CA breast with ulceration and fungation Explainanatomy of breast in detail also
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
Finding Sources
Reading File
I now have comprehensive data. Let me compile the complete answer.
Carcinoma Breast with Ulceration & Fungation + Detailed Breast Anatomy
PART 1: ANATOMY OF THE BREAST (Detailed)
1. Position and Surface Anatomy
The female breast lies between the skin and the superficial pectoral fascia, overlying the pectoralis major muscle. It extends:
- Vertically: from rib II to rib VI along the midclavicular line
- Horizontally: from the lateral sternal border to the midaxillary line
- The breast overlies the pectoralis major, serratus anterior, and external oblique muscles
- The superolateral extension around the lower border of the pectoralis major into the axilla is the axillary tail (of Spence)
(Gray's Anatomy for Students; THIEME Atlas of Anatomy)
2. Structural Layers (Superficial to Deep)
| Layer | Details |
|---|---|
| Skin | Thin, contains hair follicles, sebaceous glands, modified sweat glands (areola) |
| Subcutaneous fat | Envelops the glandular tissue |
| Glandular parenchyma | 15-20 lobes of glandular tissue |
| Cooper's ligaments | Fibrous septa suspending breast from dermis to deep fascia |
| Retromammary space | Loose areolar tissue allowing breast mobility over pectoral fascia |
| Superficial pectoral fascia | Defines posterior border of breast |
| Pectoralis major muscle | Deep to the breast |
The retromammary space (also retromammary bursa) is a potential space between the breast and the deep fascia; when this is obliterated by tumor invasion, the breast becomes fixed to the chest wall - a sign of locally advanced disease.
(Sabiston Textbook of Surgery)
3. Parenchyma - Glandular Architecture
The mature breast is composed of three principal tissue types:
- Glandular epithelium - predominant in adolescents
- Fibrous stroma - interlobular (dense) and intralobular (loose, specialized)
- Adipose tissue - predominant in postmenopausal women
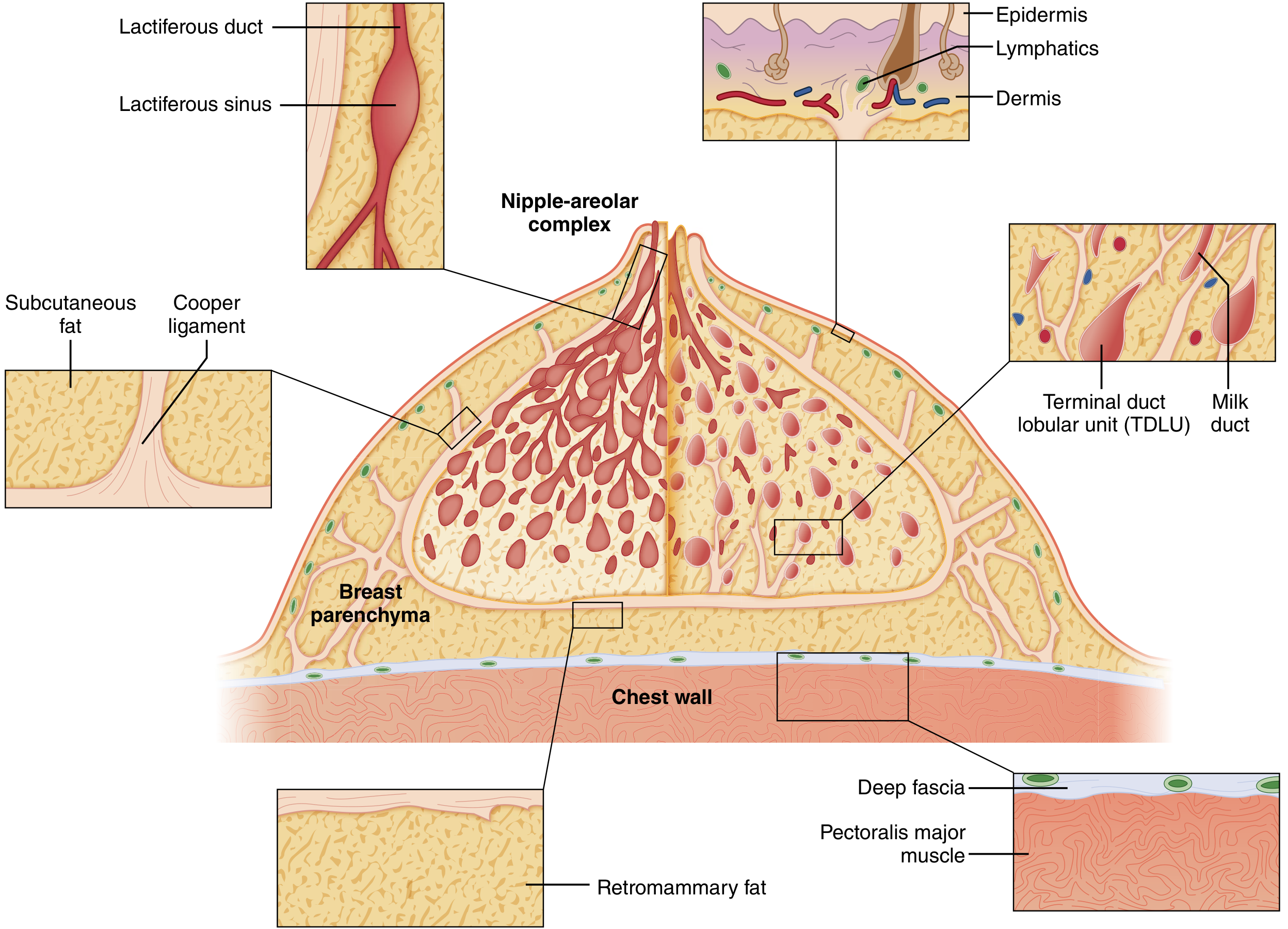
Duct system (configured like an inverted tree):
- 15-20 lobes, each ending in a lactiferous duct opening at the nipple
- Each duct has a dilated portion (the lactiferous sinus) just beneath the nipple-areolar complex (NAC)
- Ducts branch progressively outward, terminating in terminal duct lobular units (TDLUs)
- TDLUs are the basic secretory unit and the site where most breast malignancies originate
Duct epithelium:
- Inner layer: luminal epithelial cells
- Outer layer: myoepithelial cells (contractile - propel milk toward nipple)
- Surrounded by a continuous basement membrane (laminin, type IV collagen, proteoglycans)
- Basement membrane breach = the boundary between DCIS and invasive carcinoma
(Sabiston Textbook of Surgery; THIEME Atlas)
Here is the classic cutaway diagram of the mature breast:
4. Nipple-Areolar Complex (NAC)
- The nipple is a cylindrical projection; contains 15-20 lactiferous duct openings
- Areola: pigmented skin surrounding the nipple, contains:
- Montgomery's glands (modified sebaceous glands, seen as small elevations = Montgomery's tubercles)
- Smooth muscle fibers that cause nipple erection
- Rich in sebaceous and sweat glands
- The NAC is richly invested with lymphatics (Sappey's subareolar plexus)
5. Cooper's Ligaments (Suspensory Ligaments)
Multiple fibrous bands running from the chest wall/deep fascia to the dermis. They:
- Provide structural support and shape to the breast
- Are anchored into the skin - when infiltrated by cancer, they cause skin dimpling
- Edema or cancer infiltration of Cooper's ligaments produces the characteristic "peau d'orange" (orange-peel skin) appearance
(Sabiston Textbook of Surgery)
6. Blood Supply
| Source | Branches | Territory |
|---|---|---|
| Internal thoracic (mammary) artery | 2nd, 3rd, 4th perforating branches (medial mammary branches) | Medial breast (largest contribution - ~60%) |
| Lateral thoracic artery (branch of axillary) | Lateral mammary branches | Lateral and upper breast |
| Thoracoacromial artery (branch of axillary) | Pectoral branch | Upper breast |
| Posterior intercostal arteries | 2nd-5th mammary branches | Lateral breast |
The principal blood supply enters the breast supero-laterally.
Venous drainage follows the arteries - into the internal thoracic vein, lateral thoracic vein, and axillary vein. The axillary vein is particularly important; Batson's vertebral venous plexus connects to this system, providing a hematogenous route for vertebral/CNS metastasis.
(THIEME Atlas; Schwartz's Principles of Surgery; Fischer's Mastery of Surgery)
7. Nerve Supply
Sensory innervation has a segmental arrangement:
- Lateral and medial mammary branches of intercostal nerves T2-T6
- Supraclavicular nerves (branches of cervical plexus C3, C4) - supply upper breast
- The lateral cutaneous branch of T4 (intercostal) carries sensation from the nipple-areolar complex - this is clinically important in nipple-sparing mastectomy
- Sympathetic fibers innervate blood vessels and smooth muscle of nipple/areola
8. Lymphatic Drainage (Clinically Most Important)
Lymphatic channels are abundant in both breast parenchyma and dermis. The collecting point beneath the NAC is Sappey's subareolar plexus (described in 1885).
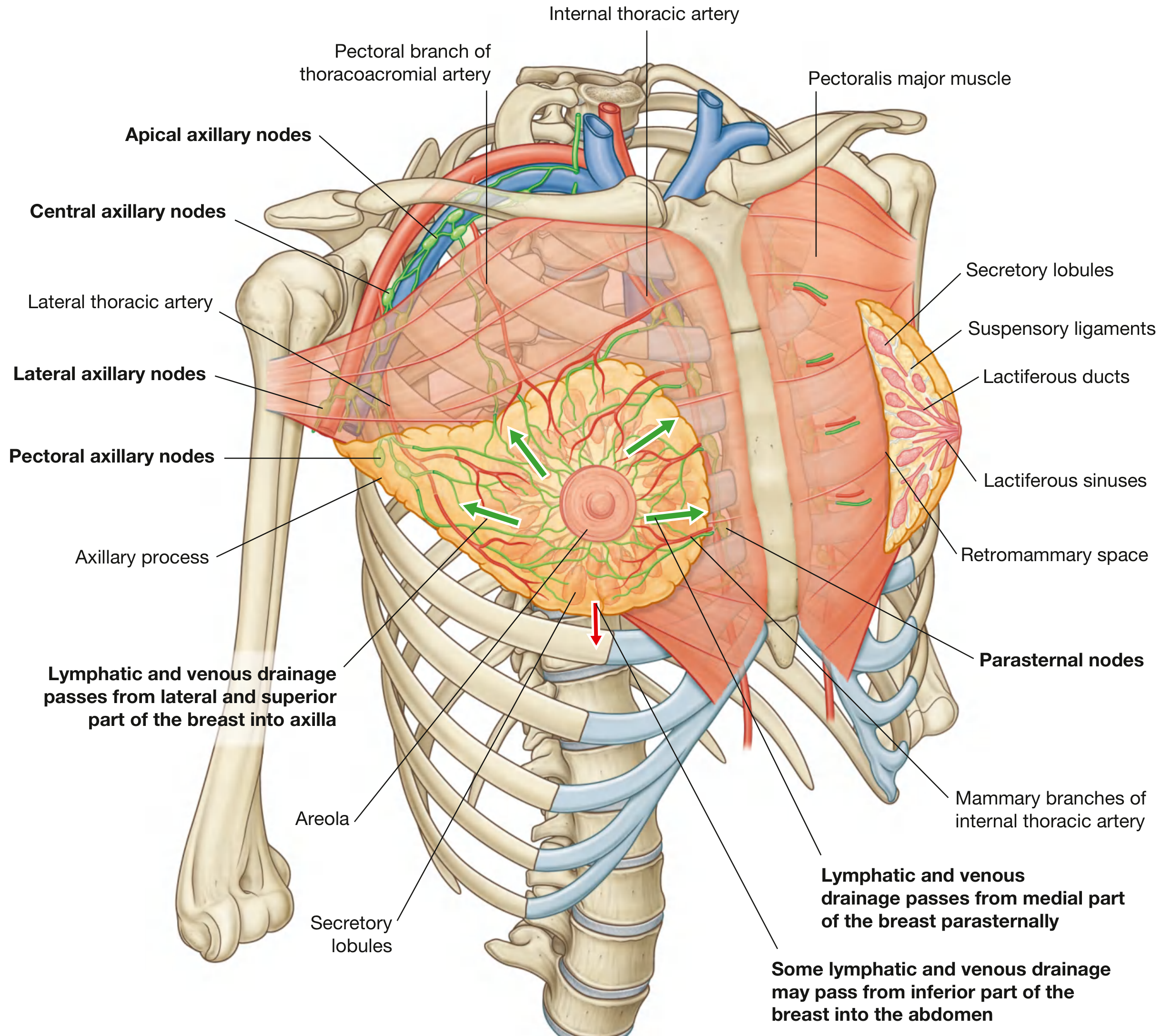
Routes of drainage:
| Route | % of flow | Destination |
|---|---|---|
| Axillary lymph nodes | 70-80% | Via lateral and superior lymphatics |
| Internal mammary (parasternal) nodes | 20% (secondary), 2-3% (primary) | Via medial lymphatics through pectoralis |
| Intercostal nodes | Minor | Via posterior intercostal lymphatics |
| Inferior route | Rare | May drain to abdominal/subdiaphragmatic nodes |
Axillary nodal levels (defined by relationship to pectoralis minor):
| Level | Location | Nodes |
|---|---|---|
| Level I (lower) | Lateral to lateral border of pectoralis minor | Pectoral (anterior), subscapular (posterior), lateral, paramammary |
| Level II (middle) | Posterior to / at level of pectoralis minor | Central, Interpectoral (Rotter's nodes) |
| Level III (upper / infraclavicular) | Medial to medial border of pectoralis minor | Apical nodes |
From Level III, drainage continues to supraclavicular nodes and then into the subclavian lymphatic trunk.
Prognostic significance (THIEME Atlas):
- Level I involvement: ~65% 5-year survival
- Level II involvement: ~31% 5-year survival
- Level III involvement: approaches 0% 5-year survival
This is why sentinel lymph node biopsy (SLNB) is the cornerstone of axillary staging.
(Sabiston; THIEME Atlas; Gray's Anatomy for Students)
PART 2: CARCINOMA BREAST WITH ULCERATION AND FUNGATION
Definition and Pathological Basis
Fungation is the protrusion of tumor tissue through the overlying skin, producing an exophytic, ulcerating, malodorous mass. It represents locally advanced (Stage T4) breast carcinoma.
Mechanism (S. Das - Manual on Clinical Surgery):
"Fungation of the skin is a late feature of advanced carcinoma of the breast due to infiltration of the skin by the growth. The skin becomes infiltrated, its blood supply is compromised, pressure necrosis sets in, the skin breaks down, and the tumor fungates outward."
This is distinct from:
- Fungation in large fibroadenoma or sarcoma - here the skin is NOT infiltrated but becomes atrophic from pressure, then gives way. A probe can be passed under the skin margin in this case (skin not adherent). In carcinoma, the skin IS infiltrated - a probe cannot be passed underneath the margin.
TNM Staging (AJCC 8th Edition - Bailey & Love)
| Category | Criteria |
|---|---|
| T4a | Extension to chest wall (pectoralis muscle invasion alone does not qualify) |
| T4b | Ulceration and/or ipsilateral macroscopic satellite nodules and/or edema (peau d'orange) of skin - does not meet criteria for inflammatory carcinoma |
| T4c | T4a + T4b combined |
| T4d | Inflammatory carcinoma - peau d'orange + redness involving >1/3 of breast surface |
Ulceration/fungation = T4b (minimum); if chest wall involved = T4c.
Overall stage: Stage IIIB (T4b, N0-N3, M0) or Stage IV if distant metastases present.
Clinical Features of Ulceration & Fungation
Inspection findings (S. Das):
- Ulcer anywhere on the breast skin - may be central over the mass or peripheral
- Fungating growth protruding through the skin
- Destruction of the nipple (if fungation involves the NAC)
- Associated features of locally advanced disease:
- Peau d'orange (lymphedema of dermal lymphatics)
- Skin nodules (satellite/metastatic skin deposits)
- Nipple retraction or destruction
- Edema and erythema
Here is a clinical photograph of advanced fungating breast carcinoma:
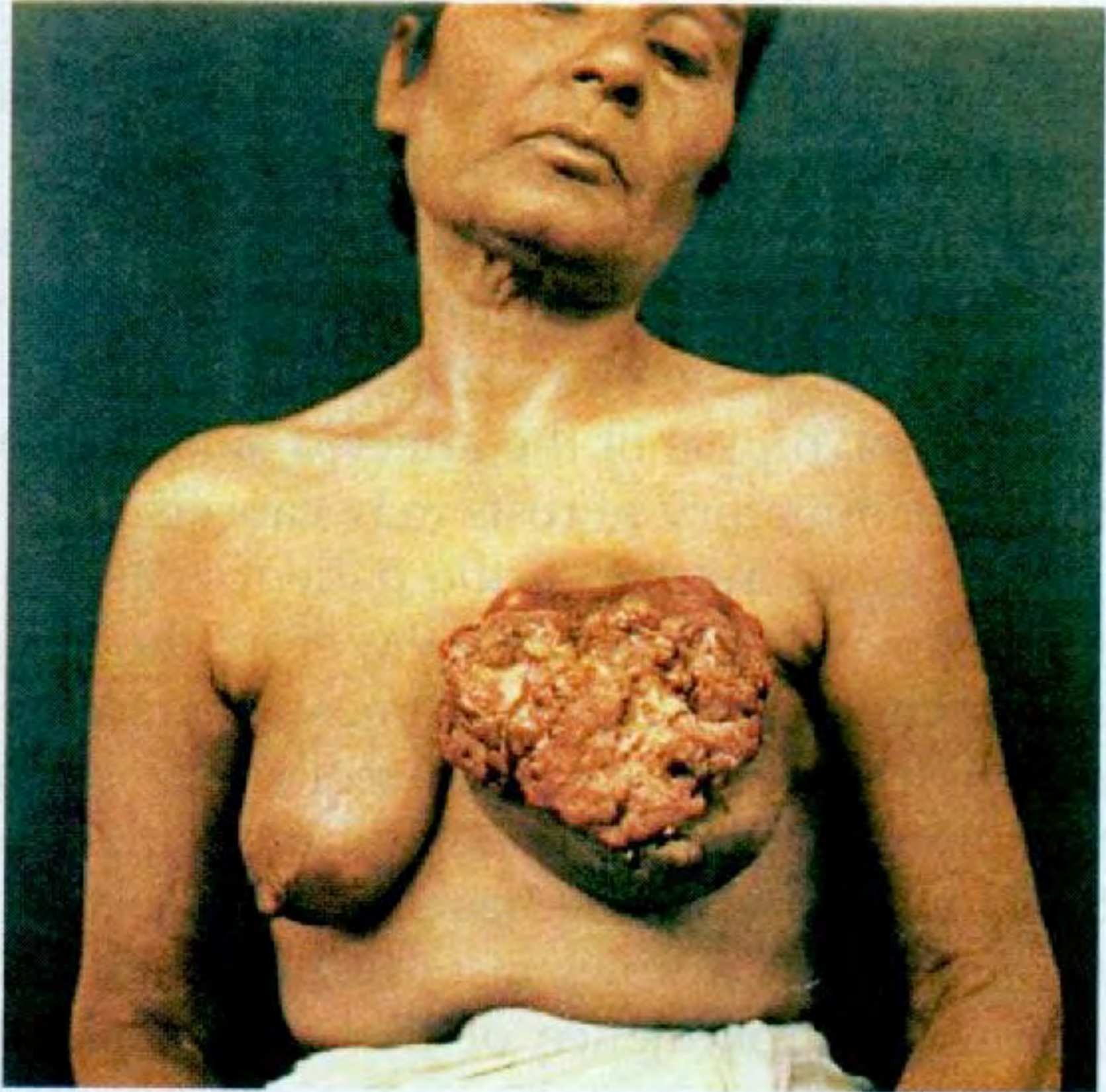
(S. Das - A Manual on Clinical Surgery, 13th Edition)
Peau d'Orange - Mechanism
When tumor cells infiltrate the dermal lymphatics, lymph flow is obstructed. The skin becomes edematous and thickened. Because hair follicles and sebaceous glands tether the skin to the dermis, they remain fixed while the surrounding skin swells, producing the characteristic orange-peel dimpling. This is the hallmark of dermal lymphatic involvement by carcinoma.
- Localized peau d'orange = T4b
- Involving >1/3 of breast surface + redness/warmth = Inflammatory carcinoma (T4d)
Examination of an Ulcer in Breast Carcinoma (S. Das)
When examining any ulcer on the breast:
- Site - over the tumor, or elsewhere on the breast
- Edge - everted (carcinomatous ulcer has everted, indurated edges)
- Floor - sloughy, necrotic, malodorous; may have bleeding granulation tissue
- Base - indurated, hard, fixed to underlying structures
- Probe test - probe CANNOT be passed under the skin margin (skin is infiltrated) - distinguishes fungating carcinoma from benign fungation (fibroadenoma/sarcoma)
- Surrounding skin - satellite nodules, peau d'orange, erythema
- Discharge - serous, bloody, or infected (malodorous)
Management of Locally Advanced Breast Cancer (T4) with Ulceration
Goals: Systemic disease control + local wound/symptom management
1. Systemic Therapy (primary treatment):
- Neoadjuvant chemotherapy - for HER2-positive tumors, triple-negative, node-positive, or premenopausal women
- Regimens: AC-T (anthracycline + cyclophosphamide, followed by taxane)
- HER2+: add trastuzumab + pertuzumab
- Neoadjuvant hormonal therapy - for elderly/frail with ER/PR+ disease (3-6 months)
- Response is assessed at 3 weeks after initiation
2. Surgical Treatment:
- Modified radical mastectomy (MRM) is standard if disease becomes resectable after neoadjuvant therapy
- Primary closure may require skin grafting or flap reconstruction if ulceration is extensive
- Palliative "toilet mastectomy" (fungating mastectomy) for symptom control - removes malodorous, infected fungating mass even when cure is not possible
- Axillary dissection (Level I-III) if clinically node positive
3. Radiation Therapy:
- Postmastectomy radiation to chest wall + regional nodes
- May be used as primary treatment in inoperable cases for local control
4. Local Wound Care (Palliative):
- Regular dressings with activated charcoal dressings for odor
- Metronidazole gel (topical) - for anaerobic bacterial odor control
- Debridement of necrotic tissue
- Hemostatic measures for bleeding (silver nitrate, alginate dressings)
- Adequate analgesia
5. Prognosis:
- T4b with nodal disease (Stage IIIB): 5-year survival ~40-50% with multimodal therapy
- Presence of distant metastases: palliative intent only
Key Differential Diagnosis - Causes of Breast Ulceration
| Cause | Key Feature |
|---|---|
| Carcinoma (commonest) | Hard, infiltrated base; skin fixed; probe test negative |
| Large fibroadenoma/phyllodes | Skin attenuated but NOT infiltrated; probe passes under margin; soft mass |
| Sarcoma (rapidly growing) | Similar to benign - skin not infiltrated |
| Paget's disease | Nipple erosion; eczema-like, nipple may be destroyed |
| Inflammatory carcinoma | Diffuse erythema, warmth, peau d'orange >1/3 breast |
| Tuberculosis of breast | Rare; indolent; may discharge caseous material |
Sources:
- S. Das - A Manual on Clinical Surgery, 13th Edition
- Sabiston Textbook of Surgery, Biological Basis of Modern Surgical Practice
- Bailey and Love's Short Practice of Surgery, 28th Edition
- THIEME Atlas of Anatomy - General Anatomy and Musculoskeletal System
- Gray's Anatomy for Students
- Fischer's Mastery of Surgery, 8th Edition
- Schwartz's Principles of Surgery, 11th Edition
This is a shared conversation. Sign in to Orris to start your own chat.