BONE HEALING - relative and absolute stability
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Reading File
Reading File
Finding Sources
Reading File
Reading File
I now have a very comprehensive dataset from multiple authoritative sources. Let me compile the full answer.
Bone Healing: Relative vs. Absolute Stability
The mechanical environment at the fracture site is the single most important determinant of which healing pathway is activated. The two pathways have directly opposing mechanical requirements - a fixation strategy aimed at one will suppress the other.
The Perren Strain Theory (Foundation)
Strain = change in fracture gap / fracture gap length (ΔL/L)
This defines which tissue can tolerate the mechanical environment:
| Strain Level | Tissue Formed | Healing Type |
|---|---|---|
| < 2% | Bone | Primary (direct) bone healing |
| 2% - 10% | Cartilage → soft callus | Secondary (indirect) bone healing |
| > 10% | Fibrous tissue only | No bone formation possible |
| > 60% | Tissue rupture / nonunion | Healing failure |
- Strain is highest at a simple fracture fixed with a gap (incompletely reduced)
- Strain decreases as callus matures and stiffens - this is the self-regulating mechanism of secondary healing
Absolute Stability → Primary (Direct) Bone Healing
Mechanical Requirements
- No motion at the fracture site under physiologic load
- Interfragmentary motion must remain < 0.15 mm; fracture strain < 2-5%
- Requires anatomic reduction with interfragmentary compression
- No gap at the fracture site (cutting cones cannot cross gaps)
Biological Process
Primary bone healing bypasses the intermediate stages (hematoma, callus) and proceeds directly to the remodeling stage:
- Contact healing: Osteoclast "cutting cones" cut directly across the fracture line; osteoblasts trail behind and lay down new lamellar bone parallel to the long axis
- Gap healing: At sites with microscopic residual gaps, lamellar bone is laid down perpendicular to the bone axis, then remodeled by secondary cutting cones parallel to the axis. This bone is less well-anchored and weaker than contact-healed bone.
Key Features
- No periosteal callus - healing is radiographically invisible (a major pitfall)
- Healing is a slower process than callus healing
- Early plate removal risks refracture through the original fracture site - plate removal should be delayed up to 2 years
- Implants must have a longer fatigue life because they carry load for the full duration
- The process is highly sensitive to even small amounts of motion or any residual gap
Clinical Indications
- Intra-articular fractures - anatomic reduction is mandatory to prevent posttraumatic arthritis; absolute stability is the preferred strategy
- Simple diaphyseal fractures amenable to compression plating (short oblique/transverse)
- Requires removal of the fracture hematoma to achieve interfragmentary compression (a biologic tradeoff)
Devices Achieving Absolute Stability
- Lag screws (oblique fractures)
- Compression plating (transverse fractures)
- Dynamic compression plates (DCP) applied with compression technique
Relative Stability → Secondary (Indirect) Bone Healing
Mechanical Requirements
- Controlled micromotion at the fracture site under physiologic load
- Strain approximately 2-10% (soft callus range)
- Does NOT require anatomic reduction of individual fragments - requires restoration of length, alignment, and rotation
- Preserves the fracture hematoma (biologic advantage)
Biological Process - 4 Stages
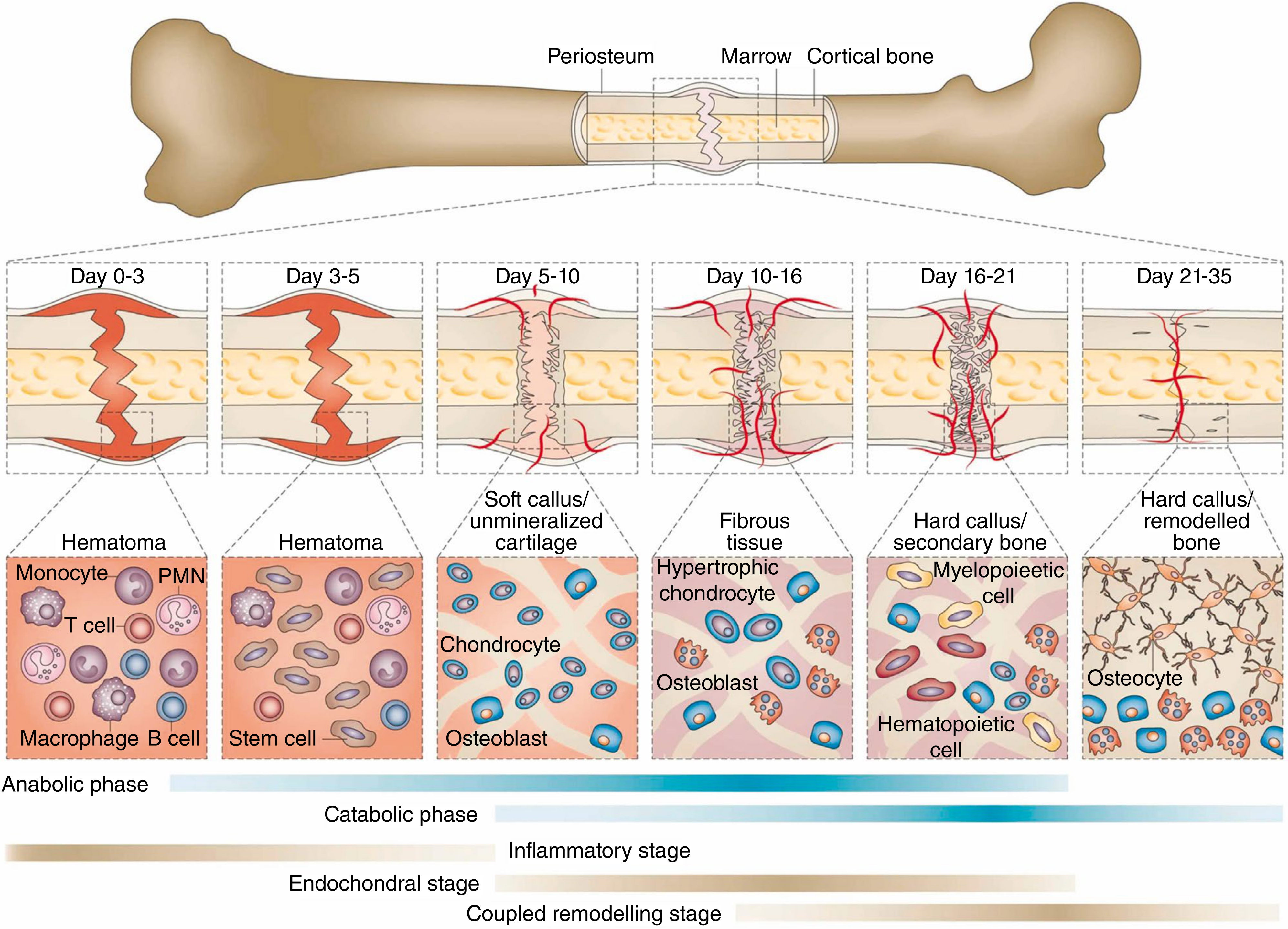
Stage 1 - Hematoma formation (Day 0-3): Rupture of blood vessels fills the fracture gap. Monocytes, T cells, macrophages, B cells invade. The hematoma forms the initial scaffold; inflammatory cells begin lysosomal degradation of necrotic tissue.
Stage 2 - Granulation tissue / Soft callus (Day 3-10): Pluripotential mesenchymal/stem cells invade and differentiate into fibroblasts, chondroblasts, and osteoblasts. Angiogenesis occurs within periosteal tissue and marrow. A cartilaginous soft callus forms around the fracture site.
Stage 3 - Hard callus (Day 10-21): The cartilaginous callus undergoes endochondral ossification (replaced by woven bone). Osteoblasts and hypertrophic chondrocytes are prominent. Calcified callus of immature woven bone forms.
Stage 4 - Remodeling (Day 21 onward, lasting months-years): Woven bone is replaced by lamellar bone. The medullary canal is restored. Bone is returned to near-normal morphology and mechanical strength.
The self-regulating mechanism: As callus matures and spreads out around the fracture, it reduces local strain - this is why secondary healing is self-stabilizing. The system progressively stiffens until primary bone healing conditions are met and remodeling can complete.
Direction of Motion Matters
- Axial micromotion - stimulates callus formation (desirable)
- Shear motion - inhibits callus formation (harmful). Bridge plates with long working lengths can induce up to 3x more shear than axial motion - an important construct consideration.
Key Features
- Callus is visible on radiograph - provides clinical confirmation of healing
- More forgiving environment than absolute stability - works across a wide range of fracture patterns including comminuted fractures where anatomic reduction is impossible
- Intramedullary nails have inherently low axial stiffness but can be tuned for torsional rigidity
- Faster and stronger healing compared to primary bone healing in experimental models
Clinical Indications
- Diaphyseal and metaphyseal fractures
- Comminuted fractures (where anatomic reduction is impossible/undesirable)
- Femoral, tibial shaft fractures
Devices Achieving Relative Stability
- Intramedullary (IM) nails - preferred; inherently low stiffness, high strength
- Bridge plates (biological plating)
- External fixators
- Functional bracing/casts
Key Comparison Table
| Feature | Absolute Stability | Relative Stability |
|---|---|---|
| Fracture site motion | Zero (< 0.15 mm) | Controlled micromotion |
| Strain | < 2% | 2-10% |
| Reduction required | Anatomic | Functional (length/alignment/rotation) |
| Healing type | Primary/direct | Secondary/indirect |
| Callus | None | Prominent periosteal callus |
| Ossification type | Intramembranous (osteonal remodeling) | Endochondral |
| Radiographic monitoring | Difficult (invisible) | Easy (visible callus) |
| Healing speed | Slower | Faster |
| Hematoma | Removed (for compression) | Preserved |
| Fracture type best suited | Intra-articular, simple diaphyseal | Comminuted, diaphyseal/metaphyseal |
| Implants | Lag screws, compression plates | IM nails, bridge plates, ex-fix, casts |
Critical Pitfall: Never Mix Strategies
"Attempting to mix the direct and callus healing strategies will not properly support either mode of healing and result in a nonunion." - Rockwood & Green's Fractures in Adults, 10th Ed.
A classic error is combining an interfragmentary lag screw (aiming for absolute stability) with a relatively stable construct (e.g., bridge plate or external fixator). The lag screw compresses the fracture, preventing callus formation, but the overall construct remains too flexible to achieve the motion-free environment needed for primary healing.
Nonunion: When Stability Fails
- Hypertrophic nonunion: Too much motion - callus keeps forming to try to stabilize the fracture but fails to bridge. Radiograph shows abundant callus with no bridging. Treatment: increase stability.
- Atrophic nonunion: Overly stiff construct with a residual fracture gap - insufficient motion to stimulate callus, no biology to drive primary healing. Treatment: improve biology (bone grafting, muscle flap) + address mechanical environment.
Sources:
- Rockwood and Green's Fractures in Adults, 10th ed. 2025 (blocks 1, 5)
- Miller's Review of Orthopaedics, 9th ed.
- Bailey and Love's Short Practice of Surgery, 28th ed.
- Campbell's Operative Orthopaedics, 15th ed. 2026
This is a shared conversation. Sign in to Orris to start your own chat.