures | ~3-10% | Cold saline irrigation of cortex (first line); cease stimulation; propofol 0.5-1 mg/kg IV increments (wait briefly to see if self-limiting before giving propofol - propofol suppresses EEG); if refractory: benzodiazepines as last resort |
| Airway obstruction / Apnoea | ~1-5% | Jaw thrust; nasopharyngeal airway; reduce/stop propofol/remifentanil; emergency LMA/ETT - severely hindered by pin-fixed head; prevention critical |
| Respiratory depression | Common with propofol + opioids | Verbal stimulation; reduce sedation; supplemental O2; ETCO2 monitoring |
| Uncooperative / agitated patient | ~5% | Reassurance; repositioning; small propofol bolus; abort to GA if necessary |
| Nausea and vomiting | Common with opioids | Prophylactic ondansetron + dexamethasone; avoid/minimise opioids |
| Uncontrolled pain | Inadequate scalp block | Supplemental LA by surgeon; small ketamine boluses; fentanyl bolus |
| Intractable brain oedema | Rare | Mannitol, hyperventilation, head-up position, steroids; may require GA conversion |
| Haemodynamic instability | Dexmedetomidine bradycardia; catecholamine surges | Atropine for bradycardia; ephedrine/phenylephrine for hypotension |
| Conversion to GA | ~2-8% | Pre-planned emergency GA plan; video laryngoscope available; RSI with appropriate head position strategies |
| Post-dural puncture headache | N/A for craniotomy | N/A |
| Postoperative neurological deficit | From resection | PACU or ICU monitoring; post-op neurological assessment |
"Seizures usually stop with cessation of stimulus or with irrigation of the cortex with cold saline." - Miller's Anesthesia, 10e
10. Postoperative Management
- PACU or ICU observation (neurological observations every 15-30 min initially)
- Multimodal analgesia: paracetamol, NSAIDs (cautiously), scalp infiltration of long-acting LA
- Nausea prophylaxis continued
- Anticonvulsant medication maintained/resumed
- Monitoring for: delayed seizures, neurological deterioration, haematoma (headache, reduced GCS), raised ICP, pneumocephalus
- Steroids (dexamethasone) to reduce cerebral oedema
- VTE prophylaxis when appropriate
11. Summary Comparison - Anaesthetic Approaches
| Technique | Airway | Sedation | Best For |
|---|---|---|---|
| MAC throughout | Unprotected, spontaneous | Propofol ± remifentanil ± dex | Cooperative patient; short procedures |
| AAA - LMA | LMA Phase 1&3; unprotected Phase 2 | Propofol ± remifentanil ± dex | Most cases; flexible |
| AAA - ETT | ETT Phase 1; unprotected Phase 2; ETT Phase 3 | GA then emergence | High aspiration risk; obese patients |
| Dex + remifentanil MAC | Unprotected | Dex + remifentanil | ECoG-based procedures; respiratory risk |
Key Examination Points
- The essential element is the scalp nerve block - sedation cannot compensate for inadequate local anaesthesia
- Six nerves of the scalp must be blocked: supratrochlear, supraorbital, zygomaticotemporal, auriculotemporal, lesser occipital, greater occipital
- Propofol must be stopped ≥15 min before ECoG - residual beta activity obscures seizure focus
- Dexmedetomidine advantage: sedation + analgesia with minimal respiratory depression; can be maintained during mapping at 0.1-0.2 mcg/kg/h
- Capnography is essential - airway is all but inaccessible with head in pin fixation
- Avoid benzodiazepines as premedication if ECoG is planned
- Seizures during mapping - cold saline first; then propofol 0.5-1 mg/kg; wait before giving propofol in case self-limiting
- Conversion to GA is pre-planned - video laryngoscope must be immediately available
Sources:
- Miller's Anesthesia, 2-Volume Set, 10th Edition (Chapter 53: Awake Craniotomy and Seizure Surgery)
- Barash, Cullen & Stoelting's Clinical Anesthesia, 9th Edition (Chapter: Awake Craniotomy)
- Morgan & Mikhail's Clinical Anesthesiology, 7th Edition
Brain Death And Organ Harvesting 30 mark Question
Finding Sources
Finding Sources
Searching the Web
brain death criteria diagnosis organ harvesting anaesthesia management 2024 guidelines
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading Web Page
anaesthesia organ harvesting brain dead donor intraoperative management
Finding Sources
Finding Sources
Reading File
Reading File
I now have comprehensive, authoritative content from multiple textbooks and clinical guidelines. Let me compile the complete 30-mark answer.
Brain Death and Organ Harvesting — 30-Mark Model Answer (Anaesthesia MD Examination)
1. Definition and Historical Context
Brain death (death by neurological criteria, DNC) is defined as the irreversible cessation of function of the whole brain, including the brainstem, in a patient on mechanical ventilation with a beating heart.
- First codified by the Harvard Ad Hoc Committee in 1968, following the world's first cardiac transplant by Dr Christiaan Barnard in 1967
- Incorporated into the Uniform Determination of Death Act (USA) and legally recognised in most countries
- The legal time of death is the moment the apnoea test confirms PaCO2 criteria are met in the absence of any respiratory effort
- Equivalent terms: death by neurological criteria (DNC), brain stem death (BSD - UK terminology)
"Brain death, as a clinical entity, was first proposed in 1968 by an Ad Hoc Committee at the Harvard Medical School... This redefining of death has been instrumental in permitting retrieval of viable organs for transplantation." - Plum & Posner
2. Causes of Brain Death
| Category | Examples |
|---|---|
| Traumatic | Severe traumatic brain injury (TBI) - most common |
| Vascular | Aneurysmal subarachnoid haemorrhage (aSAH), massive intracerebral haemorrhage, ischaemic stroke with herniation |
| Anoxic-ischaemic | Cardiac arrest with prolonged resuscitation |
| Infective/Inflammatory | Fulminant meningitis/encephalitis |
| Metabolic | Fulminant hepatic failure with cerebral oedema |
| Mass lesions | Large tumour with uncontrollable herniation |
The brainstem is very resilient to injury; true brain death is relatively uncommon. (Bradley & Daroff's Neurology)
3. Prerequisites Before Brain Death Testing (5 marks)
Before the clinical examination can be performed, ALL prerequisites must be satisfied. Failure to exclude confounders is a major source of error.
A. Establish Irreversible Cause of Coma
- Known, structural, irreversible catastrophic neurological injury
- Neuroimaging (CT/MRI) explains the coma
- Patient has received aggressive treatment (osmotherapy, ICP management, surgery) and further treatment is futile
B. Exclude Confounding Conditions
| Confounder | Requirement |
|---|---|
| Hypothermia | Core temperature must be ≥36°C |
| Drug intoxication | Sedatives, hypnotics, opioids, anaesthetic agents must be excluded; toxicology screen if uncertain; wait appropriate elimination time (usually 5 half-lives) |
| Neuromuscular blocking agents | Confirm complete reversal using train-of-four peripheral nerve stimulator (4/4 twitches) |
| Metabolic disturbances | Correct severe electrolyte abnormalities, acid-base disturbances, hypoglycaemia |
| Severe cardiovascular instability | Systolic BP must be ≥100 mmHg before testing |
| Pharmacological paralysis | No residual neuromuscular blockade |
"Because the history early in the course is often fragmentary and the use of sedative and analgesic medications is often unknown, brain death should not be determined within hours of emergency department evaluation." - Bradley & Daroff's Neurology
C. Qualified Examiners
- Two independent doctors (in most countries) - neither involved in transplant team
- Senior physicians (consultant/attending) qualified in neurology, neurosurgery, or intensive care
- Two separate examinations, separated by an appropriate observation period (institution-dependent)
4. Clinical Examination for Brain Death (8 marks)
The examination has three components: establishing deep coma, testing brainstem reflexes, and the apnoea test.
A. Level of Consciousness
- Unresponsive to all stimuli
- No purposeful motor response to painful stimulation (deep pressure on condyles of TMJ, supraorbital notch, nail beds, sternal rub)
- Motor responses from spinally-mediated reflexes (Lazarus sign - arms rising and meeting midline) may still occur and are not incompatible with brain death, but require explanation
- Decerebrate or decorticate posturing IS incompatible with brain death
B. Brainstem Reflexes - All Must Be Absent Bilaterally
| Reflex | Cranial Nerve | Test | Brain Death Finding |
|---|---|---|---|
| Pupillary light reflex | CN II, III | Bright light to each eye | Fixed, dilated pupils (4-9mm); no constriction bilaterally |
| Corneal reflex | CN V, VII | Cotton/suction catheter touches cornea | No blink bilaterally |
| Oculocephalic reflex (Doll's eye) | CN III, VI, VIII | Rapid head turning (contraindicated if C-spine injury) | Eyes remain fixed (no conjugate movement) |
| Oculovestibular reflex (Caloric) | CN VIII, III, VI | Head at 30°; 50 mL ice water instilled in each ear; wait 5 min between sides; observe 1 min | No eye deviation toward irrigated side bilaterally |
| Gag reflex | CN IX, X | Stimulate posterior oropharynx | Absent gag |
| Cough reflex | CN X | Suction catheter passed to carina | Absent cough |
| Grimace to pain | CN V, VII | Noxious stimulation to face | No grimacing |
Clinical findings NOT compatible with brain death:
- Nystagmus or spontaneous eye movements
- Conjugate eye deviation
- Pinpoint pupils (suggests opioid effect)
- Decerebrate/decorticate posturing
- Grimacing to pain
(Bradley & Daroff's Neurology, 8th Ed.)
C. Apnoea Test
Purpose: Demonstrate absence of respiratory drive at the level of the medullary respiratory centre.
Prerequisites:
- Systolic BP ≥100 mmHg (vasopressors if needed)
- PaO2 ≥200 mmHg (pre-oxygenate with 100% O2 for 10 minutes)
- Normalise PaCO2 to baseline (35-45 mmHg) by adjusting ventilator
Technique:
- Obtain baseline ABG confirming normocapnia and adequate oxygenation
- Disconnect from ventilator
- Deliver 100% O2 via catheter at carina level (6 L/min) - apnoeic oxygenation maintains SpO2
- Observe for any respiratory effort (chest/abdominal excursion, gasping) for 8-10 minutes
- Obtain ABG at end of observation period
Positive Test (Brain Death Confirmed) When:
- No respiratory effort is observed AND
- PaCO2 ≥60 mmHg OR a rise of ≥20 mmHg from a normal baseline PaCO2
Abort apnoea test if:
- SpO2 falls below 85-90% (despite apnoeic oxygenation)
- Severe haemodynamic instability (hypotension, severe arrhythmia)
- In these cases, proceed to ancillary/confirmatory tests
Time of death = time PaCO2 target is achieved in the absence of respiratory effort. (Bradley & Daroff's Neurology)
5. Ancillary (Confirmatory) Tests
Not routinely required in most countries if the clinical examination (including apnoea test) is complete and unambiguous. Indicated when:
- Clinical exam cannot be completed (e.g., severe facial trauma, severe lung disease preventing apnoea test)
- Confounders cannot be fully excluded
- Legal or institutional requirements
- Religious/cultural objections to clinical criteria alone
| Test | Finding in Brain Death | Notes |
|---|---|---|
| EEG | Electrocerebral silence (isoelectric - no potentials >2 mV over 30 min recording, ≥8 electrodes) | Can be falsely isoelectric with hypothermia, drug overdose; does NOT confirm brainstem death alone |
| Cerebral angiography (4-vessel) | Absent intracranial blood flow | Gold standard; invasive |
| CT Angiography (CTA) | Absent intracranial circulation | Non-invasive; preferred in many centres |
| Radionuclide Scintigraphy (HMPAO-SPECT) | No cerebral perfusion ("hollow skull sign") | Useful when CTA unavailable |
| Transcranial Doppler (TCD) | Reverberant flow/systolic spikes only; no net flow | Non-invasive; operator-dependent; technical pitfalls |
| Brainstem Auditory Evoked Potentials (BAEPs) | Absent waves III-V | Tests brainstem conduction |
| Somatosensory Evoked Potentials | Absent cortical N20 | Supplements EEG |
"Cerebral angiography, cerebral perfusion scintigraphy, or transcranial Doppler have been used to demonstrate cessation of cerebral blood flow as ancillary tests." - Bradley & Daroff
6. Communication with Family
- Family should not be surprised by brain death - they should have been counselled about the prognosis from the time of severe brain injury
- Announcement: "Your loved one has died but is being supported by machines"
- Organ donation discussion occurs separately from the brain death declaration - by organ procurement organisation (OPO) personnel, not the treating team
- In the USA: federal law requires physician to contact the OPO
- Cultural/religious sensitivity mandatory - some faiths (Orthodox Jewish, Japanese tradition) may not accept brain death criteria
- Family refusal remains a major cause of lost donor potential
7. Types of Organ Donation
A. Donation After Brain Death (DBD)
- Heart-beating donor
- Optimal organ quality (warm ischaemia avoided)
- Allows time for full evaluation and multiple organ procurement
- Accounts for ~70% of deceased donors (USA)
B. Donation After Circulatory (Cardiac) Death (DCD)
- Non-heart-beating donor
- Maastricht Classification:
| Category | Description | Type |
|---|---|---|
| I | Dead on arrival | Uncontrolled |
| II | Unsuccessful resuscitation | Uncontrolled |
| III | Imminent cardiac arrest (planned withdrawal of life support) | Controlled |
| IV | Cardiac arrest in brain-dead donor | Controlled |
- Controlled DCD (Cat III) most common: life support withdrawn in OT; organ procurement begins after 5-minute "no-touch" period of confirmed cardiac arrest
- Warm ischaemia time is longer in uncontrolled DCD - reduces organ quality
- DCD accounted for 30.2% of deceased donors in USA in 2021 (Miller's Anesthesia, 10e)
8. Pathophysiology Following Brain Death - "The Catecholamine Storm" (4 marks)
Brain death triggers a massive, predictable sequence of physiological derangements that threaten organ viability. Understanding this is the basis of all donor management.
Phase 1: Autonomic Storm (Cushing Response/Catecholamine Surge)
- As intracranial pressure rises and herniation occurs, brainstem ischaemia triggers an intense sympathetic discharge
- Plasma catecholamines rise 10-100x above baseline
- Cardiovascular effects: severe hypertension, tachycardia, arrhythmias, myocardial ischaemia, reversible left ventricular dysfunction (catecholamine cardiomyopathy)
Phase 2: Post-Herniation Cardiovascular Collapse
- Loss of sympathetic tone → systemic vasodilation, increased venous capacitance, relative hypovolaemia
- Exacerbated by prior osmotherapy (mannitol), diuresis, and inadequate fluid resuscitation
- Progressive hypotension requiring vasopressors
Phase 3: Hypothalamic-Pituitary Axis Disruption
Brain death destroys the hypothalamic-pituitary axis, causing:
| Derangement | Mechanism | Clinical Effect |
|---|---|---|
| Central diabetes insipidus (DI) | Loss of ADH (vasopressin) | Massive polyuria, hypernatraemia, hyperosmolaemia |
| Thyroid hormone deficiency | Loss of TSH | Reduced cardiac contractility, metabolic suppression |
| Adrenocortical failure | Loss of ACTH/cortisol | Haemodynamic instability, electrolyte disturbances |
| Insulin deficiency/resistance | Loss of hypothalamic regulation | Hyperglycaemia |
Phase 4: Systemic Consequences
- Hypothermia - loss of hypothalamic temperature regulation
- Coagulopathy - DIC from thromboplastin release from injured brain
- Pulmonary oedema - neurogenic (sympathetic storm) + aspiration risk
- Anaemia - from haemorrhage, haemodilution
- Infection - ICU-acquired, aspiration pneumonia
9. ICU Management of the Brain-Dead Organ Donor (5 marks)
The focus shifts from cerebral preservation to organ preservation. The key principle: avoid ischaemia to all donor organs.
The "Rule of 100s" (Trauma Surgery guideline)
- Systolic BP >100 mmHg
- Urine output >100 mL/h
- PaO2 >100 mmHg
A. Haemodynamic Goals
| Parameter | Target |
|---|---|
| Mean Arterial Pressure (MAP) | ≥60-70 mmHg |
| Systolic BP | >100 mmHg |
| CVP | 6-10 mmHg (4-8 for lung-optimised protocol) |
| Heart rate | 60-100/min |
| Cardiac index | >2.4 L/min/m² |
| Mixed venous O2 saturation | >60% |
- Vasopressors: Noradrenaline (norepinephrine) first choice; vasopressin has dual benefit (vasopressor + treats DI); avoid high-dose dopamine
- Fluid resuscitation: balanced crystalloids; albumin; avoid synthetic starches
- Inotropes (dopamine, dobutamine) if cardiogenic dysfunction
B. Respiratory Goals (Critical for Lung Donation)
| Parameter | Target |
|---|---|
| SpO2 | >95% |
| PaO2 | >100 mmHg |
| PaCO2 | 35-45 mmHg |
| TV | 6-8 mL/kg (lung-protective) |
| PEEP | 5-8 cm H2O |
| FiO2 | Minimum to achieve target SpO2 |
- Frequent suctioning; HOB 30-45°; avoid ventilator-associated pneumonia
- Lung-protective ventilation critical for lung procurement
C. T4 Hormonal Resuscitation Protocol
The T4 (hormone replacement) protocol addresses hypothalamic-pituitary disruption and has been shown to improve organ donation rates:
| Drug | Dose | Purpose |
|---|---|---|
| Methylprednisolone | 15 mg/kg IV bolus | Anti-inflammatory; adrenal replacement; improves lung function |
| Tri-iodothyronine (T3) or Thyroxine (T4) | T3: 4 mcg bolus then 3 mcg/h; or T4: 20 mcg bolus then 10 mcg/h | Restores cardiac contractility; reverses metabolic suppression |
| Vasopressin (ADH) | 0.5-2.4 U/h infusion | Treats DI; vasopressor; reduces noradrenaline requirements |
| Insulin | Titrated to glucose 6-10 mmol/L | Glycaemic control; reduces ischaemia-reperfusion injury |
"Early initiation of hormonal therapy has shown improved organ donation rates and should be considered in all brain-dead potential organ donors." - Mulholland's Surgery, 7e
D. Specific Organ Targets
| System | Management |
|---|---|
| Kidneys | Adequate MAP and urine output (>1 mL/kg/h); avoid nephrotoxins; optimise fluid balance |
| Heart | Treat arrhythmias; maintain sinus rhythm; avoid high-dose inotropes; echocardiography to assess function |
| Liver | Normalise glucose; avoid hepatotoxic drugs; maintain adequate perfusion |
| Lungs | Lung-protective ventilation; apnoeic oxygenation trials; bronchoscopy if secretions |
| Pancreas | Glycaemic control; maintain perfusion |
| Corneas/Skin | Clock starts on BD declaration - can retrieve up to 24h later |
E. Diabetes Insipidus Management
- Urine output >3-4 mL/kg/h + rising serum Na+ + low urine osmolality (hypotonic)
- Vasopressin (desmopressin DDAVP 0.5-2 mcg IV q6h, or vasopressin infusion)
- Replace fluid losses with 0.45% NaCl or 5% dextrose
- Target sodium: 130-155 mmol/L
10. Anaesthesia for Organ Procurement (Harvesting) in the Operating Theatre (6 marks)
Role of the Anaesthesiologist
The anaesthesiologist must:
- Verify the brain death certificates
- Confirm family consent is in order
- Confirm no absolute contraindications to donation (e.g., active HIV, active malignancy)
- Continue ICU-level haemodynamic support
- Manage spinal reflexes and haemodynamic responses to surgical stimulation
Why Anaesthesia is Required Despite Brain Death?
The brain-dead donor has no cortical or brainstem function, so consciousness and pain are impossible. However:
- Spinal cord reflexes remain intact and may cause gross movements (Lazarus reflex, limb movements) during surgical stimulation, which is distressing to the surgical team
- Haemodynamic reflexes - surgical stimulation can cause spinal-sympathetic reflex responses: hypertension and tachycardia (without pain perception), which can worsen catecholamine-mediated organ injury
- Volatile agents may provide ischaemic preconditioning - theoretical benefit for organ protection
- Muscle relaxants provide optimal surgical conditions
"Neuromuscular blockade required to inhibit spinal motor reflexes... volatile anaesthetics due to theoretical advantage of ischaemic preconditioning... brain death may cause haemodynamic response to noxious stimuli; hypertension should be avoided." (BC Transplant Anaesthesia Guidelines, 2024)
Monitoring in OT
| Monitor | Rationale |
|---|---|
| Standard ASA monitoring | ECG, SpO2, ETCO2, NIBP |
| Arterial line | Beat-to-beat BP; ABGs; rapid responses to instability |
| Central venous catheter | CVP monitoring; vasopressor/inotrope delivery |
| Urinary catheter | Hourly urine output |
| Temperature | Hypothermia prevention |
| Peripheral nerve stimulator | Confirm NMB |
| Hourly ABG, electrolytes, glucose, lactate | Organ protection |
Anaesthetic Technique
Induction/Maintenance:
- Neuromuscular blockade (NMB): suxamethonium/rocuronium; maintain throughout
- Volatile anaesthetic (isoflurane/sevoflurane): 0.5-1 MAC - suppresses spinal motor reflexes; ischaemic preconditioning
- Opioids (fentanyl): to attenuate haemodynamic responses to incision - not for analgesia (brain dead) but to reduce reflex hypertension
- Continue vasopressors and inotropes as per ICU management
- Ventilation: lung-protective strategy as per ICU
Intraoperative Haemodynamic Goals:
| Parameter | Target |
|---|---|
| MAP | >60 mmHg |
| Systolic BP | >100 mmHg |
| Heart rate | 60-100/min |
| CVP | 6-10 mmHg initially; reduced to 4-6 mmHg after heart/lung procurement; raised to 10-12 mmHg for kidney procurement |
| Urine output | >1 mL/kg/h |
| Temperature | >35°C |
"In a stable patient, one may keep CVP 'low' till heart and lung are harvested. Thereafter the CVP is raised to 10-12 mmHg for the benefit of urosurgeons." - NOTTO Guidelines (India)
Drug Management:
- Continue vasopressin infusion for DI
- Insulin to maintain glucose 6-10 mmol/L
- Methylprednisolone if not already given
- NAC (N-acetylcysteine) 30 mg/kg 1 hour before procurement; 300 mg via portal vein before cross-clamp - shown to improve graft survival
- Prophylactic broad-spectrum antibiotics (cephalosporin)
- Heparin IV bolus (300-400 units/kg) before aortic cross-clamping - to prevent vascular thrombosis during cold flush
Surgical Sequence (Multi-organ Procurement)
- Midline incision - suprasternal notch to pubis
- Thoracic dissection - heart, lungs mobilised
- Abdominal dissection - liver, pancreas, kidneys, bowel
- Heparin given before cross-clamping
- Aortic cross-clamp (supradiaphragmatic) + cold perfusion with preservation solution begins
- At cross-clamp: all vasopressors ceased; ventilator stopped
- Cardioplegia for heart
- Sequential organ removal in order of ischaemia tolerance:
- Heart (most sensitive - 4h cold ischaemia)
- Lungs (6h cold ischaemia)
- Liver (12-24h)
- Pancreas (12-24h)
- Kidneys (24-36h)
- Intestines (8-12h)
- Corneas, skin, bones - post-cardiac death
11. Donation After Circulatory Death (DCD) - Anaesthetic Implications
- Life support withdrawn in OT (Maastricht III) - comfort care drugs (morphine, midazolam) given to relieve any distress
- No-touch period of 2-5 minutes after cardiac arrest (permanent cardiac arrest confirmed)
- Rapid organ retrieval begins immediately after no-touch period
- Warm ischaemia time is the critical variable - shorter warm ischaemia = better organ outcomes
- Ex-vivo machine perfusion (normothermic or hypothermic) increasingly used to recondition DCD organs
12. Ethical and Legal Considerations
| Issue | Principle |
|---|---|
| Dead donor rule | Organs must not be retrieved until death is declared; death must not be caused by organ procurement |
| Consent | Informed consent from next-of-kin; donor card/advance directive |
| Separation of teams | Brain death declaration team ≠ transplant team |
| Non-maleficence | Comfort care not withheld for organ-preservation purposes in DCD |
| Justice | Equitable organ allocation (UNOS/OPTN in USA; NOTTO in India) |
| Cultural/religious sensitivity | Orthodox Judaism, some Asian cultures may reject brain death criteria; requires cultural intermediaries |
| Medicolegal | In medicolegal cases, permission from appropriate authority required before procurement |
13. Summary - Key Examination Points
- Harvard criteria 1968 - first formalised brain death; 25 assessments required
- Three absolute requirements for brain death: deep coma (known irreversible cause) + all brainstem reflexes absent + apnoea test positive (PaCO2 ≥60 mmHg or rise ≥20 mmHg, no respiratory effort)
- Five confounders to exclude before testing: hypothermia, drugs, NMB, metabolic, hypotension
- Ancillary tests (EEG, CTA, SPECT, TCD) - not routinely required; used when clinical exam incomplete
- Catecholamine storm → haemodynamic collapse → hypothalamic-pituitary failure → DI, hypothyroidism, adrenal failure
- T4 protocol: methylprednisolone + T3/T4 + vasopressin + insulin
- Anaesthesia in OT: NMB + volatile agent + opioids = suppress spinal reflexes + haemodynamic responses; NOT for consciousness (brain dead)
- CVP strategy: low (4-8) during heart/lung harvesting; raise (10-12) for kidney procurement
- Dead donor rule and separation of teams are non-negotiable ethical principles
- DCD donors now account for 30% of deceased donors in the USA; Maastricht classification
Sources:
- Miller's Anesthesia, 2-Volume Set, 10th Edition
- Bradley & Daroff's Neurology in Clinical Practice, 8th Edition
- Plum & Posner's Diagnosis and Treatment of Stupor and Coma, 5th Edition
- Mulholland & Greenfield's Surgery: Scientific Principles and Practice, 7th Edition
- BC Transplant - Anesthesia for Donors following Death by Neurological Criteria (2024)
- NOTTO (National Organ & Tissue Transplant Organisation) India - OT Guidelines
This is a shared conversation. Sign in to Orris to start your own chat.