Intervention radiology in urinary tractrguhs radio pg 20 mark ans
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
I now have very comprehensive content from Grainger & Allison's diagnostic radiology textbook. Let me compile the full 20-mark answer on Interventional Radiology in the Urinary Tract.
Interventional Radiology in the Urinary Tract
20-Mark PG Radiology Answer
(Based on Grainger & Allison's Diagnostic Radiology)
Introduction
The genitourinary (GU) tract is especially prone to anatomical and morphological variations, and successful intervention relies on careful anatomical appreciation and planning. Interventional procedures in the urinary tract span from the renal collecting system down to the bladder and urethra, encompassing drainage, stone clearance, stricture management, embolisation, and denervation.
I. ANATOMICAL BASIS FOR RENAL ACCESS (Essential Foundation)
Renal Position
- Kidneys lie in the perinephric space at T12-L2/L3 level
- Upper pole is more medial and more posterior than the lower pole (coronal axis tilt ~15 degrees)
- Renal pelvis points anteromedially in the short axis
Pelvicalyceal Anatomy
- Adult kidney has ~8-9 calyces; upper and lower pole calyces are often fused (larger, easier to access)
- Posterior calyces are ideal for access - closer to the skin surface, allow straight-line navigation to adjacent calyces or renal pelvis
- Access to the pelviureteric junction (PUJ) and ureter is easier from an interpolar or upper pole calyx
Vascular Anatomy (Brodel's Line)
- Main renal artery divides into anterior (larger) and posterior (smaller) divisions, then segmental and lobar divisions
- Peripheral lobar and arcuate arteries skirt around the calyx in the columns of Bertin - termed the "vascular ring"
- Brodel's bloodless line (posterior avascular plane) runs along the lateral border of the kidney - the safest approach for renal puncture
- A posterior calyx is approached from slightly lateral to posteromedial, thus traversing the relatively avascular zone between anterior and posterior arterial divisions
Safest Puncture Site
- Lower pole, posterolateral puncture of the centre of the calyx is theoretically safest
- Upper pole is more posterior (easier navigation) but must be approached with care to avoid pleural transgression
II. GENERAL EQUIPMENT FOR RENAL ACCESS
| Equipment | Details |
|---|---|
| Needles | 21-G (two-part Seldinger system) or 18-G (one-part system) |
| Guidewires | Bentsen wire (floppy, straight tip) or angled hydrophilic wire for calyx navigation; stiff Amplatz-type wire once in renal pelvis/ureter |
| Catheters | Angled tip (Kumpe) or Cobra shape for navigation; pigtail catheter with large drainage holes for drainage |
| Dilatation | Serial dilators; care to avoid kinks which cause pelvic rupture |
III. PERCUTANEOUS NEPHROSTOMY (PCN)
Indications (Table 85.2 - Key ones)
- Relief of renal obstruction with or without associated infection
- Pyonephrosis / infected hydronephrosis (most urgent)
- Pre-operative or palliative decompression
- Access for subsequent antegrade stenting, PCNL, or nephrolithotripsy
- Treatment of urinary leaks and fistulas
- Urinary diversion in ureteric injury or leak
Timing
- Should ideally be performed within working hours on a stable, well-resuscitated patient
- Must NOT be delayed in suspected pyonephrosis or infected hydronephrosis - urgent decompression is required
Technique
- US guidance is used to identify the collecting system
- Fluoroscopy confirms wire and catheter placement
- Two-part system (21-G initial needle, 0.018-inch platinum-tipped wire, 4-F dilator, then 0.035-inch working wire) OR one-part 18-G diamond point needle
- Ideally puncture the centre of a calyx to stay within the vascular ring
- Navigate wire from calyx into renal pelvis, then down the ureter
- Dilate tract and insert pigtail drainage catheter (>6F); locking pigtail preferred for anchorage
Guidance Modalities
| Method | Technique |
|---|---|
| US-guided (single puncture) | Entire procedure under US; no fluoroscopy or contrast needed - preferred for infected systems |
| Fluoroscopically guided (single puncture) | After initial US puncture, fluoroscopy for wire/catheter positioning |
| Combined US + fluoroscopy | Most common clinical practice |
Special Situations
Paediatric PCN:
- Under general anaesthesia
- System can rapidly decompress on needle entry - catheter must be inserted swiftly
- Stiff 0.035-inch wire inserted directly; no pre-dilatation needed for dilated systems
- Neonatal 5-F catheters available; standard 6-F pigtail also works
- Minimize radiation: low-dose techniques, good collimation
Pregnancy:
- Urolithiasis is the commonest cause of ureteric obstruction
- US-guided procedure preferred; fluoroscopy only if necessary
- Lateral or supine/oblique approach; IV opiates to minimize fetal respiratory depression
- Lead shielding when fluoroscopy is used
Complications of PCN and Management (Table 85.3)
| Complication | Management |
|---|---|
| Sepsis (most common serious complication) | Pre-procedural antibiotics; avoid overdistension and manipulation; delay nephrostogram until recovery |
| Haemorrhage (2nd most serious) | Haematuria for a few days - usually resolves spontaneously |
| Venous bleeding | Catheter tamponade + blood transfusion |
| Arterial bleeding | Prolonged catheter tamponade; if fails - renal angiography and embolisation |
| Renal/pelvic injury | Prolonged internal or external drainage (self-limiting) |
| Bowel injury (rare) | Separate nephrostomy for renal drainage; leave drain in colon; nephrostogram after a few days to exclude renocolic fistula |
Key point on arterial bleeding: Angiography should be performed with the nephrostomy catheter initially in situ; if no bleeding point is seen, withdraw catheter over a guidewire while maintaining access and repeat angiographic images to unmask an occult bleeding point.
IV. PERCUTANEOUS NEPHROLITHOTOMY (PCNL)
- Gold standard for renal stones >2 cm or those not amenable to ESWL/ureteroscopy
- Requires stiff Amplatz-type guidewire and larger tract dilatation
- Upper or interpolar calyx access preferred for better instrument angulation
- Performed under GA; ultrasonic, pneumatic, or laser lithotripsy used intracorporeally
- Post-procedure nephrostomy left for drainage and tamponade
V. ANTEGRADE URETERIC STENTING
Indications
- Ureteric obstruction (benign or malignant stricture)
- Primary stenting or second procedure after several days of external PCN drainage
Ureteric Stents - Versus PCN
| Feature | Ureteric Stent (Double-J) | PCN |
|---|---|---|
| External bag | No | Yes |
| Patient comfort | Better | Worse |
| Risk of infection | Similar | Similar |
| Malignant stricture success | Variable | Usually effective |
| Primary stenting technical success | ~85% | Near 100% (after external drainage) |
Key rule: Primary antegrade stenting is contraindicated in infected obstructed systems - PCN first, then stent later.
Types of Ureteric Stents
Plastic (Double-J / Double Pigtail) Stents:
- Hollow tube with pigtail in renal pelvis and bladder
- Made of modern polymers (better biocompatibility than early polyethylene/polyurethane)
- High encrustation rate - require regular exchange
- Dysuria/urinary frequency in up to 50% of patients
Metal Stents (for long-term, especially malignant strictures):
- Wallstent (conventional) - becomes permanently incorporated via urothelial epithelialisation; NOT ideal for ureter
- Uventa / Allium stents - NiTiNol mesh with PTFE or polymer covering
- Memokath stent - uncovered NiTiNol wire spiral
- Modern metallic stents do not become incorporated; some are removable even after several years
Pathological Changes After Stenting
- All stents cause reactive urothelial hyperplasia, thickened mucosa, periureteral inflammation
- Reduced and ineffective peristalsis - early drainage is passive, dependent on renal-bladder pressure gradient
- Peristalsis rarely seen before 2 months post-stenting
- Plastic stents develop biofilm and become encrusted/blocked
- Technical success for antegrade stenting: 77-95%; 30% blocked at 3 months in one study
Technique of Antegrade Stenting
- Interpolar or upper pole access preferred
- Nephrostogram confirms level and completeness of stricture
- Curved tip hydrophilic wire + angled high-torque catheter used to cannulate stricture
- Stent deployed across stricture with proximal pigtail in renal pelvis and distal pigtail in bladder
Balloon Dilatation of Ureteric Strictures
- Used for benign ureteric strictures (post-surgical, post-inflammatory)
- High-pressure balloon catheters used
- Best results in short, recent, benign strictures
- Results are inferior for longer, chronic, or malignant strictures
VI. TREATMENT OF URINARY LEAKS AND FISTULAS
- PCN drainage alone often sufficient to allow healing of urinary leaks
- Bypassing the leak site with an internal stent diverts urine away from the fistula
- Combined approach (PCN + stent) used for persistent leaks
- Role of interventional radiology well-established in managing leakage after continent urinary diversion
VII. SUPRAPUBIC BLADDER CATHETERISATION
Indications
- Urethral obstruction not amenable to urethral catheterisation
- Complex urethral trauma
- Neurogenic bladder management
Technique
- Bladder must be adequately distended before puncture
- Catheter should pass through the rectus sheath in the midline, not more than 2 cm above the pubic symphysis
- Seldinger technique: US-guided puncture, wire inserted, serial dilatation, peel-away sheath, catheter placed, balloon inflated; fluoroscopic confirmation
- Trocar technique: After urine aspiration, catheter advanced directly into bladder
- CT-guided insertion for complex pelvic anatomy (previous surgery/congenital abnormalities)
- Image-guided bowel perforation rate: 0.3% vs. 2.4-2.7% for cystoscopically-assisted insertion
VIII. MANAGING A NON-DEFLATABLE URINARY CATHETER BALLOON
- Overinflation (balloon rupture) - risk of bladder rupture + retained fragments: not recommended
- Liquid dissolution agents - risk of chemical cystitis
- Best method: Reopen balloon channel with a hydrophilic or 0.018-inch stiff guidewire
- Alternatively: sharp end of guidewire ruptures the balloon
- If fails: transabdominal US-guided puncture of balloon with a 22-G needle (balloon fixed by gentle urethral traction) OR transrectal US-guided puncture (under antibiotic prophylaxis)
IX. PERCUTANEOUS CYSTOLITHOTRIPSY (PCCL)
- Used for large bladder stones not amenable to endoscopic fragmentation
- Suprapubic access using similar Seldinger technique as SPC
- Lithotripsy performed via percutaneous access
- Particularly useful in patients with urethral stricture or small urethra
X. EMBOLISATION IN THE URINARY TRACT
Renal Artery Embolisation
- Indications: Renal AVM, post-traumatic haemorrhage, AML (angiomyolipoma) bleeding, pre-operative tumour devascularisation, post-PCN arterial haemorrhage
- Endovascular approach has largely replaced open surgery
- Embolic agents: coils, particles (PVA), liquid agents (NBCA, Onyx)
Prostatic Artery Embolisation (PAE)
- Approved by NICE (2018) for benign prostatic hypertrophy (BPH)
- Reduces prostate volume and improves urinary symptoms
- Steep learning curve; refinements in technique ongoing
Varicocele Embolisation
- Via percutaneous sclerotherapy or coil embolisation of the spermatic vein
- Approach: transvenous (left renal vein → left spermatic vein OR right femoral → ovarian vein for females)
- Technical success ~100%; clinical success ~85%
- Complications: venous spasm, perforation, non-target embolisation, thrombophlebitis
- Gonadal shield to minimize radiation to testes
Pelvic Congestion Syndrome (PCS)
- Ovarian vein embolisation (left-sided more common)
- Left renal venogram shows reflux into left ovarian vein
- Tortuous pelvic veins crossing midline
- Amplatzer vascular plug or coils used
XI. RENAL DENERVATION (RDN)
- Used for resistant hypertension (uncontrolled despite 3+ antihypertensive drugs)
- Renal sympathetic nerves run in the adventitia of the renal arteries
- Mechanism: Ablation reduces afferent (chemoreceptor/mechanoreceptor) and efferent sympathetic activity, lowering RAAS activation, reducing noradrenaline spillover
- Technique: Spyral catheter (multiple electrodes) via transfemoral approach into renal artery; radiofrequency energy pulses applied to destroy nerves
- Performed bilaterally, usually as a day case under local anaesthesia and sedation
- Evidence: HTN-3 trial was negative; more recent sham-controlled trials (SPYRAL HTN-ON MED, SYMPLICITY HTN-3) have shown modest but significant BP reduction
- Non-atheromatous disease responds well to PTA alone; stents perform better than PTA for atheromatous disease
XII. ABLATION OF RENAL CYSTS / LYMPHOCELES
- Percutaneous aspiration and injection of sclerosant (e.g., ethanol) for symptomatic simple renal cysts
- Lymphoceles post-renal transplant: percutaneous drainage +/- sclerotherapy
- US-guided approach; fluoroscopic confirmation
SUMMARY TABLE: Key Points for PG Exam
| Topic | Key Fact |
|---|---|
| Safest PCN approach | Lower pole, posterolateral, centre of calyx (Brodel's line) |
| Upper pole access risk | Pleural transgression, pneumothorax |
| Most urgent PCN indication | Pyonephrosis / infected hydronephrosis |
| Primary antegrade stenting contraindication | Infected obstructed system |
| Metal stents for ureter | NiTiNol-based (Uventa, Allium, Memokath); some removable |
| PCN vs stent technical success | Primary stenting ~85%; post-PCN stenting ~100% |
| PAE approval | NICE 2018 for BPH |
| Non-deflatable balloon best Rx | Hydrophilic wire through balloon channel |
| SPC bowel perforation (image-guided) | 0.3% (vs 2.4-2.7% cystoscopic) |
| Arterial post-PCN haemorrhage | Renal angiography + embolisation |
| Peristalsis after stenting | Rarely seen before 2 months |
| RDN nerves location | Adventitia of renal arteries |
| Resistant HTN definition | Uncontrolled on 3+ drugs |
Source: Grainger & Allison's Diagnostic Radiology, Chapter 85 - Interventional Uroradiology, pages 2160-2199
Medullary sponge kidney10 mark
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have comprehensive content from multiple authoritative textbooks with imaging. Here is the complete 10-mark answer:
Medullary Sponge Kidney (MSK)
10-Mark PG Answer
Definition
Medullary sponge kidney (MSK), also called precalyceal canalicular ectasia, is a disorder characterised by dilatation (ectasia) of the distal collecting ducts and cyst formation strictly confined to the medullary pyramids, particularly their inner papillary portions. Despite the name, the kidney does not closely resemble a sponge on gross pathology.
Epidemiology
- Frequency: approximately 1 in 5000 in the general population (many cases are asymptomatic and underestimated)
- Found in up to 20% of patients presenting with nephrolithiasis
- Incidence of MSK in calcium stone formers: ~13% (vs ~2% in otherwise normal patients)
- Associated with a 60% lifetime risk for renal stones
- Women have a greater incidence of MSK than men among calcium stone formers
- Symptoms typically begin between the 4th and 5th decade of life; adolescent presentations are reported
Genetics / Pathogenesis
- Usually regarded as sporadic, but familial clustering with autosomal dominant inheritance (reduced penetrance, variable expressivity) is well-documented
- GDNF (Glial cell-derived neurotrophic factor) gene variants cosegregate with MSK in familial cases
- Mutations in the RET proto-oncogene and GDNF suggest a developmental defect in ureteric bud-metanephric mesenchyme interaction
- Mutations in hydrogen proton pump genes ATP6V1B1 and ATP6V0A4 link MSK to distal RTA
- Associated conditions:
- Congenital hemihypertrophy
- Beckwith-Wiedemann syndrome
- CAKUT syndrome, Wilms tumor
- Ehlers-Danlos syndrome
- Primary hyperparathyroidism
- ADPKD (precalyceal canalicular ectasia commonly seen)
Pathology
- Bilateral in 70% of cases; may involve one or more papillae
- Dilated ducts communicate proximally with normal-sized collecting tubules and show relative constriction at their junction with the calyx
- Duct diameter: usually 1-3 mm, occasionally 5 mm, rarely up to 7.5 mm
- Cysts measure 1-8 mm - spherical or oval, may be isolated or communicate with the collecting system
- Cysts frequently contain spherical concretions composed of apatite (calcium phosphate)
- Affected pyramids and calyces are enlarged; nephromegaly can result when many pyramids are involved
- Renal cortex, medullary rays, calyces, and renal pelvis appear grossly normal
- Histology: dilated ducts may show inflammatory cell infiltration or interstitial fibrosis in prominent cases
Clinical Features
MSK is usually benign and asymptomatic, often discovered incidentally. When symptomatic:
| Feature | Details |
|---|---|
| Renal stones | Most common presentation; calcium oxalate, calcium phosphate (apatite) or mixed |
| Haematuria | Gross or microscopic; recurrent; unrelated to stones or infection |
| UTI | Recurrent; more common in females with stones |
| Renal colic | From stone passage |
| Tubular dysfunction | Mild concentration defect; impaired urinary acidification |
| Incomplete distal RTA | Found in 30-40% of patients; acidification defect after NH4Cl load |
| Bone disease | Osteopenia/osteoporosis from RTA and hypercalciuria |
Metabolic Abnormalities (Stone Risk Factors)
- Hypercalciuria - most commonly absorptive (59%); renal calcium leak in 18%
- Hypocitraturia - most common metabolic abnormality in some series (77%); marker of distal RTA
- Urinary stasis within ectatic tubules
- Hyperparathyroidism (primary) association
- The combination of stasis + hypercalciuria + hypocitraturia drives stone formation
Diagnosis / Imaging
Plain X-ray (KUB)
- Small, round calculi in the pyramidal regions just beyond the calyces
- Calculi arranged in clusters fanning away from the calyx - characteristic distribution
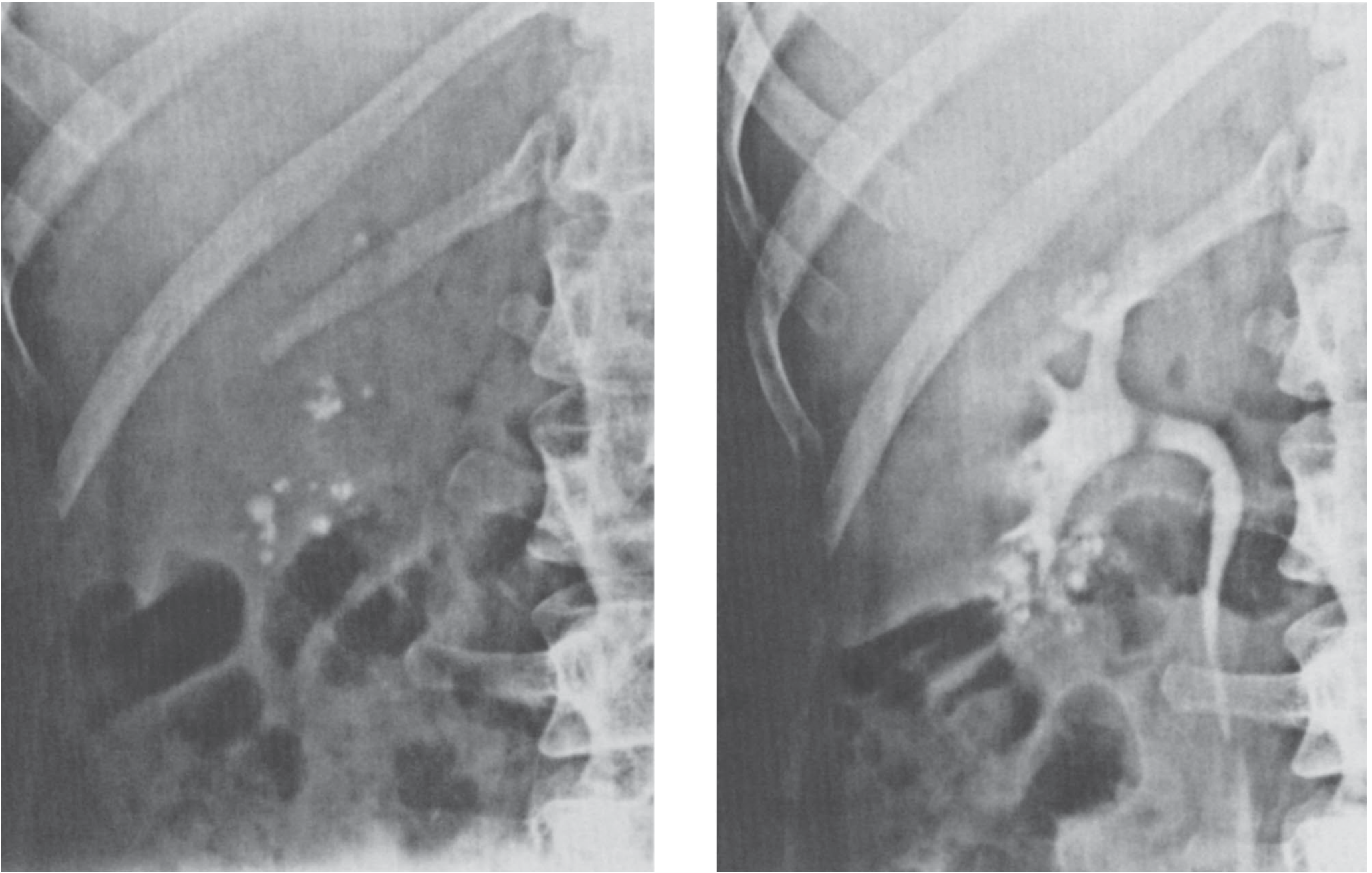
IVU / Excretory Urography (Gold standard - traditional)
- Definitive diagnosis made on excretory urography
- Dilated collecting ducts visualised on early and later radiographs without compression and without ureteral obstruction
- "Bouquet of flowers" or "paintbrush" appearance - dilated (streaked) tubules seen just lateral to calyces; many contain round masses of radiopaque material
- Calyces are large; stones are located in dilated collecting tubules
- Renal pelvis and calyces are normal in configuration
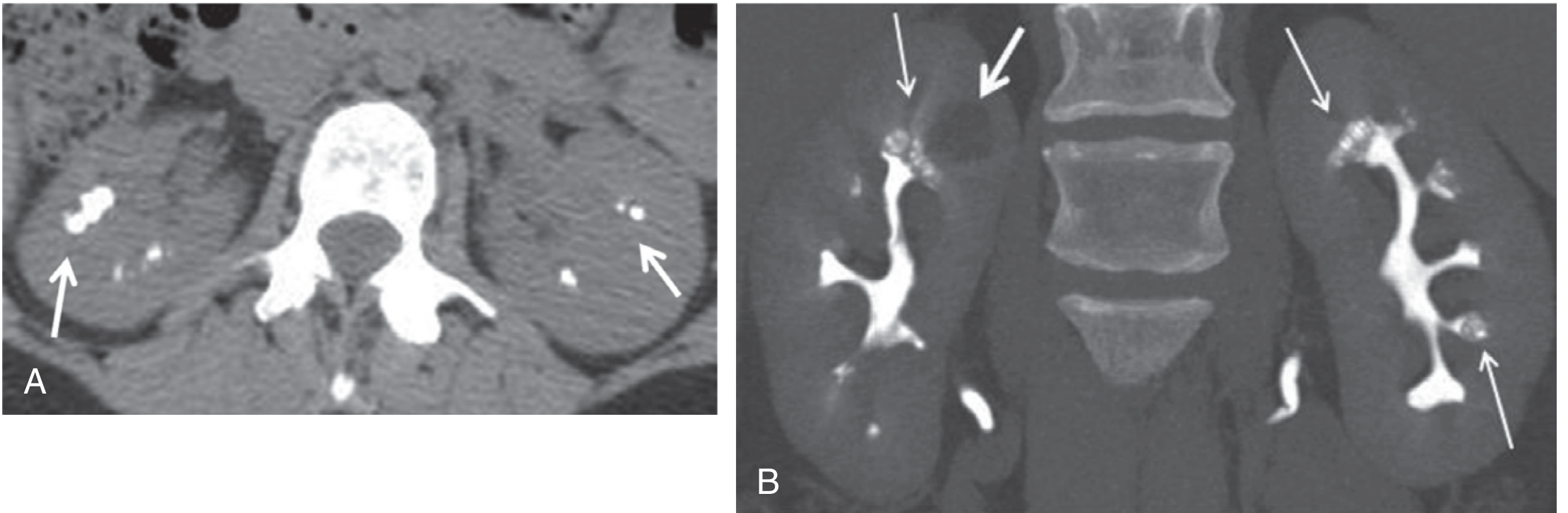
CT (Now the primary investigation)
- Non-contrast CT: Medullary nephrocalcinosis (bilateral medullary calcification) - arrows pointing to medullary calcific foci
- CT Urography (CTU): Using multidetector-row CT with high-resolution 3D reconstruction and late urographic phase:
- Medullary cysts visible
- Dilated collecting tubules showing "papillary brush pattern" bilaterally
- Coronal MIP (maximum intensity projection) during excretory phase best demonstrates the ectatic tubules
Ultrasound
- Medullary hyperechogenicity - suggestive but NOT diagnostic
- Cannot differentiate from other causes of medullary nephrocalcinosis
Differential Diagnosis
| Condition | Distinguishing Features |
|---|---|
| Tuberculosis | Usually unilateral; calyceal ulceration; AFB positive |
| Healed papillary necrosis | Typical calyceal deformity; impaired renal function; associated conditions (DM, analgesics) |
| Nephrocalcinosis (other causes) | More diffuse tubular/parenchymal calcification; features of primary hyperparathyroidism or RTA |
| ADPKD | Cortical + medullary cysts; family history; extrarenal cysts |
Treatment
No specific treatment exists for MSK itself. Management is directed at complications:
Stone Prevention
- High fluid intake: target urine output >2.5 L/day
- Potassium citrate (first-line): 20 mEq/day in two divided doses, titrated to urinary citrate >450 mg/24 h; monitor urine pH (keep <7.5 to prevent calcium phosphate stone formation in ectatic tubules)
- Achieves significant reduction in stone event rate: 0.58 to 0.10 stones/year/patient
- Also improves bone densitometry (vertebral T-score: -2.82 to -1.98; hip T-score: -2.03 to -1.86)
- Thiazide diuretics: added for persistent hypercalciuria or ongoing stone passage despite citrate
- Stone composition directs specific metabolic treatment (restrict oxalate for calcium oxalate stones, etc.)
UTI Management
- Standard antibiotic treatment for episodes
- Surveillance urine cultures in recurrent cases
Stone Clearance
- ESWL / ureteroscopy / PCNL as per stone size and location
Prognosis
- Generally excellent - benign disorder that rarely progresses to ESKD
- Most patients remain asymptomatic throughout life
- A small minority suffer from recurrent urolithiasis, bacteriuria, and pyelonephritis leading to reduced GFR
- Does not transform into malignancy
- Bone mineral density can improve with potassium citrate therapy
Summary Box for PG Exam
| Key Point | Fact |
|---|---|
| Pathology confined to | Medullary pyramids (papillary collecting ducts) |
| Bilateral involvement | 70% |
| Classic imaging | IVU - "bouquet of flowers / paintbrush" appearance |
| CT finding | Medullary calcinosis + papillary brush pattern on CTU |
| Best investigation currently | Multidetector CT Urography (late excretory phase + MIP) |
| Most common metabolic abnormality | Hypercalciuria + Hypocitraturia |
| RTA type | Incomplete distal RTA (30-40%) |
| Gene associations | GDNF, RET, ATP6V1B1, ATP6V0A4 |
| Stone type | Calcium phosphate (apatite) or mixed with calcium oxalate |
| Treatment | Potassium citrate + high fluid intake; thiazides second-line |
| Prognosis | Good; ESKD rare |
Sources: Brenner & Rector's The Kidney (8e), p. 2018-2019 | Comprehensive Clinical Nephrology (7e), p. 675 | Smith & Tanagho's General Urology (19e), p. 544 | Campbell-Walsh-Wein Urology
This is a shared conversation. Sign in to Orris to start your own chat.