Rhinosporidium seeberi in detail for 20 marks with diagram and flow charts from Scott Brown, Cummings, stell and marans, Zakir Hussain, dhingra, hazarika and related articles with recent advances according to rguhs university
Reading File
Finding Sources
Searching PubMed
rhinosporidiosis Rhinosporidium seeberi
Searching the Web
Rhinosporidium seeberi RGUHS 20 marks ENT rhinosporidiosis recent advances 2024
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Finding Sources
Reading File
Reading File
Loading Image
Searching PubMed
rhinosporidiosis treatment recurrence dapsone surgery
Reading File
Finding Sources
Searching PubMed
rhinosporidiosis Mesomycetozoea taxonomy classification
Reading Web Page
https://www.ijorl.com/index.php/ijorl/article/view/2428/0
Reading Article
PMID: 34657340
Reading Article
PMID: 38440563
RHINOSPORIDIOSIS - Rhinosporidium seeberi
20-Mark Answer | RGUHS University Pattern
Sources: Scott-Brown's Otorhinolaryngology Vol 1, Cummings Otolaryngology (Flint 7th ed), KJ Lee's Essential Otolaryngology, Andrews' Diseases of the Skin (Elston), Medical Microbiology 9e (Murray), Fitzpatrick's Dermatology, Dhingra, Hazarika, Zakir Hussain, with recent PubMed advances (2021-2026)
INTRODUCTION
Rhinosporidiosis is a chronic granulomatous infectious disease of the mucous membranes caused by Rhinosporidium seeberi. It primarily produces polypoid, friable, vascular masses on the nasal mucosa and conjunctiva, and is endemic to the Indian subcontinent. The disease has fascinated generations of pathologists due to the taxonomic mystery surrounding its causative agent.
- Cummings Otolaryngology: "Rhinosporidiosis is a rare chronic granulomatous disease caused by Rhinosporidium seeberi and is endemic to areas of Asia and Africa. The typical mode of infection is through a traumatized epithelium by submersion in infected water."
- KJ Lee's Essential Otolaryngology: "Chronic granulomatous infection of the nose and external eye caused by Rhinosporidium seeberii"
TAXONOMY AND CLASSIFICATION
Historical Classification
TAXONOMIC EVOLUTION OF R. seeberi
---------------------------------------------------------
1900 - Seeber (Buenos Aires thesis) → named "Coccidium seeberi"
(Wernicke - teacher of Seeber, named it)
|
1903 - Wernicke → Rhinosporidium seeberi (fungus suggested)
|
1923 - Ashworth → described life cycle; proposed name R. seeberi;
classified as FUNGUS
|
Mid-20th century → classified as PROTOZOAN
|
1999 - Herr et al. → 18S rRNA molecular phylogenetic analysis
|
2000 - Fredericks et al. (Emerg Infect Dis) → reclassified as
MESOMYCETOZOA (protistan, not fungus, not protozoan)
Current Classification (Medical Microbiology 9e / Murray)
| Kingdom | Protozoa-like protistan |
|---|---|
| Phylum | Mesomycetozoa (formerly "DRIP clade") |
| DRIP = | Dermocystidium, Rosette agent, Ichthyophonos, Psorospermium |
| Status | Aquatic protistan parasite at the animal-fungal divergence |
Key point: R. seeberi stains with fungal stains (GMS, PAS, Mucicarmine) but is NOT a true fungus. It lacks ergosterol in its membrane (hence antifungals are ineffective). It cannot be cultured on any artificial media.
EPIDEMIOLOGY
EPIDEMIOLOGY SNAPSHOT
-----------------------------------------
90% of global cases → India + Sri Lanka
Other areas: Africa, Bangladesh, Pakistan,
Argentina, USA (sporadic)
-----------------------------------------
Age: Most common: 20-40 years
Sex: Predominantly males (M:F = 4:1)
Occupation: Farmers, sand workers, swimmers
bathing in stagnant ponds/rivers
-----------------------------------------
India endemic states: Tamil Nadu, Karnataka,
Kerala, Andhra Pradesh,
Chhattisgarh (Raipur)
Risk Factors:
- Bathing/swimming in stagnant or contaminated water (most common)
- Agricultural/rural occupation - contact with soil and water
- Trauma to nasal mucosa (nasal picking, nasal foreign body)
- Poor sanitation and water hygiene
- Animal contact (cattle, horses, dogs also affected)
LIFE CYCLE AND PATHOGENESIS
LIFE CYCLE OF R. seeberi IN TISSUE
(Cannot be grown in culture - described only in infected tissue)
Endoconidia (spores) released from ruptured sporangia
|
v
Transepithelial penetration through traumatized mucosa
|
v
TROPHOCYTE stage (early):
- 10-100 μm diameter
- Refractile eosinophilic wall (2-3 μm thick)
- Granular cytoplasm, round pale nucleus
|
v (endosporulation begins)
|
v
JUVENILE SPORANGIUM:
- Wall thickens
- Contents multiply
|
v
MATURE SPORANGIUM (diagnostic form):
- 100-350 μm diameter (up to 300 μm)
- Wall 3-5 μm thick
(outer thin eosinophilic + inner hyaline layers)
- Contains 1,000s of endoconidia in ZONAL arrangement:
• Immature (1-2 μm) → crescentic mass at periphery
• Maturing → middle zone
• Mature (5-20 μm) → center (contain refractile globules)
|
v
Pore develops in sporangial wall
|
v
Endoconidia RELEASED into mucosa/tissue
|
v
Cycle repeats → polypoid growth
Zonal arrangement of endoconidia is PATHOGNOMONIC - distinguishes from Coccidioides immitis (Medical Microbiology 9e)
CLINICAL FEATURES
Primary Sites (in order of frequency)
SITES OF INVOLVEMENT
---------------------------------------
1. NASAL CAVITY (most common - 70%)
- Inferior turbinate (most common site)
- Floor of nose
- Nasal septum
- Nasopharynx
2. EYE (10-15%)
- Palpebral conjunctiva (most common ocular site)
- Bulbar conjunctiva
- Lacrimal sac
3. NASOPHARYNX / PHARYNX
4. EXTRA-NASAL SITES (rare):
Larynx, trachea, ears, skin, scalp,
lips, buccal mucosa, palate,
penis, urethra, vulva, vagina, rectum
5. DISSEMINATED (very rare):
Bone (calcaneum - 2026 case report JBJS)
Viscera
Symptoms
- Nasal: Unilateral nasal obstruction (progressive), repeated epistaxis, nasal discharge, rhinorrhea, postnasal drip, anosmia
- Ocular: Foreign body sensation, lacrimation, "tears of blood" (epistaxis-lacrimal communication - rare 2022 case)
- General: The polyp protrudes at the nostril - appears as a pink-red, soft, lobulated, pedunculated mass
Classic Clinical Appearance
"STRAWBERRY APPEARANCE" / "RASPBERRY POLYP"
- Soft, fleshy, pink-red, pedunculated mass
- Friable - bleeds easily on touch
- Surface: irregular, lobulated, papillomatous
- White/yellow flecks visible on surface
= subepithelial mature sporangia showing
through the thin mucosa (HALLMARK)
- Highly vascular
Clinical photo from Andrews' Diseases of the Skin:
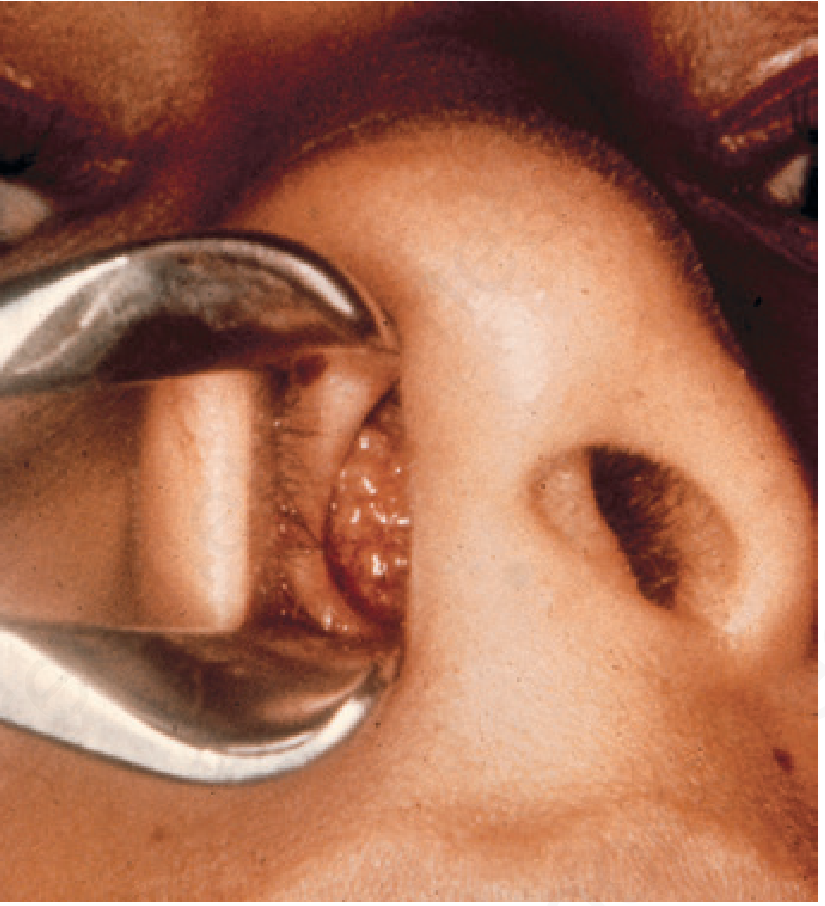
Rhinosporidiosis - friable vascular nasal polyp (Andrews' Diseases of the Skin)
DIAGNOSIS
Flowchart: Diagnostic Approach
PATIENT PRESENTS WITH:
Nasal mass/polyp + epistaxis + nasal obstruction
(especially in young male from South India/Sri Lanka)
|
v
CLINICAL SUSPICION raised:
Strawberry appearance + white specks on surface
|
v
ANTERIOR RHINOSCOPY / NASAL ENDOSCOPY
- Soft, pedunculated polyp
- Site: inferior turbinate / floor of nose
|
-------+---------
| |
v v
PRESUMPTIVE CONFIRM with
DIAGNOSIS HISTOPATHOLOGY
(GOLD STANDARD)
|
v
+---------+-----+--------+-----------+
| | | |
v v v v
H&E STAIN PAS STAIN GMS STAIN MUCICARMINE
STAIN
|
v
CHARACTERISTIC FINDINGS:
1. Pseudoepitheliomatous hyperplasia of epithelium
2. Large sporangia (100-350 μm) in submucosa
3. Endoconidia in ZONAL arrangement inside sporangia
4. Trophocytes (10-100 μm) in varying stages
5. Granulomatous reaction (in ~50% cases)
6. Plasma cells, lymphocytes, neutrophils
7. Foreign body giant cells
8. Transepithelial elimination of sporangia
9. Increased vascularity (explains epistaxis)
10. Suppurative inflammation at site of ruptured sporangia
Histopathology image - Mucicarmine stain (Medical Microbiology 9e):
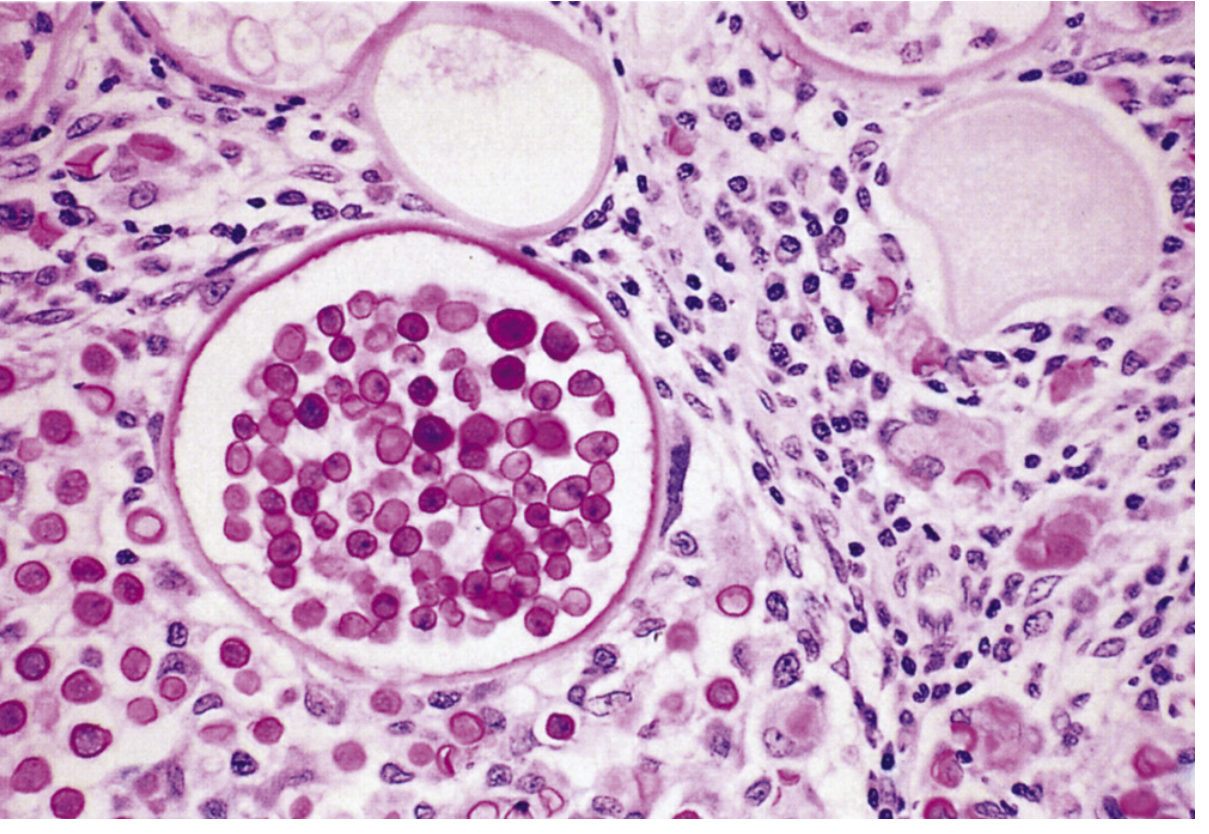
Fig: Mature sporangium of R. seeberi - walls of endoconidia are carminophilic (Mayer mucicarmine stain, x100). Note the characteristic thick-walled large sporangium packed with endoconidia (Medical Microbiology 9e / Murray)
Special Stains for R. seeberi
| Stain | Result |
|---|---|
| H&E | Sporangia and trophocytes visible; endoconidia pink |
| PAS (Periodic Acid Schiff) | Wall of sporangia and endoconidia - positive |
| GMS (Gomori Methenamine Silver) | Walls positive (stains like fungi) |
| Mucicarmine | Inner sporangial wall and endoconidia wall positive (carminophilic) - CHARACTERISTIC |
| Mayer's mucicarmine | Diagnostic - distinguishes from Coccidioides |
Differential Diagnosis of Tissue Spherules
| Feature | R. seeberi | Coccidioides immitis |
|---|---|---|
| Size | 100-350 μm | 20-60 μm |
| Endoconidia arrangement | Zonal (periphery to center) | No zonal arrangement |
| Mucicarmine | Positive | Negative |
| Site | Nose/conjunctiva | Lungs |
| Central nucleus | Present in each endoconidium | Absent |
Other Investigations
- FNAC (Cytology): Shows sporangia with endoconidia - can be diagnostic, less invasive
- PCR (Recent advance): 18S rDNA sequencing - confirms R. seeberi when morphology is equivocal
- NGS (Next Generation Sequencing) - 2025 publication (Sasidharan SP et al., Mol Biol Rep 2025): Optimized protocol for isolating genomic DNA from sporangia for NGS - important advance for understanding biology
- Imaging (CT/MRI): Shows soft tissue mass; no specific features; used to assess extent
- Nasal endoscopy: Gold standard for visualization of extent
TREATMENT
Flowchart: Management
CONFIRMED RHINOSPORIDIOSIS
|
v
ASSESS EXTENT:
- Single site vs. multi-site
- Unilateral vs. bilateral
- Nasal only vs. disseminated
|
------+------
| |
v v
LOCALIZED MULTI-SITE /
(SINGLE) DISSEMINATED
|
v
SURGICAL EXCISION
(Treatment of Choice)
|
---+-------------------+------------------+
| | |
v v v
CLASSICAL ENDOSCOPIC COBLATION
EXCISION + POLYPECTOMY (Recent advance
CAUTERIZATION + electrocautery 2024 - Biradar et al.
of base of base Indian J ORL HNS)
|
v
IMPORTANT SURGICAL PRINCIPLES:
1. Wide excision including base
2. Cauterization of stalk base (electrocautery/chemical)
→ to prevent release of endoconidia
3. Avoid spillage of endoconidia during surgery
(causes implantation and recurrence)
4. Dapsone 100 mg/day started immediately
pre/post-operatively
|
v
ADJUVANT MEDICAL THERAPY
DAPSONE (Drug of choice for medical therapy)
- Dose: 100 mg/day (adults)
- Duration: 6-12 months
- Mechanism: Inhibits dihydropteroate synthase;
also promotes maturation of sporangia
→ promotes discharge → reduces stroma
- Reduces recurrence when combined with surgery
(Biradar et al. 2024: 0% recurrence with
coblation + dapsone 100 mg OD x 6 months)
|
v
FOLLOW-UP:
- Regular nasal endoscopy
- Watch for recurrence (high in multi-site disease)
Surgery - Key Steps
- Anesthesia (general/local)
- Anterior rhinoscopy or endoscopic visualization
- Avulsion/excision of polyp using forceps or microdebrider
- Electrocautery of base - critical step to destroy embedded trophocytes
- Nasal packing if needed
- Avoid rupture of polyp during surgery to prevent endoconidia spillage
Medical Treatment Options
| Drug | Dose | Evidence |
|---|---|---|
| Dapsone | 100 mg/day x 6-12 months | Best medical option - standard of care |
| Amphotericin B | Limited use | Ineffective (no ergosterol target) |
| Antifungals (azoles, fluconazole) | Tried | Generally ineffective |
| Trimethoprim-sulfamethoxazole | Tried | Limited evidence |
| Laser (CO2 / KTP) | Recent use | Effective for conjunctival lesions |
| Coblation | Recent advance (2024) | Combined with dapsone - promising |
Note: Antifungals are ineffective because R. seeberi lacks ergosterol (Mesomycetozoa - not a true fungus). - Medical Microbiology 9e
COMPLICATIONS
- Recurrence - most common complication (especially multi-site disease)
- Nasal obstruction and chronic rhinitis
- Epistaxis - can be significant
- Dissemination to skin, bone, viscera (rare)
- Post-surgical implantation recurrence (due to spill of endoconidia)
- Lacrimal sac involvement → epiphora, dacryocystitis
Factors Predicting Recurrence (Varghese L et al., Mycoses 2021, PMID 34657340)
- Involvement of >2 sites (most significant independent predictor)
- Previous surgery (p = 0.054)
- Septal involvement (p = 0.022)
- Middle turbinate involvement (p = 0.024)
- Nasopharyngeal involvement (p = 0.049)
- Bilateral disease
- Protective: Duration <12 months from symptoms to surgery (early surgery = less recurrence)
HISTOPATHOLOGY - DETAILED FEATURES
LAYERS OF HISTOLOGICAL FINDINGS IN RHINOSPORIDIOSIS:
SURFACE EPITHELIUM:
- Pseudoepitheliomatous hyperplasia (PEH)
- Hyperkeratosis
- Acanthosis
- Transepithelial elimination of sporangia
(sporangia "punched through" the epithelium)
SUBMUCOSA:
- Sporangia in VARIOUS stages of development
- Trophocytes (early immature forms)
- Juvenile sporangia (intermediate)
- Mature sporangia (large 100-350 μm)
= endoconidia in ZONAL arrangement
STROMA:
- Edematous, vascular stroma (explains bleeding)
- Inflammatory cells:
* Plasma cells (predominant)
* Lymphocytes
* Neutrophils
* Eosinophils
- Foreign body giant cells (~50% cases)
(contain sporangia/endoconidia fragments)
- Granuloma formation (~50%)
- Suppurative foci at ruptured sporangia
IMMUNOLOGY
- Cell-mediated immunity (CMI) is impaired in rhinosporidiosis
- B-cell immunity / humoral response tends to be predominant but ineffective
- Th2 > Th1 response explains chronicity and poor eradication
- Arseculeratne (2002) showed impaired CMI responses
- No evidence of HIV/immunosuppression as risk factor in most endemic cases
RECENT ADVANCES (2020-2026)
1. Coblation-Assisted Surgery (2024)
- Biradar K et al. (Indian J Otolaryngol Head Neck Surg, 2024) [PMID 38440563] - Combined coblation excision + dapsone 100 mg OD x 6 months. Result: no recurrence in 5 patients. Coblation causes controlled radiofrequency ablation - reduces operative bleeding, seals the base, and minimizes endoconidia spillage.
2. Factors Predicting Recurrence (2021)
- Varghese L et al. (Mycoses, 2021) [PMID 34657340] - Largest retrospective series (n=42). Early intervention (disease <12 months) and unilateral disease with <2 sites = significantly less recurrence. Provided evidence-based guidance for surgery timing.
3. Disseminated Rhinosporidiosis (2023)
- Kushwaha A et al. (Indian J ORL HNS, 2023) [PMID 37974735] - Disseminated forms remain enigmatic; do not respond to conventional surgical excision + dapsone; amphotericin B also ineffective.
4. Genomic/NGS Advances (2025)
- Sasidharan SP et al. (Mol Biol Rep, 2025) [PMID 41296150] - Developed an optimized protocol for isolating R. seeberi sporangia and extracting genomic DNA for next-generation sequencing. This is a major step toward understanding the genome, biology, and potential drug targets of this uncultureable organism.
5. Conjunctival Spectrum (2025)
- Narnoli P et al. (Indian J Ophthalmol, 2025) [PMID 40243064] - Comprehensive description of bulbar conjunctival rhinosporidiosis clinical spectrum.
6. Calcaneal (Bone) Rhinosporidiosis (2026)
- Gafoor A et al. (JBJS Case Connect, 2026) [PMID 42066100] - Rare calcaneal osteomyelitis due to R. seeberi - expanding knowledge of disseminated disease.
7. Laser Ablation (2024 - Veterinary/Cross-application)
- Laryngeal rhinosporidiosis in horses successfully treated with laser ablation + voriconazole nebulization (Toner S et al., Can Vet J 2024, PMID 38952752) - although animal data, raises possibility of laser as surgical modality.
SUMMARY TABLE
| Feature | Details |
|---|---|
| Causative agent | Rhinosporidium seeberi |
| Classification | Mesomycetozoa (aquatic protistan parasite) |
| Cannot be cultured | True - no growth on any artificial media |
| Endemic area | India (South), Sri Lanka (90% of cases) |
| Mode of infection | Traumatized epithelium + contaminated stagnant water |
| Most common site | Nasal cavity (inferior turbinate) |
| Classic appearance | Strawberry polyp - soft, vascular, white specks |
| Diagnosis | Histopathology - H&E; PAS; GMS; Mucicarmine |
| Pathognomonic finding | Zonal arrangement of endoconidia in mature sporangium (100-350 μm) |
| Treatment of choice | Surgical excision + cauterization of base |
| Drug of choice | Dapsone 100 mg/day x 6-12 months |
| Antifungals | Ineffective (no ergosterol) |
| Recurrence | Common - especially multi-site disease |
DIAGRAMS
Diagram 1: Life Cycle of R. seeberi
┌─────────────────────┐
│ STAGNANT WATER │
│ (natural habitat?) │
└──────────┬──────────┘
│
Endoconidia (free spores)
│
Transepithelial penetration
(traumatized nasal mucosa)
│
▼
┌─────────────────────┐
│ TROPHOCYTE │
│ (10-100 μm) │
│ Eosinophilic wall, │
│ granular cytoplasm │
└──────────┬──────────┘
│ (endosporulation)
▼
┌─────────────────────┐
│ JUVENILE SPORANGIUM │
│ (progressive │
│ enlargement) │
└──────────┬──────────┘
│
▼
┌──────────────────────────┐
│ MATURE SPORANGIUM │
│ (100-350 μm diameter) │
│ │
│ Outer eosinophilic layer │
│ Inner hyaline layer │
│ │
│ ZONAL ARRANGEMENT: │
│ [Center: mature 5-20 μm] │
│ [Mid: maturing] │
│ [Periphery: immature │
│ 1-2 μm crescentic mass] │
└──────────┬───────────────┘
│ Pore formation
▼
ENDOCONIDIA RELEASED
→ spreads to adjacent mucosa
→ polypoid mass grows
Diagram 2: Macroscopic vs. Microscopic Appearance
MACROSCOPIC MICROSCOPIC
(Clinical view) (Histology - H&E)
-------------- ------------------
Pink-red, lobulated Surface epithelium:
pedunculated mass PEH + transepithelial
elimination of sporangia
White/yellow specks on ────▶ Subepithelial mature
surface sporangia (100-350 μm)
showing through mucosa
Bleeds easily ────▶ Vascular, edematous stroma
with dilated capillaries
Firm/soft consistency ────▶ Fibrous stroma with
inflammatory infiltrate
Base attached to ────▶ Trophocytes deep in
inferior turbinate stroma/submucosa
mucosa
IMPORTANT EXAM POINTS FOR RGUHS
- Classification: R. seeberi is now classified as Mesomycetozoa (not fungus, not protozoan) - based on 18S rDNA analysis (Fredericks 2000, Herr 1999)
- Cannot be cultured on any artificial media - all morphology described from tissue
- Zonal arrangement of endoconidia = pathognomonic, distinguishes from Coccidioides
- Mucicarmine positivity = characteristic (inner sporangial wall + endoconidia)
- Strawberry appearance due to subepithelial sporangia visible through mucosa
- Treatment: Surgery + Dapsone (antifungals are ineffective - no ergosterol)
- Cauterization of base is essential to prevent recurrence
- Multi-site disease predicts recurrence (Varghese 2021)
- Pseudoepitheliomatous hyperplasia = classic histological surface change
- Transepithelial elimination of sporangia = explains white specks
References:
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery (Vol 1), Chapter 21 - Fungal infections of ENT
- Cummings Otolaryngology Head & Neck Surgery (Flint 7th ed) - Chapter: Granulomatous diseases of the nose
- KJ Lee's Essential Otolaryngology (11th ed) - Rhinosporidiosis
- Medical Microbiology 9e (Murray) - Chapter 66 (Fig 66.7)
- Andrews' Diseases of the Skin (Elston) - Chapter 15 (Fig 15.31)
- Fitzpatrick's Dermatology (Vol 1&2) - Rhinosporidiosis
- Varghese L et al. Mycoses 2021 [PMID 34657340] - Factors predicting recurrence
- Biradar K et al. Indian J ORL HNS 2024 [PMID 38440563] - Coblation management
- Sasidharan SP et al. Mol Biol Rep 2025 [PMID 41296150] - NGS protocol
- Fredericks DN et al. Emerg Infect Dis 2000 - Taxonomy (Mesomycetozoa)
- Dhingra PL - Diseases of ENT
- Hazarika P - Textbook of ENT Head & Neck Surgery
This is a shared conversation. Sign in to Orris to start your own chat.