Monroe-Kellie doctrine
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Finding Sources
I now have thorough textbook content. Here is the complete answer:
Monroe-Kellie Doctrine
Core Concept
The Monroe-Kellie doctrine (also written Monro-Kellie) states that the skull is a rigid, fixed-volume compartment, and the sum of its three contents must remain constant at all times:
| Compartment | Normal proportion |
|---|---|
| Brain parenchyma | ~80-90% |
| Cerebrospinal fluid (CSF) | ~10% |
| Intracranial blood (arterial + venous) | ~10% |
"The Monroe-Kellie doctrine simply states that the total volume of contents remains constant within the skull that is rigid and nonexpansile."
- Mulholland & Greenfield's Surgery, p. 1111
Any increase in the volume of one compartment must be offset by a reduction in one or both of the others. If compensation fails, intracranial pressure (ICP) rises.
Compensatory Mechanisms (in order of recruitment)
When a space-occupying process begins (e.g., expanding hematoma, edema, tumor), the brain compensates sequentially:
- CSF displacement - CSF is shifted out of the cranial vault into the spinal subarachnoid space. Radiographically, this appears as ventricular effacement, sulcal effacement, and reduced conspicuity of the basal cisterns.
- Venous blood displacement - The cerebral venous compartment (a largely passive, compressible system) is squeezed, reducing intracranial blood volume.
- Once both are exhausted - The system becomes non-compliant. Even a tiny additional volume increment causes a steep, exponential rise in ICP.
The Pressure-Volume (Compliance) Curve
This non-linear relationship is the most clinically important consequence of the doctrine:
- On the flat portion of the curve (good compensatory reserve): large volume additions cause minimal ICP change.
- At the steep "elbow" of the curve: compensatory mechanisms are near-exhausted; ICP begins to climb.
- On the steep portion (low compliance): a trivially small volume increase causes a dramatic ICP spike.
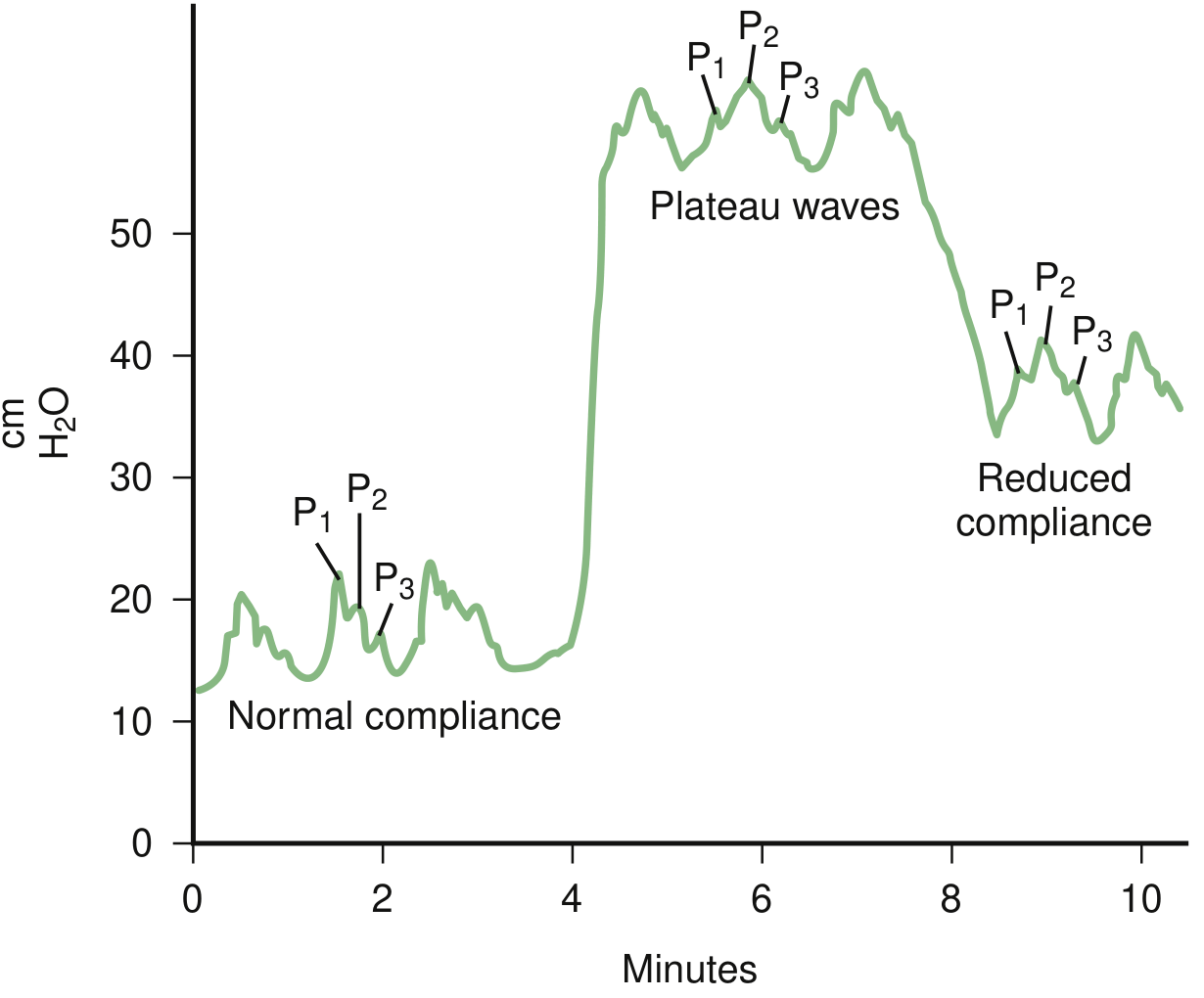
ICP waveform tracings showing normal compliance (left, P1 > P2 > P3), plateau waves (Lundberg A waves, center) reflecting critically reduced compliance, and residual reduced compliance (right). - Bradley and Daroff's Neurology, Fig. 53.3
The normal ICP waveform has three peaks: P1 (percussion wave, normally tallest), P2 (tidal wave), P3 (dicrotic wave). When compliance falls, P2 rises above P1 - this is a bedside sign of impending ICP crisis.
Normal ICP Values
- Normal supine ICP: < 15 mmHg (measured at the level of the foramen of Monro, referenced to the tragus)
- Pathological threshold requiring treatment: > 20-25 mmHg
- ICP approaching mean arterial pressure (MAP) is incompatible with cerebral perfusion
Cerebral Perfusion Pressure (CPP)
CPP ties the doctrine directly to clinical management:
CPP = MAP - ICP
- Target CPP in severe TBI: 60-70 mmHg (first 48-72 hours)
- If ICP rises unchecked or MAP falls, CPP drops - the brain becomes ischemic
- Cerebral autoregulation (vasoconstriction/dilation of precapillary venules) maintains adequate cerebral blood flow (CBF) across a MAP range of 50-150 mmHg in an intact brain
- Autoregulation is disrupted in ~1/3 of severe TBI patients - in these patients, MAP rises directly inflate cerebral blood volume, worsening ICP
Clinical Consequences of Exhausted Compensation
When the buffer is gone, pathological events cascade:
- Plateau waves (Lundberg A waves) - Sustained ICP spikes to 50-100 mmHg lasting 5-20 minutes, triggered by episodic arterial vasodilation. Clinically manifest as transient confusion, stupor, visual obscurations, headache, or Cushing's triad.
- Herniation syndromes - Brain tissue shifts through dural openings (subfalcine, transtentorial, tonsillar). Transtentorial herniation compresses the posterior cerebral artery, causing occipital infarction; subfalcine herniation compresses the anterior cerebral artery.
- Cushing's triad - Hypertension + bradycardia + irregular respiration - a terminal reflex attempt to maintain CPP.
- Global ischemia / brain death - When ICP equals MAP, CPP = 0 and cerebral circulation arrests.
Sequence of Vascular Compromise
"The venous circulation is initially affected and then arterial inflow is reduced as the cerebral perfusion pressure falls, representing the clinical endpoint of a cascade resulting in diffuse brain ischaemia."
- Grainger & Allison's Diagnostic Radiology
Therapeutic Implications
The doctrine directly informs every ICP-lowering intervention:
| Target | Intervention |
|---|---|
| Reduce brain volume | Osmotherapy (mannitol, hypertonic saline), steroids (vasogenic edema), surgical decompression |
| Reduce CSF volume | Ventriculostomy/EVD, lumbar drain |
| Reduce cerebral blood volume | Head elevation (30°), controlled hyperventilation (temporizing - lowers PaCO₂, causes vasoconstriction), avoid hypercapnia |
| Maintain CPP | Vasopressors to support MAP, treat elevated ICP |
Sources: Mulholland & Greenfield's Surgery, 7e, p. 1111 | Bradley and Daroff's Neurology in Clinical Practice | Grainger & Allison's Diagnostic Radiology | Plum and Posner's Diagnosis and Treatment of Stupor and Coma | Miller's Anesthesia, 10e
This is a shared conversation. Sign in to Orris to start your own chat.