
IMG_3290.jpeg
24 yr old male , pain and swelling in lower eye lid.. what is the probable cause
Reading File
Finding Sources
Searching PubMed
hordeolum chalazion eyelid diagnosis management
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Loading Image
The textbook image is a near-perfect match to the patient's photo. Here is a full clinical analysis:
Most Probable Diagnosis: Hordeolum (Stye) - possibly with early Chalazion features
What the Image Shows
The patient's lower eyelid shows:
- Diffuse erythema and edema of the lower lid
- Swelling along the lid margin with some puffiness extending onto the palpebral conjunctiva/inner lid
- No visible pointing pustule yet (suggesting either very early stage or an internal hordeolum)
Compare with the textbook image of a chalazion, lower lid (Pfenninger & Fowler's Procedures for Primary Care) - the morphology is virtually identical.
Differential Diagnosis (Most to Least Likely)
| Condition | Features supporting it | Features against |
|---|---|---|
| Hordeolum (internal/external stye) | Acute onset, painful, tender, erythematous swelling, young patient | No visible pointing pustule yet |
| Chalazion | Lower lid swelling, similar appearance | Chalazions are typically painless/minimally tender; this patient has pain |
| Preseptal (periorbital) cellulitis | Lid erythema and swelling | No fever mentioned, no trauma/sinus history, swelling localized to lid only |
| Allergic reaction | Eyelid edema | Would be bilateral, itchy, less painful |
| Dacryocystitis | Painful swelling near eye | Located near inner canthus/nasal side, not diffuse lower lid |
Distinguishing Hordeolum vs. Chalazion
- A hordeolum is an acute bacterial abscess of a meibomian, Zeis', or Moll's gland - typically Staphylococcus - and is tender, erythematous, and may show fluctuance. It often drains spontaneously at 5-7 days.
- A chalazion is a chronic granulomatous inflammation of a meibomian gland - generally painless or mildly tender, without significant cellulitis.
Given this patient's age (24), acute pain, and visible erythema + swelling, a hordeolum is the primary diagnosis. The diffuse lower lid swelling also suggests possible eyelid cellulitis associated with the hordeolum.
Management
For Hordeolum:
- Warm compresses - 10-15 minutes, 4x/day - the first-line treatment; promotes spontaneous drainage
- Eyelid scrubs with diluted baby shampoo or commercial lid wipes at the lash base
- Topical antibiotic ointment (erythromycin) to the lid margin
- If cellulitis component is significant: oral antibiotics (e.g., doxycycline or dicloxacillin)
- If no resolution in 2-3 weeks: refer to ophthalmologist for incision and drainage
Red flags requiring urgent referral:
- Fever, proptosis, restricted eye movement, or vision changes - these suggest orbital cellulitis, which is a serious, vision-threatening emergency
Note: This analysis is for educational purposes. A proper slit-lamp examination by a physician or ophthalmologist is recommended for definitive diagnosis, especially if symptoms worsen or do not resolve with warm compresses within a week.
Reference: Pfenninger and Fowler's Procedures for Primary Care, 3rd ed., Chapter 65 - Chalazion and Hordeolum
Search for clinical images showing hordeolum drainage and healing stages
Finding Sources
Searching the Web
hordeolum stye clinical images drainage healing stages eyelid
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
Here is a complete visual guide to hordeolum - from the clinical stages through to drainage procedure.
Hordeolum: Clinical Stages, Drainage & Healing
1. Anatomy - Chalazion vs. Stye (Hordeolum) Compared
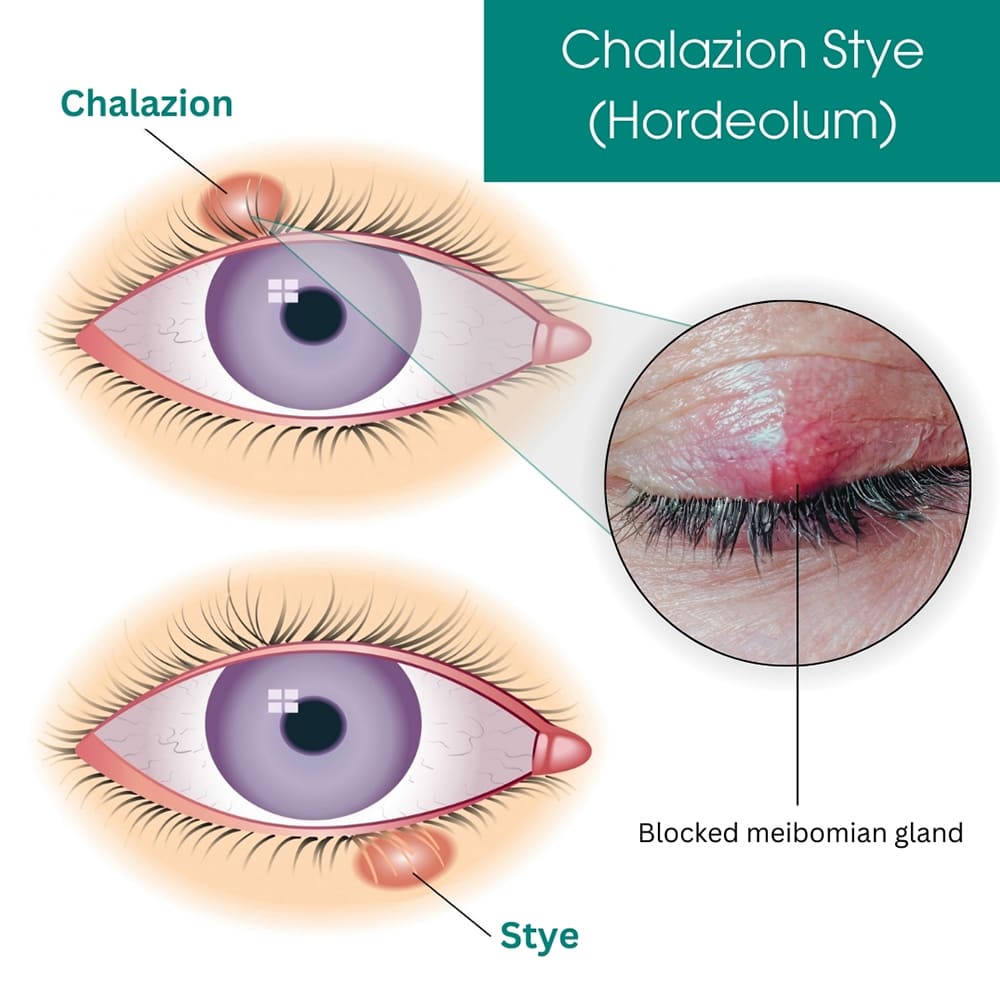
- Chalazion (upper diagram) = located in the body of the lid, caused by non-infectious meibomian gland obstruction - typically painless
- Stye/Hordeolum (lower diagram) = at the lid margin, caused by bacterial infection (usually Staph. aureus) - painful, erythematous
- The inset clinical photo shows an acutely inflamed, erythematous blocked meibomian gland - essentially what your patient has
2. Clinical Appearance - Differentiating Chalazion from Hordeolum

- Top photo: Chalazion - diffuse lid erythema and edema
- Middle diagram: Hordeolum - discrete tender nodule pointing at lid margin
- Bottom photo: Post-drainage / healing stage - residual mild redness, reduced swelling
3. Stages of a Hordeolum (Natural History)
| Stage | Day | Clinical Features |
|---|---|---|
| Stage 1 - Pricking pain | Day 1 | Mild tenderness, subtle redness, no visible lump yet |
| Stage 2 - Bump visible | Day 2-3 | Small red painful lump appears at lid margin; may show yellow/white pus head |
| Stage 3 - Peak inflammation | Day 3-5 | Maximum swelling, erythema, induration; may cause partial lid closure |
| Stage 4 - Pointing/Drainage | Day 5-7 | Pustule points and spontaneously ruptures - pus discharges, pain rapidly relieves |
| Stage 5 - Healing | Day 7-14 | Residual swelling resolves; redness fades; full recovery |
Per the Merck Manual: "Within 2 to 4 days, the lesion ruptures and discharges material (often pus), thereby relieving pain and resolving the lesion."
4. Surgical Drainage Technique (when conservative treatment fails)
Step A - Hordeolum pointing externally (pre-incision)
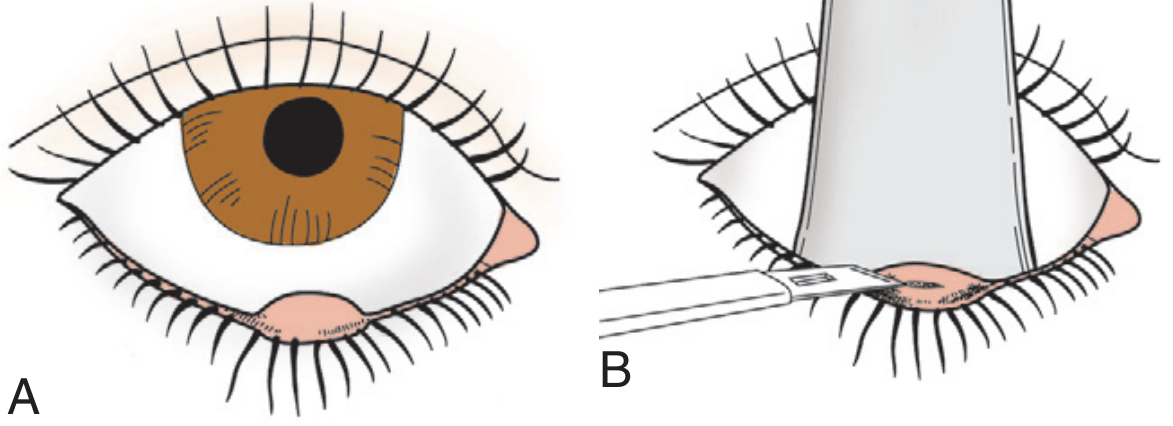
- Panel A: External hordeolum fully pointed and ready for drainage
- Panel B: A no. 11 scalpel blade makes a small incision; a tongue blade or metal elevator is placed behind the lid to protect the globe
Step B - Chalazion clamp stabilizing the lid during procedure

The chalazion clamp is applied to maintain hemostasis and stabilize the tissue. Pus is then expressed and gauze pressure applied for 5-10 min.
5. Surgical Treatment Procedure Summary
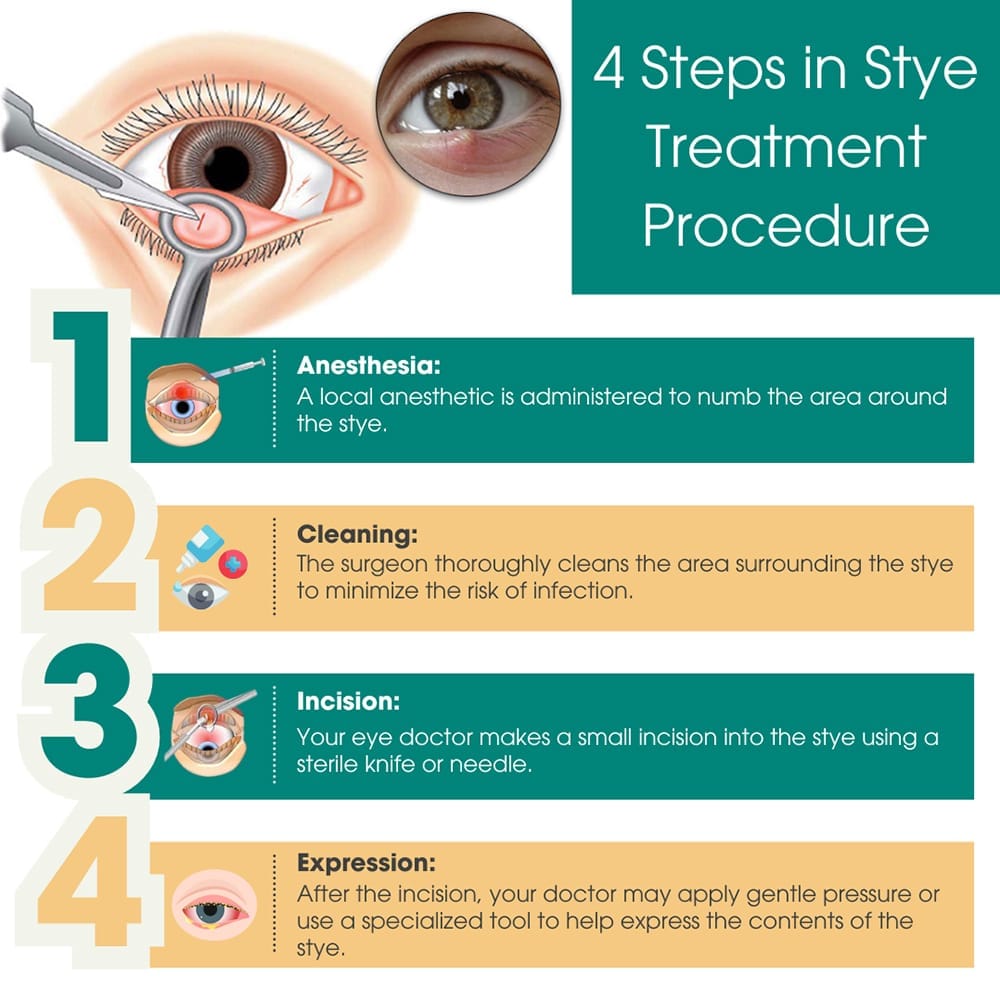
The 4 steps when surgical I&D is needed:
- Anesthesia - 2% lidocaine with epinephrine injected subcutaneously
- Cleaning - area cleaned/prepped to reduce infection spread
- Incision - small stab incision with no. 11 blade into the pointing area
- Expression - gentle pressure or curettage to evacuate pus
Key Points for Your Patient (24M, lower lid)
- Most hordeola do not need surgical drainage - they self-resolve in 5-7 days with warm compresses
- Only proceed to I&D if: no response to warm compresses by day 7-10, fluctuance is obvious, or there is spreading cellulitis
- Topical antibiotics (erythromycin ointment) help prevent spread but do not significantly shorten the natural course
- Do NOT squeeze or attempt to pop the stye - this can spread the infection and cause preseptal cellulitis
- Refer urgently if fever, proptosis, restricted extraocular movements, or vision changes develop
Sources: Pfenninger & Fowler's Procedures for Primary Care, 3rd ed.; StatPearls - Hordeolum; Merck Manual Professional
This is a shared conversation. Sign in to Orris to start your own chat.