Ischemic Colitis Definition & Epidemiology Causes & Risk Factors Watershed Areas of the Colon Clinical Features Investigations Medical Management Surgical Management Prognosis
Reading File
Finding Sources
Searching PubMed
"ischemic colitis"[MeSH Terms] AND management
Searching Images
ischemic colitis watershed areas colon anatomy
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Reading File
Loading Image
Loading Image
I now have all the material needed to compile a comprehensive, well-structured response. Let me synthesize everything.
Ischemic Colitis
Definition & Epidemiology
Ischemic colitis (IC) is a condition in which arterial blood supply to the colonocytes is insufficient to meet metabolic demands. It is the most common form of gastrointestinal ischemia. Injury can occur at two phases: during the initial ischemic insult and/or after reperfusion. Reperfusion injury is mediated by reactive oxygen species causing lipid peroxidation and cell necrosis.
- Mucosal-only injury → potentially reversible
- Transmural injury → life-threatening; leads to stricture, perforation, sepsis, and death
Epidemiology:
- Incidence: 4.5–44 cases per 100,000 persons/year (true incidence likely higher due to mild, unrecognized cases; Sabiston cites 7.1–22.9/100,000 person-years)
- Predominantly affects patients >60 years old
- Higher prevalence in women
- ~20% of patients require operative intervention, usually emergent
- Incidence is rising given the growing elderly population
Causes & Risk Factors
IC is classified by mechanism:
| Mechanism | Examples |
|---|---|
| Non-occlusive (most common) | Shock, low-flow states, drugs, colon obstruction |
| Arterial thrombosis/embolism | Atherosclerosis, hypercoagulable states |
| Venous occlusion | Rare |
| Postoperative | Aortic/cardiac surgery, IMA sacrifice |
Box: Conditions & Drugs Associated with Ischemic Colitis (Sabiston, 21st ed.)
| Category | Examples |
|---|---|
| Low-flow states | Septic shock, congestive heart failure, hemorrhagic shock, hypotension |
| Atherosclerosis | Ischemic heart disease, cerebrovascular disease, peripheral vascular disease |
| Cardiovascular/Pulmonary | Atrial fibrillation, hypertension, COPD |
| Metabolic/Rheumatologic | DM, dyslipidemia, SLE, rheumatoid arthritis |
| Gastrointestinal | Constipation, IBS, bowel obstruction |
| Surgery/Invasive procedures | Aortic surgery (especially AAA repair), cardiac surgery, chemoembolization, post-colonoscopy |
| Miscellaneous | Hypercoagulable states, sickle cell disease, long-distance running, COVID-19 |
| Drugs | Cocaine/methamphetamines, oral contraceptives, NSAIDs, opioids, immunomodulatory drugs, digoxin, diuretics |
Pathophysiology note: During hypotension, blood is redistributed to the brain at the expense of the splanchnic circulation. Mucosal injury develops within 20 minutes to 1 hour of decreased blood flow; transmural infarction occurs within 8–16 hours.
Watershed Areas of the Colon
The colon's arterial supply comes from the SMA (ileocolic, right colic, middle colic arteries) and the IMA (left colic, sigmoidal arteries, superior rectal artery). Two collateral networks exist:
- Marginal artery of Drummond — runs parallel to the mesenteric margin from cecocolic to rectosigmoid junction (absent at the splenic flexure in up to 18–50% of individuals)
- Arc of Riolan (meandering mesenteric artery) — connects SMA/middle colic to IMA/left colic; its presence signals a major mesenteric artery occlusion
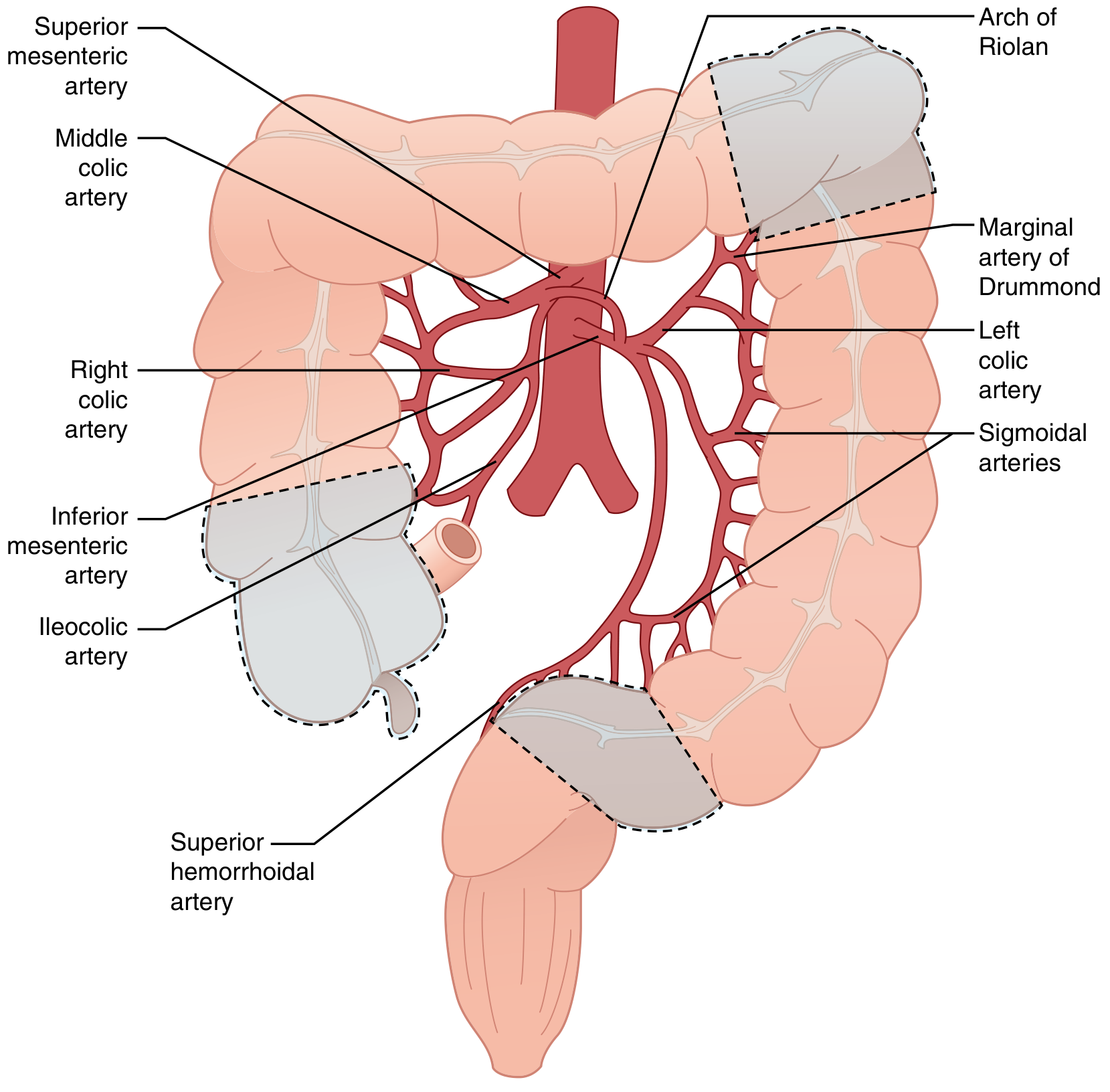
Colonic blood supply showing the two watershed areas (dashed outlines): splenic flexure and rectosigmoid/cecal regions. — Sabiston Textbook of Surgery
Two classic watershed zones (together account for ~80% of IC cases):
| Zone | Location | Vessels involved | Eponym |
|---|---|---|---|
| 1st watershed | Splenic flexure | Junction of SMA (middle colic) & IMA (left colic) | Griffith's point |
| 2nd watershed | Rectosigmoid junction | Junction of IMA (sigmoid) & superior rectal artery | Sudeck's point |
The rectum is relatively spared due to its rich collateral supply (inferior/middle rectal arteries from the internal iliac system).
Special entity — Isolated Right-Sided Colon Ischemia (IRCI):
- Associated with acute mesenteric ischemia of larger vessels
- 30-day mortality 20.3% vs. 9.0% in non-IRCI
- Requires urgent CT angiography to exclude proximal SMA occlusion
Clinical Features
Presentation is often vague and delayed while other diagnoses are excluded.
Classic triad:
- Acute onset abdominal pain (cramping, usually left-sided)
- Hematochezia (bright red blood per rectum)
- Urgent desire to defecate
Severity spectrum:
| Severity | Features |
|---|---|
| Mild (mucosal) | Diarrhea (often bloody), minimal pain; self-limiting |
| Moderate | Significant abdominal pain, tenderness, fever, leukocytosis |
| Severe (transmural/gangrenous) | Increasing tenderness, guarding, rebound, rising temperature, paralytic ileus, hemodynamic instability |
| Fulminant (rare) | Sudden onset toxic colitis with peritonitis, rapidly progressive |
Note: Rectal bleeding is seen more often in non-IRCI (70%) than IRCI (39%). Patients with IRCI more often present with severe pain without bleeding — high index of suspicion is required.
Investigations
Laboratory Studies
Routine labs are unhelpful for diagnosis but important for prognostication:
- CBC: Leukocytosis (frequent)
- Metabolic panel: Elevated lactate, BUN, creatinine; metabolic acidosis in severe cases
- Haemoglobin: Low Hgb (<12 g/dL) → poor prognostic sign
- Serum albumin: Low albumin → worse prognosis
- Coagulation studies
Poor prognostic laboratory markers: HR >100, SBP <90, Hgb <12, Na <136, LDH >450, BUN >28
Imaging
Plain Abdominal X-ray:
- "Thumbprinting" — rounded densities along gas-filled colon = submucosal oedema (non-specific)
- Free air under the diaphragm → perforation → immediate surgery
CT Abdomen & Pelvis (IV + oral contrast) — primary modality:
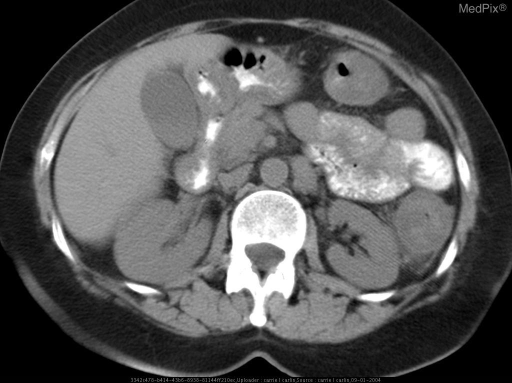
CT abdomen showing segmental wall thickening at the splenic flexure watershed zone, with "target sign" (submucosal oedema) and pericolonic fat stranding — characteristic of ischemic colitis.
| CT Finding | Significance |
|---|---|
| Segmental bowel wall thickening | Mild/moderate ischemia |
| Pericolonic fat stranding | Inflammatory response |
| Thumbprinting | Submucosal oedema |
| Pneumatosis intestinalis | Severe transmural disease → surgery |
| Portal venous gas | Severe transmural disease → surgery |
| Absent colonic wall enhancement | Severe transmural disease → surgery |
CT angiography: Indicated in IRCI or sudden severe pain out of proportion to findings (to exclude acute proximal mesenteric ischemia).
MRI: Alternative to invasive procedures for grading severity (limited acute use).
Endoscopy (Gold Standard)
Flexible colonoscopy is the gold standard — performed within 48 hours except in:
- Acute peritonitis
- Suspected severe transmural ischemia
Precautions: Avoid overinsufflation; do not advance beyond most distal extent of disease.
Endoscopic findings:
- Oedematous, friable mucosa
- Erythema, petechial haemorrhage
- Mucosal ulceration
- "Single-stripe sign" — single linear ulcer along the longitudinal axis (rare but specific for IC)
- Segmental distribution with abrupt transition between injured and normal mucosa
- Rectal sparing (helps distinguish from IBD)
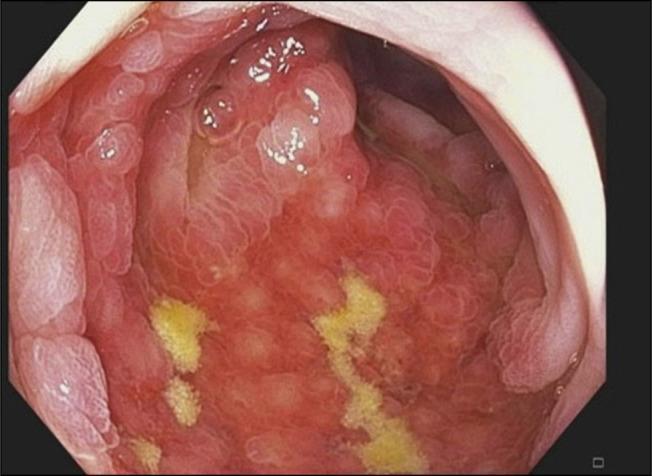
Colonoscopy image showing classic ischemic colitis features at the splenic flexure watershed zone: diffuse erythema, congestion, mucosal oedema, and fibrinopurulent exudates.
Note: Endoscopy cannot reliably distinguish partial-thickness from full-thickness ischemia.
Medical Management
~80% of patients respond to conservative non-operative treatment within a few days.
Mainstay Treatment
- Bowel rest (NPO)
- IV fluid resuscitation — correct low-flow states and hypotension
- Broad-spectrum antibiotics — cover both aerobic and anaerobic coliform bacteria (bacterial translocation is a key complication)
- Nasogastric tube if ileus is present
- Optimise comorbidities — treat heart failure, sepsis, correct coagulopathy
Additional Measures
- Phosphodiesterase-5 inhibitors, pentoxifylline, prostaglandin E1 — may improve colonic blood flow and mucosal healing
- Discontinue offending drugs (vasoconstrictors, oral contraceptives, NSAIDs, etc.)
- Avoid cathartics — risk of perforation
- Avoid glucocorticoids — unless treating underlying SLE or RA
Monitoring for Failure
Repeat imaging or endoscopy if patient fails to improve within 2–3 days or clinical condition worsens — raises concern for full-thickness ischemia.
Surgical Management
Indications for Emergency Surgery
| Indication |
|---|
| Peritonitis on examination |
| Massive/uncontrolled haemorrhage |
| Fulminant colitis |
| Free peritoneal air (perforation) |
| Pneumatosis intestinalis or portal venous gas on CT |
| Worsening clinical condition despite medical management |
| Isolated right-sided colon ischemia (IRCI) — often requires surgery |
| Pancolonic ischemia |
| Haemodynamic instability + abdominal pain without rectal bleeding |
| Gangrenous colitis |
Surgical Principles
- Midline laparotomy (diagnostic laparoscopy in selected cases)
- Assess the entire small and large bowel for ischemia
- Resect all grossly ischemic segments — anatomic resection with adequate blood supply to remaining colon
- Use intraoperative adjuncts for bowel viability assessment:
- Visual inspection (unreliable — serosa appears normal until transmural necrosis)
- Doppler ultrasonography
- Indocyanine green (ICG) infrared angiography — increasingly popular; real-time tissue perfusion assessment
Anastomosis vs. Ostomy
| Situation | Recommendation |
|---|---|
| Uncomplicated isolated right colon ischemia, well-perfused bowel | Primary anastomosis may be safe |
| Left-sided IC (most cases) | Hartmann's procedure — end colostomy + rectal stump; reverse no sooner than 6–8 weeks |
| Selected left-sided cases | Primary anastomosis ± protective diverting loop ileostomy |
| Pancolonic ischemia | Total colectomy with end ileostomy |
| Haemodynamically unstable/evolving ischemia | Leave bowel in discontinuity; planned second-look laparotomy in 12–48 hours |
Primary anastomosis is generally avoided in the acute setting due to risk of evolving ischemia, haemodynamic instability, and sepsis.
Management Algorithm
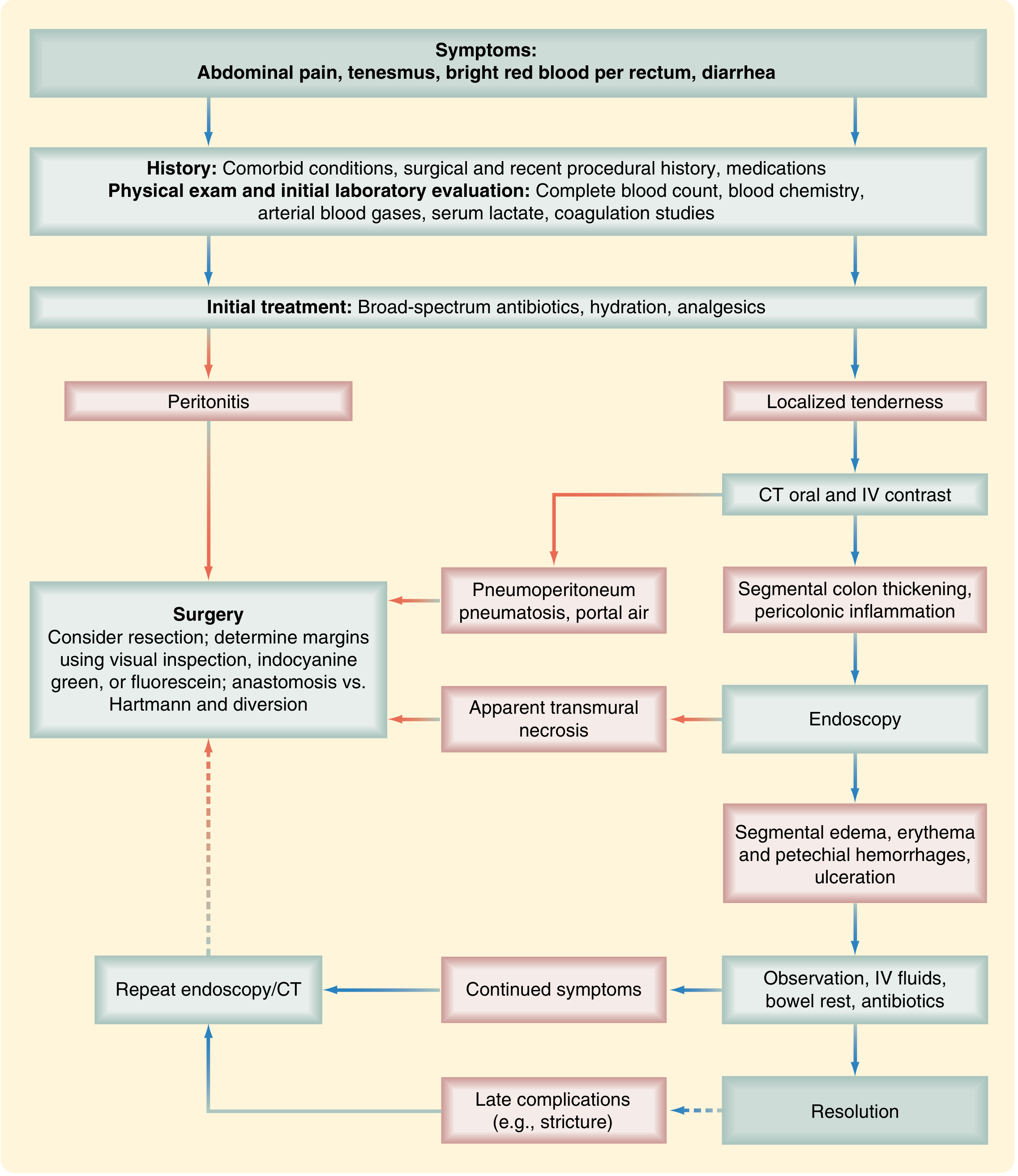
Algorithm for diagnosis and treatment of ischemic colitis. — Sabiston Textbook of Surgery / Current Surgical Therapy
Prognosis
Overall Outcomes
| Outcome | Rate |
|---|---|
| Resolution with medical management | ~80% |
| Require surgical intervention | ~20% |
| Develop stricture (long-term) | 10–15% |
| Develop chronic segmental ischemia | 15–20% |
| 30-day postoperative mortality (surgery for IC) | 25–47% |
| IRCI 30-day mortality | ~20% |
| Non-IRCI 30-day mortality | ~9% |
Late Complications
- Chronic ischemic stricture — presents with constipation, narrow stools, abdominal pain; diagnosed by contrast enema, CT, or endoscopy; requires elective resection if symptomatic or malignancy cannot be excluded
- Chronic relapsing colitis — recurrent bouts of pain, bloody diarrhoea, sepsis; requires surgical resection
Poor Prognostic Indicators
- Isolated right-sided colon ischemia (IRCI) or pancolonic disease
- HR >100 bpm, SBP <90 mmHg
- Haemoglobin <12 g/dL
- Hyponatraemia (Na <136 mEq/L)
- LDH >450 U/L, BUN >28 mg/dL
- Metabolic acidosis / elevated lactate
- Pre-operative septic shock, acute renal failure
- Elderly age, poor functional status, multiple comorbidities
- Delay from hospital admission to surgery
Follow-up
Colonoscopy after recovery is recommended to:
- Evaluate for stricture formation
- Exclude other diagnoses (IBD, malignancy)
Sources:
- Current Surgical Therapy, 14th ed. (Alsaad & Lipsett)
- Sabiston Textbook of Surgery, 21st ed.
- Yamada's Textbook of Gastroenterology, 7th ed.
- Schwartz's Principles of Surgery, 11th ed.
This is a shared conversation. Sign in to Orris to start your own chat.