60 yr old female known SHTN came with dyspnea for 1 day and pedal edema for 1 week
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Loading Image
Now I have comprehensive information. Let me compile a thorough clinical response.
Clinical Case Analysis: 60F with SHTN, Dyspnea (1 day) + Pedal Edema (1 week)
Most Likely Diagnosis
Acute Decompensated Heart Failure (ADHF) - most likely HFpEF (Heart Failure with Preserved Ejection Fraction) secondary to hypertensive heart disease.
The classic triad:
- Known systemic hypertension - the primary underlying cause
- Pedal edema for 1 week - gradual volume overload (backward failure)
- Acute dyspnea for 1 day - acute decompensation with pulmonary congestion
This is the "Typical Hypertensive" ADHF phenotype - usually not volume overloaded as much as fluid redistributed, and elevated BP at presentation is the driver.
Pathophysiology
Chronic hypertension leads to:
- Concentric LV hypertrophy - increased wall thickness, reduced compliance
- Diastolic dysfunction - impaired LV relaxation and filling
- HFpEF - elevated filling pressures despite preserved EF
- Any precipitant (salt load, medication non-compliance, new arrhythmia) tips the patient into acute decompensation with pulmonary edema and peripheral fluid redistribution
History to Elicit
Cardiac symptoms:
- Orthopnea (number of pillows), PND, bendopnea
- Chest pain/palpitations (rule out ACS, AF as precipitant)
- Previous similar episodes / prior HF diagnosis
Precipitating factors:
- Medication non-adherence (antihypertensives, diuretics)
- Dietary salt excess
- Use of NSAIDs, thiazolidinediones, cold/flu preparations
- Recent febrile illness or infection
- Reduced urine output
Background:
- Duration and control of hypertension
- DM, CKD, CAD, valvular disease
- Alcohol, smoking
Examination
| Finding | Significance |
|---|---|
| BP (elevated or low?) | Hypertensive ADHF vs low-output state |
| HR, SpO2, RR | Hemodynamic severity |
| JVP elevated | Right-sided congestion |
| Basal crepitations | Pulmonary edema |
| S3 gallop | Ventricular dysfunction |
| Pitting pedal edema | Volume overload |
| Hepatomegaly | Congestion |
| Loud P2 | Pulmonary hypertension |
Investigations
Immediate:
- ECG - LVH, arrhythmia (AF), ischemia
- CXR - cardiomegaly, pulmonary venous congestion, Kerley B lines, pleural effusion
- BNP / NT-proBNP - class I recommendation for diagnosis of acute HF; highly elevated in ADHF (BNP >100 pg/mL, NT-proBNP >300 pg/mL)
- SpO2 / ABG - degree of hypoxia
- CBC - anemia as precipitant
- RFT (Creatinine, BUN, electrolytes) - cardiorenal syndrome (BUN >43 mg/dL and Cr >2.75 mg/dL are markers of worse prognosis)
- LFT - hepatic congestion
- Blood glucose, HbA1c - DM comorbidity
- Troponin - rule out ACS as precipitant
Non-urgent:
- Echocardiography - most important: assess EF (HFrEF vs HFpEF), LVH, diastolic dysfunction grading, valvular disease, wall motion abnormalities
- Thyroid function (hyperthyroidism as precipitant)
Management
Phenotype Classification (This Patient)
Given known hypertension and this presentation, she most likely fits the "Hypertensive ADHF" phenotype (BP elevated, fluid redistribution rather than pure volume overload):
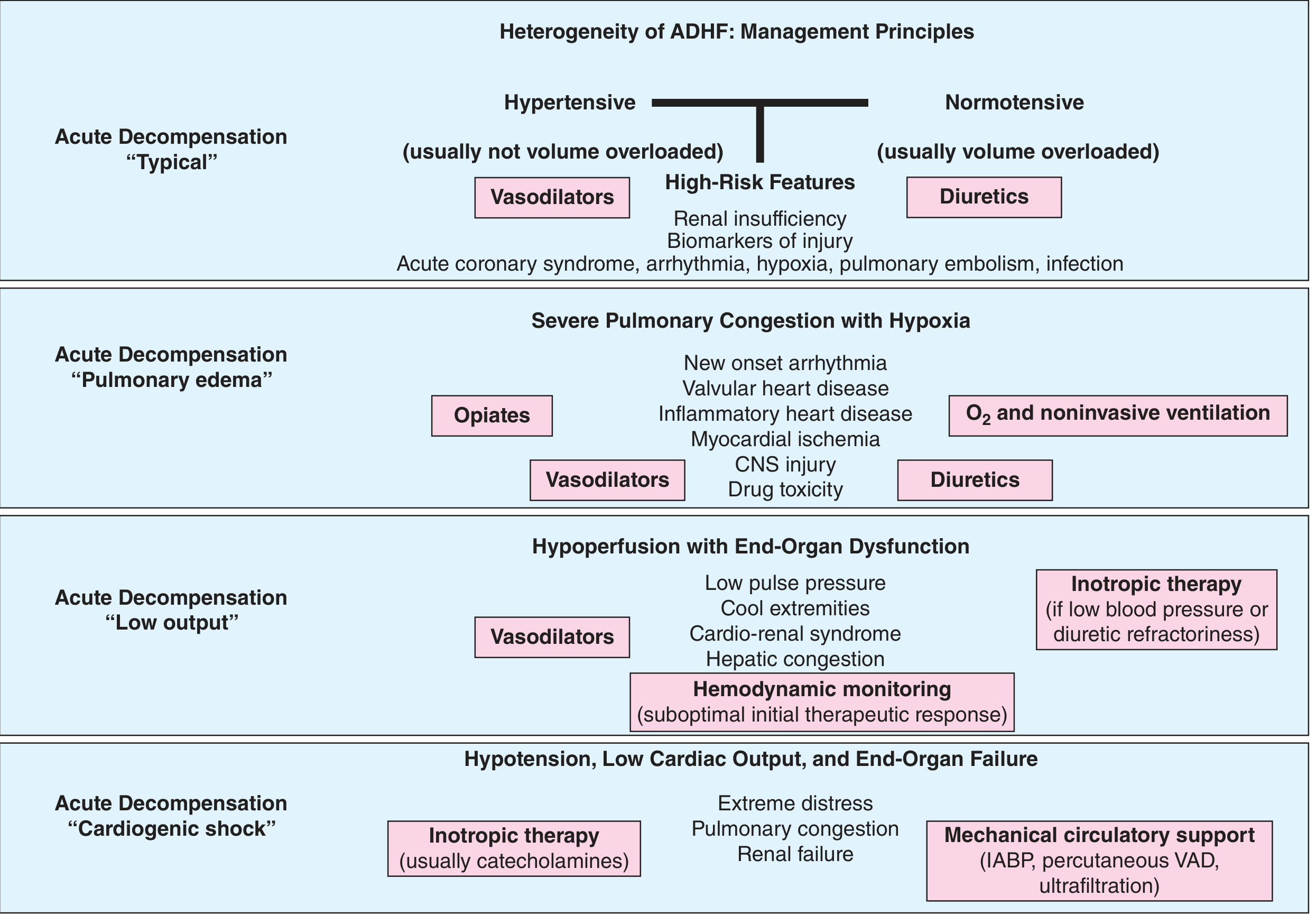
Step 1 - Immediate stabilization
- Sit upright (reduces preload)
- Supplemental O2 to maintain SpO2 ≥94%
- Noninvasive ventilation (CPAP/BiPAP) if severe pulmonary edema / respiratory distress
Step 2 - Pharmacotherapy
| Drug | Dose | Rationale |
|---|---|---|
| IV Furosemide | 40 mg IV (or 1-2.5x oral dose) | First-line decongestant; bolus vs infusion - no clear difference in trials |
| IV Nitrates (GTN/nitroglycerine) | SL or IV infusion | Vasodilator of choice in hypertensive ADHF - reduces preload AND afterload, relieves dyspnea, lowers BP |
| IV Nitroprusside | If severe hypertensive emergency | More potent vasodilator for refractory hypertension |
- For diuretic resistance: add metolazone or chlorothiazide (sequential nephron blockade) - watch for hypokalemia
- Avoid: ACEi/ARB/beta-blocker initiation during acute decompensation if hemodynamically unstable
Step 3 - Monitor response
- Weight daily (surrogate for fluid status)
- JVP, edema, pulmonary crackles normalization
- Urine output >0.5 mL/kg/hr
- Renal function (cardiorenal syndrome in ~30%)
- Pre-discharge BNP/NT-proBNP - elevated level at discharge = high readmission risk
Step 4 - Address precipitants
Per Harrison's 22e, always identify and treat:
- Medication non-adherence
- Dietary indiscretion (salt)
- Concurrent infection
- AF or other arrhythmia
- Myocardial ischemia (ECG, troponins, stress test)
- Valvular disease (echo)
Discharge and Long-Term Management
| Drug Class | Agent | Indication |
|---|---|---|
| ACE inhibitor/ARB/ARNi | Ramipril, Sacubitril-valsartan | BP control, neurohormonal blockade |
| Beta-blocker | Metoprolol, Carvedilol | After euvolemia achieved |
| MRA | Spironolactone | If HFrEF or HFpEF with persistent congestion |
| Loop diuretic | Oral furosemide/torsemide | Maintenance decongestion |
| SGLT2i | Empagliflozin/Dapagliflozin | Proven mortality benefit in both HFrEF and HFpEF |
Salt restriction (<2g/day), fluid restriction, daily weight monitoring, and BP targets (<130/80 mmHg) are essential.
Differential Diagnoses to Consider
| Diagnosis | Features distinguishing from HF |
|---|---|
| Pulmonary embolism | Sudden dyspnea, pleuritic pain, DVT, D-dimer, CTPA |
| Bilateral pleural effusion (non-cardiac) | Hepatic/renal cause; BNP normal |
| Pneumonia | Fever, cough, consolidation on CXR, WBC elevated |
| CKD with fluid overload | Uremic symptoms, frothy urine, very elevated creatinine |
| Hypertensive emergency with pulmonary edema | Severe HTN + organ damage |
Key Prognostic Markers (ADHF)
Parameters associated with worse outcomes (Harrison's 22e):
- BUN >43 mg/dL
- Systolic BP <115 mmHg at presentation
- Creatinine >2.75 mg/dL
- Elevated troponins and natriuretic peptides
- Residual congestion at discharge
The 30-day readmission rate for ADHF is nearly 25%, and 1-year combined CV events reach 50% - making thorough in-hospital management and post-discharge follow-up critical.
Sources: Harrison's Principles of Internal Medicine 22e; Brenner & Rector's The Kidney; Fuster & Hurst's The Heart, 15th Ed.
This is a shared conversation. Sign in to Orris to start your own chat.