Pupil and it's abnormalities from basics to clinical at mbbs level with some clinical based scenarios for better understanding
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
Excellent! I now have rich textbook content and clinical images. Let me compile the comprehensive answer.
The Pupil: From Basics to Clinical - A Complete MBBS Guide
1. ANATOMY OF THE PUPIL
The pupil is the circular aperture in the center of the iris that regulates light entry into the eye. Normal size is 2-6 mm in ambient light (average ~3 mm; smaller in the elderly).
Iris Muscles
Two smooth muscles control pupil size with reciprocal action:
| Muscle | Location | Innervation | Receptor | Action |
|---|---|---|---|---|
| Sphincter pupillae | Circumferential around pupil | Parasympathetic (CN III) | Muscarinic (M3) | Constriction - Miosis |
| Dilator pupillae | Radial fibers | Sympathetic | Alpha-1 (α1) | Dilation - Mydriasis |
Pupil size = balance between sympathetic tone (dilation) and parasympathetic tone (constriction).
- Costanzo Physiology 7th Edition, p. 63
2. NEURAL CONTROL (INNERVATION)
A. Parasympathetic Pathway (Miosis - Constriction)
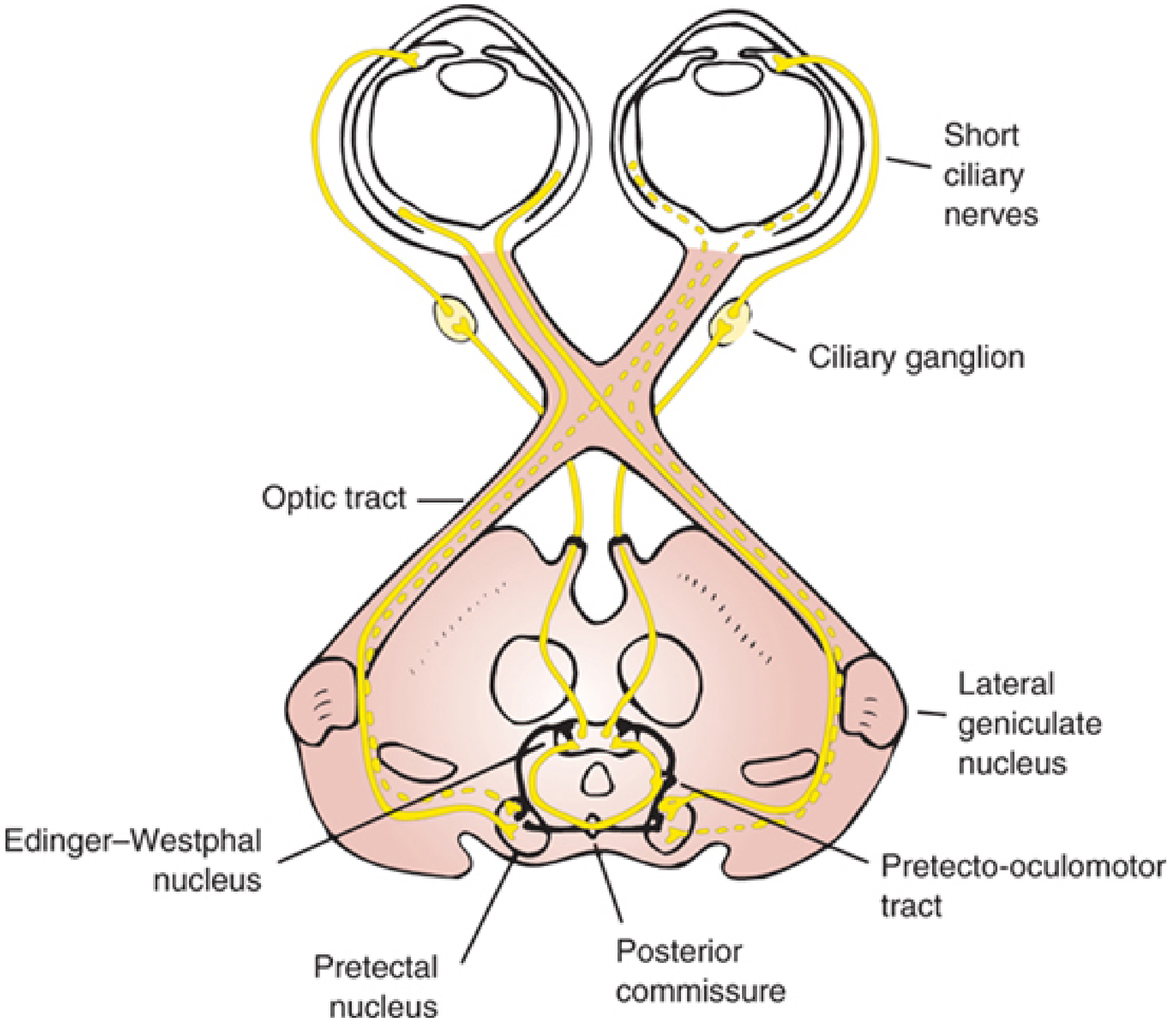
FIGURE: Parasympathetic innervation of the pupil and pathways for the light reflex (Localization in Clinical Neurology, 8e)
- Edinger-Westphal nucleus (rostral midbrain) - preganglionic parasympathetic origin
- Fibers travel with CN III (oculomotor nerve) - in the periphery/superficial dorsal surface of the nerve
- Synapse in ciliary ganglion (behind the globe, lateral to the optic nerve)
- Postganglionic short ciliary nerves → sphincter pupillae → miosis
The parasympathetic fibers travel superficially in CN III - this is why early CN III compression (e.g., from a posterior communicating artery aneurysm) causes a dilated, fixed pupil before eye movement is lost.
B. Sympathetic Pathway (Mydriasis - Dilation)
A 3-neuron chain (first, second, third order):
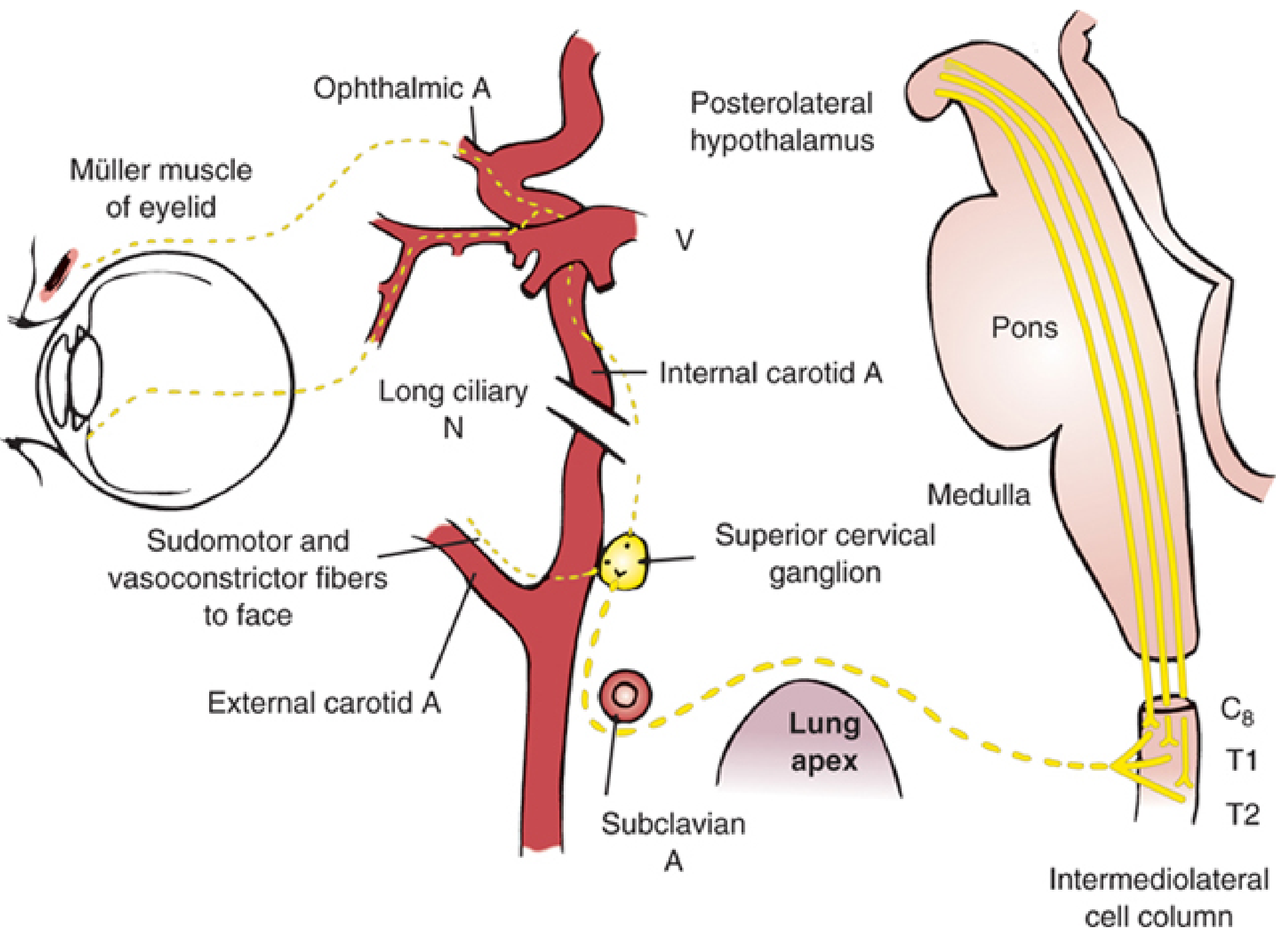
FIGURE: Sympathetic innervation - first-order (hypothalamus), second-order (C8-T2 spinal cord), third-order (superior cervical ganglion to eye) (Localization in Clinical Neurology, 8e)
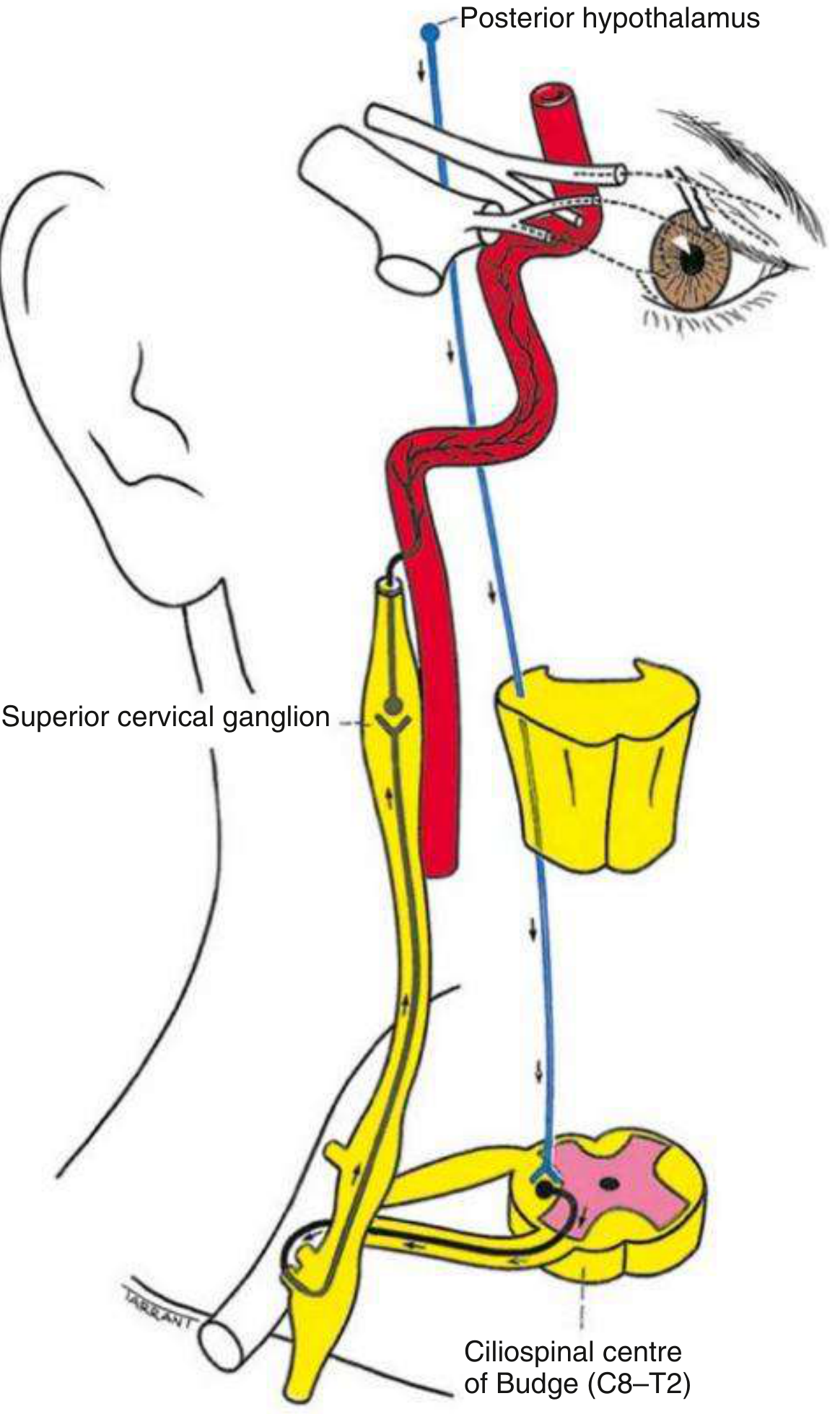
FIGURE: Sympathetic pathway from posterior hypothalamus to eye via ciliospinal centre of Budge (C8-T2) (Kanski's Clinical Ophthalmology, 10th)
| Neuron Order | Origin | Course | Notes |
|---|---|---|---|
| 1st order (Central) | Posterolateral hypothalamus | Descends ipsilaterally through lateral tegmentum of brainstem → ciliospinal center of Budge (C8-T2) | Lesions here = central Horner |
| 2nd order (Preganglionic) | C8-T2 intermediolateral cell column | Exits, passes over lung apex, ascends with carotid to superior cervical ganglion | Vulnerable to Pancoast tumor |
| 3rd order (Postganglionic) | Superior cervical ganglion | Ascends with internal carotid artery → cavernous sinus → ophthalmic branch (V1) → long ciliary nerves → dilator pupillae | Joins CN VI briefly in cavernous sinus |
- Bradley and Daroff's Neurology in Clinical Practice; Localization in Clinical Neurology, 8e
3. THE PUPILLARY LIGHT REFLEX (PLR)
Arc of the PLR
Afferent limb:
- Light → retinal ganglion cells (intrinsically photosensitive) → optic nerve → optic chiasm → optic tract → pretectal nucleus (dorsal midbrain) - fibers leave BEFORE the lateral geniculate nucleus (LGN), explaining why cortical blindness does NOT abolish the PLR.
- Pretectal nucleus sends bilateral signals via posterior commissure → bilateral Edinger-Westphal nuclei
Efferent limb:
- Edinger-Westphal nucleus → CN III → ciliary ganglion → short ciliary nerves → sphincter pupillae → miosis bilaterally
Why both pupils constrict to light in one eye? Because the pretectal nucleus projects to BOTH Edinger-Westphal nuclei via the posterior commissure - this is the basis of the consensual reflex.
The Near (Accommodation) Reflex Triad
When focusing on a near object, three things happen simultaneously:
- Miosis (pupil constriction)
- Accommodation (ciliary muscle contracts, lens rounds up)
- Convergence (medial recti contract)
The near reflex pathway is less well-defined but involves occipitomesencephalic pathways influencing the Edinger-Westphal nucleus from a more ventral route - distinct from the light reflex pathway. This anatomical separation explains light-near dissociation with dorsal midbrain lesions.
4. NORMAL PUPIL PHENOMENA
- Hippus (pupillary unrest): Normal, nonrhythmical small oscillations (<1 mm) after light stimulation - no clinical significance
- Physiological anisocoria: Occurs in up to 20% of the population; difference of 0.4-1 mm; equal in both light and dark; no associated abnormality - this is the most common cause of unequal pupils
- Miosis with age: Pupils become smaller (senile miosis) due to iris muscle weakness
- Bradley and Daroff's Neurology in Clinical Practice
5. PUPILLARY ABNORMALITIES
The Key Clinical Question First:
Is the abnormal pupil the LARGER or SMALLER one?
- Large pupil = defect in parasympathetic constriction (or excess sympathetic)
- Small pupil = defect in sympathetic dilation (or excess parasympathetic)
- Afferent lesions (optic nerve/retina) = pupils are EQUAL in size - only the reflex response is altered (RAPD)
- Kanski's Clinical Ophthalmology, 10th
5A. ABNORMALITIES OF THE LARGE PUPIL (Mydriasis)
i. CN III Palsy (Oculomotor Nerve Palsy)
Mechanism: Compression of parasympathetic fibers on the surface of CN III → loss of sphincter function → unopposed sympathetics → dilated, fixed pupil
Signs:
- Unilateral mydriasis (4-8 mm), non-reactive to light or near
- Ptosis (levator palpebrae superioris paralysis)
- Eye deviated "down and out" (unopposed action of CN IV and CN VI)
IMPORTANT - "Surgical" vs "Medical" CN III palsy:
- Surgical (compressive) - aneurysm (posterior communicating artery), uncal herniation: PUPIL IS INVOLVED FIRST (parasympathetics are superficial)
- Medical (ischemic/microvascular) - diabetes, hypertension: PUPIL IS TYPICALLY SPARED (ischemia affects the core, sparing the peripheral parasympathetics)
A third nerve palsy with pupil involvement is a neurosurgical emergency until a posterior communicating artery aneurysm is ruled out.
Pharmacological test: 1% pilocarpine drops → a denervated pupil (CN III palsy) WILL constrict; a pharmacologically dilated pupil will NOT constrict.
ii. Adie's Tonic Pupil (Holmes-Adie Syndrome)
Mechanism: Damage to postganglionic parasympathetic fibers - denervation of the ciliary ganglion and postganglionic fibers to the sphincter pupillae. Often follows a viral illness. Affects young women predominantly.

FIGURE: Right Adie pupil - large right pupil with absent direct and consensual light reflex (Kanski's Clinical Ophthalmology, 10th)
Signs:
- Large, regular pupil (unilateral in 80%)
- Absent or sluggish direct and consensual light reflex
- Tonic constriction to near (slow and tonic, with slow re-dilation - "tonic pupil")
- Vermiform (worm-like) movements of the pupillary border on slit-lamp
- Light-near dissociation (responds to near but not light)
- Holmes-Adie Syndrome = Adie pupil + absent deep tendon reflexes (especially knee and ankle)
Key feature: With time ("little old Adie"), the pupil becomes SMALL as aberrant regeneration of accommodative fibers to the sphincter increases tonic firing.
Pharmacological test: 0.1-0.125% pilocarpine (dilute) → denervation hypersensitivity → the Adie pupil constricts; the normal pupil does NOT.
Contrast with CN III palsy: Adie pupil responds to near (tonic); CN III palsy shows no near response either.
iii. Pharmacological Mydriasis
- Anticholinergic agents (atropine, scopolamine, ipratropium nebulized accidentally, jimson weed/Datura exposure)
- The pupil is large, fixed, and will NOT constrict with 1% pilocarpine - this differentiates it from CN III palsy or Adie
5B. ABNORMALITIES OF THE SMALL PUPIL (Miosis)
i. Horner Syndrome (Oculosympathetic Palsy)
Mechanism: Interruption anywhere along the 3-neuron sympathetic pathway → loss of dilator tone → miosis + ptosis (Müller muscle paresis)
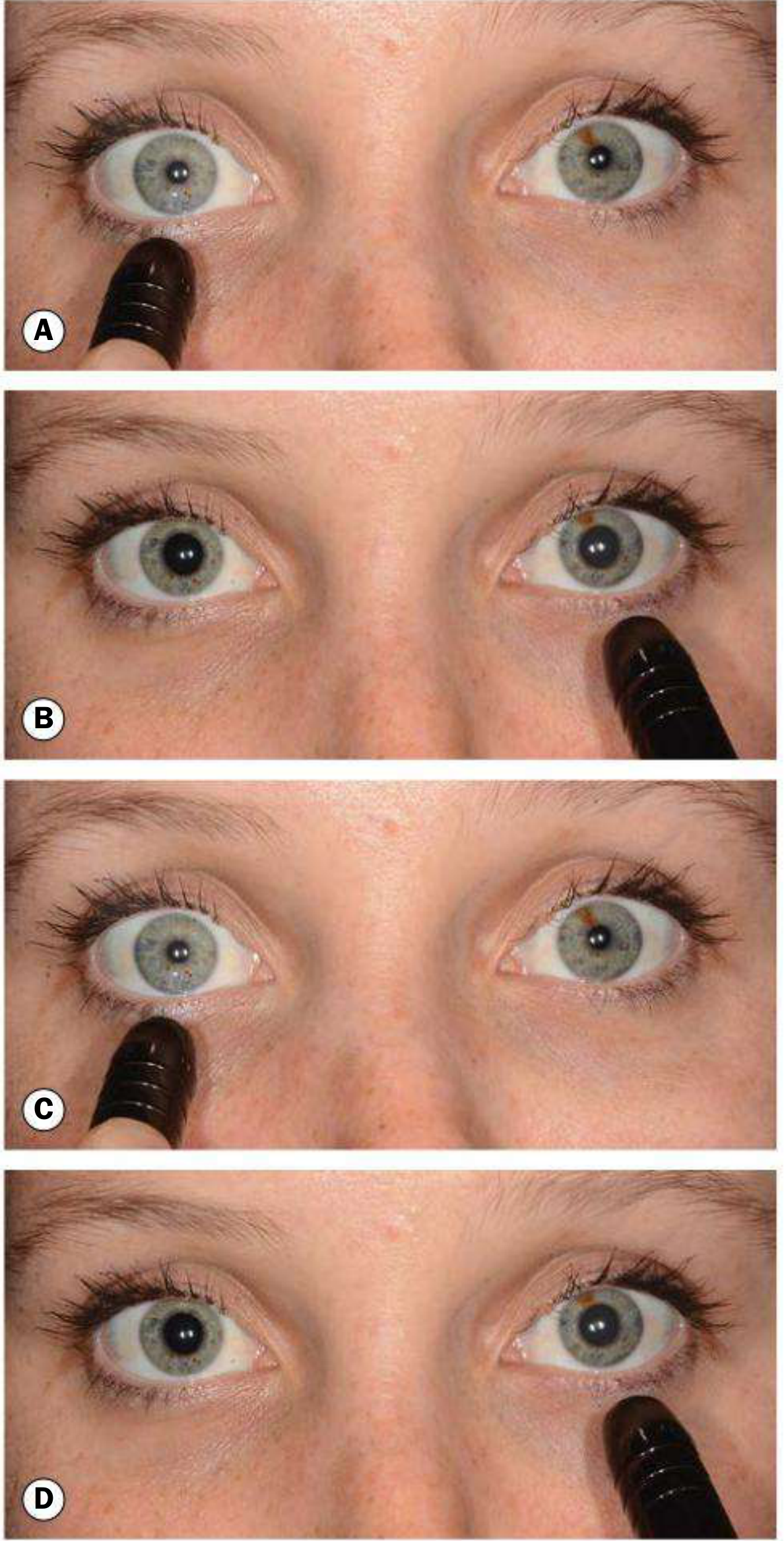
FIGURE: Swinging flashlight test demonstrating left RAPD. (A) Normal right eye stimulated - both pupils constrict. (B) Diseased left eye stimulated - both pupils dilate. (C) Back to right - both constrict. (D) Back to diseased left - both dilate. (Kanski's Clinical Ophthalmology, 10th)
Classic Triad of Horner Syndrome:
- Miosis (small pupil) - anisocoria worse in the DARK (Horner pupil fails to dilate)
- Ptosis (partial/mild, 1-2 mm) - due to Müller muscle paresis
- Anhidrosis - loss of sweating on the ipsilateral face (only with pre-ganglionic lesions)
Additional features: Enophthalmos (apparent), lower lid elevation (reverse ptosis), heterochromia iridis (in congenital cases - lighter iris on affected side due to loss of sympathetic input during development)
Causes by neuron order:
| Order | Causes |
|---|---|
| 1st order (Central) | Brainstem stroke (Wallenberg syndrome - lateral medullary infarct is classic), brain tumors, syringomyelia, multiple sclerosis, hypothalamic lesions |
| 2nd order (Preganglionic) | Pancoast tumor (lung apex), thyroid/neck mass, post-thoracic surgery, cervical rib, aortic aneurysm |
| 3rd order (Postganglionic) | Carotid artery dissection (painful Horner), cavernous sinus lesion, otitis media, cluster headache |
Pharmacological Testing:
| Drug | Normal Pupil | Horner Pupil | Use |
|---|---|---|---|
| 10% Cocaine (blocks norepinephrine reuptake) | Dilates | Fails to dilate | Confirms Horner |
| 0.5-1% Apraclonidine (alpha-2 agonist, weak alpha-1) | No effect | Dilates (reversal of anisocoria) | Confirms Horner (now preferred) |
| 1% Hydroxyamphetamine/Paredrine (releases norepinephrine) | Dilates | Dilates if 1st/2nd order; Fails to dilate if 3rd order | Localizes lesion |
An acute painful Horner syndrome (ipsilateral neck/face pain) = carotid artery dissection until proven otherwise. Urgent CTA/MRA.
ii. Argyll Robertson Pupil
Classic: Bilateral, small (miotic, often <2 mm), irregular pupils with iris atrophy
Key feature: Light-Near Dissociation - pupils do NOT react to light, but DO constrict normally to near stimuli ("accommodates but does not react")
Classic cause: Neurosyphilis (though diabetes is now more common cause of diabetic-type light-near dissociation)
Site of lesion: Rostral midbrain - the pretectal lesion interrupts the light reflex fibers while sparing the near reflex pathway (which is more ventral)
Mnemonic: "Prostitute's Pupils" - accommodates but doesn't react (historically linked to syphilis)
5C. AFFERENT PUPILLARY DEFECT (APD / Marcus Gunn Pupil)
Mechanism: Damage to the afferent limb (retina or optic nerve) reduces light signal reaching the midbrain. Because the efferent pathway and both irises are intact, the pupils REMAIN EQUAL at rest - but the response to light is reduced in the affected eye.
Swinging Flashlight Test:
- Shine light in normal eye → BOTH pupils constrict (normal direct + consensual)
- Swing light to AFFECTED eye → BOTH pupils DILATE (reduced afferent input = less constriction signal)
- This "paradoxical dilation" when light is swung to the affected eye = RAPD (Relative APD)
Causes: Optic neuritis (most common), severe retinal disease, optic nerve lesions (tumor, glaucoma), large retinal detachment
Key teaching point: Pure cortical blindness does NOT produce an RAPD because the pupillary light reflex leaves the optic tract BEFORE the LGN (before reaching the cortex).
5D. PUPILS IN COMA - Brainstem Localization
The pupils tell you WHERE the lesion is in an unconscious patient:
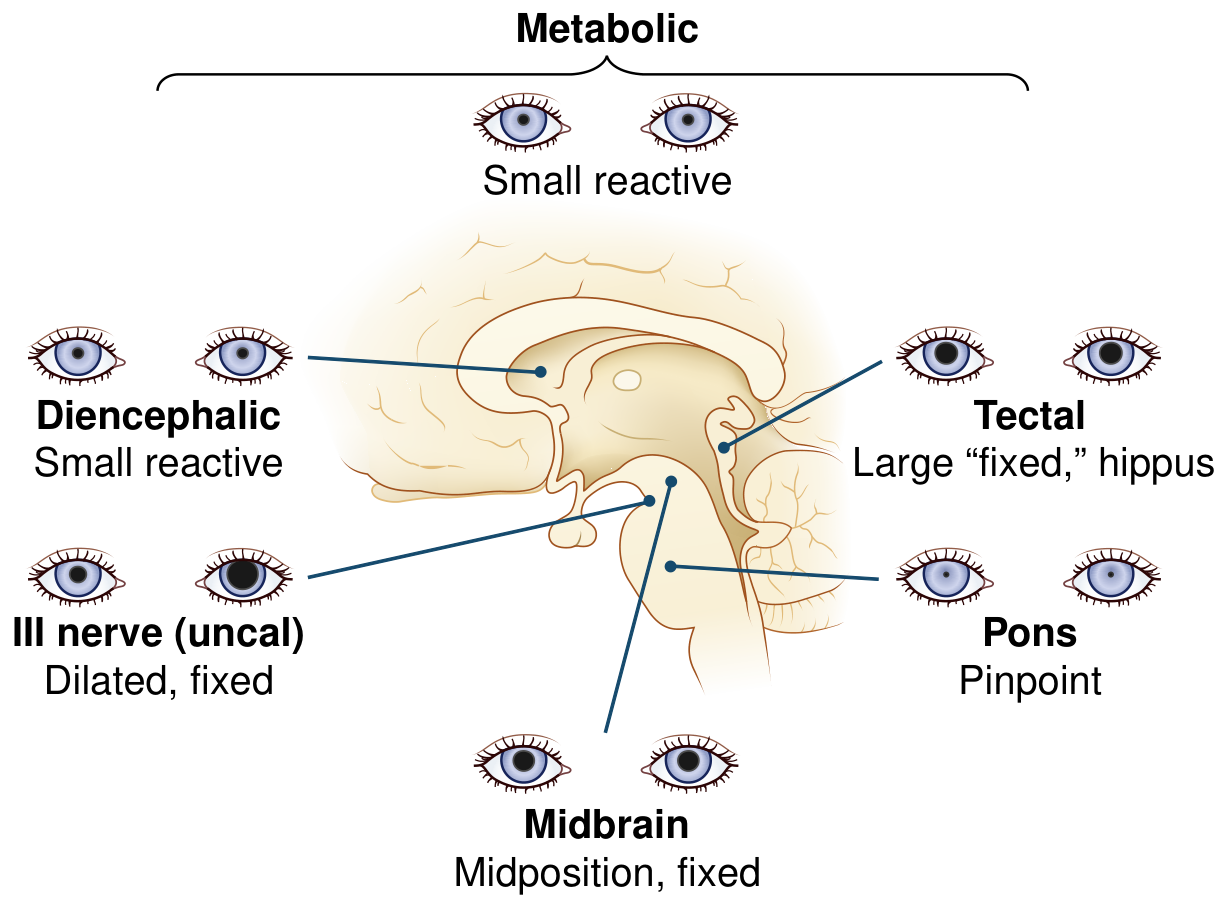
FIGURE: Pupils in Comatose Patients - correlation with lesion level (Bradley and Daroff's Neurology in Clinical Practice)
| Location of Lesion | Pupil Findings |
|---|---|
| Metabolic/Toxic | Small, reactive bilaterally (PLR preserved - most resistant to metabolic insults) |
| Diencephalon/Thalamus | Small, reactive ("diencephalic pupils") |
| Dorsal Midbrain (Tectal) | Mid-position, fixed to light, but may react to near; hippus (spontaneous oscillations) |
| Nuclear Midbrain | Fixed, irregular, mid-position (both sympathetic and parasympathetic disrupted) |
| Pons | Pinpoint pupils (bilateral sympathetic pathway interruption; parasympathetics intact) - but still reactive to magnification |
| Uncal Herniation (CN III compression) | Unilateral dilated, fixed (surgical emergency) |
| Medulla/Cervical Cord | Horner syndrome (unilateral small pupil) |
Metabolic vs Structural coma: Preservation of the PLR strongly suggests metabolic coma. Fixed pupils point to structural brainstem damage.
- Bradley and Daroff's Neurology in Clinical Practice; Plum and Posner's Diagnosis and Treatment of Stupor and Coma
6. SUMMARY TABLE OF MAJOR PUPILLARY ABNORMALITIES
| Condition | Size | Light Reflex | Near Reflex | Other Features | Pharmacological Test |
|---|---|---|---|---|---|
| CN III Palsy | Dilated (mydriasis) | Absent | Absent | Ptosis, eye "down and out" | 1% pilocarpine constricts |
| Adie's Tonic Pupil | Large (initially) | Absent/sluggish | Tonic (slow) - Light-near dissociation | Young women; vermiform movements | Dilute pilocarpine (0.1%) constricts |
| Pharmacological mydriasis | Large | Absent | Absent | History of drug exposure | 1% pilocarpine does NOT constrict |
| Horner Syndrome | Small (miosis) | Normal | Normal | Ptosis, anhidrosis; worse anisocoria in dark | Apraclonidine confirms; hydroxyamphetamine localizes |
| Argyll Robertson | Small, irregular | Absent | Normal | Bilateral; iris atrophy | - |
| RAPD (Marcus Gunn) | Equal at rest | Paradoxical dilation on swinging test | Normal | No anisocoria! | Swinging flashlight test |
| Pinpoint (Pontine) | Bilateral tiny | Reactive (barely) | - | Coma, bilateral | - |
| Uncal herniation | Unilateral dilated | Fixed | - | Rapid deterioration of consciousness | Emergency! |
7. CLINICAL SCENARIOS FOR MBBS
SCENARIO 1 - The Surgical Emergency
Presentation: A 35-year-old woman presents to the ER with the "worst headache of her life" (thunderclap headache). On examination, she has a unilateral dilated right pupil (7 mm) that is non-reactive to light. There is ptosis of the right eye and the eye is deviated downward and outward.
What is the diagnosis?
Posterior communicating artery (PCoA) aneurysm compressing CN III - the parasympathetic fibers travel on the OUTSIDE of CN III, so they are compressed first.
Why is this an emergency?
The aneurysm may rupture causing subarachnoid hemorrhage.
Next step: Urgent CT head (without contrast) to look for SAH, then CT angiography (CTA) or digital subtraction angiography (DSA) to identify the aneurysm.
Teaching point: In CN III palsy, ask: is the pupil involved? If YES - think compressive (surgical) cause. If pupil is spared - think microvascular (diabetes, hypertension) - "medical CN III palsy."
SCENARIO 2 - Horner with Neck Pain
Presentation: A 42-year-old man presents with acute onset right-sided neck and face pain with right-sided ptosis and a small right pupil. The anisocoria is more evident in a dim room.
What is the diagnosis?
Right Horner syndrome (miosis + ptosis). The acute painful onset with neck pain = carotid artery dissection until proven otherwise.
Workup: Urgent MRI/MRA or CTA of the neck to look for carotid dissection.
Confirm Horner first: Apraclonidine 0.5% drops - if Horner, the affected pupil dilates and anisocoria reverses within 30-45 minutes.
Teaching point: Painful Horner = carotid dissection; Painless Horner in a smoker = Pancoast tumor (lung apex) until proven otherwise.
SCENARIO 3 - The Young Woman With Blurred Vision
Presentation: A 28-year-old woman notices her right pupil is larger than the left and she has blurring for near vision. On examination, the right pupil is large (6 mm), has an absent direct and consensual light reflex, but shows slow tonic constriction to a near target. Deep tendon reflexes are absent bilaterally.
Diagnosis: Right Adie's tonic pupil with Holmes-Adie syndrome (absent DTRs).
Confirmatory test: Dilute pilocarpine 0.1-0.125% - the Adie pupil constricts due to denervation hypersensitivity; the normal left pupil does not.
Teaching point: The combination of large pupil + light-near dissociation + absent DTRs in a young woman = Holmes-Adie syndrome. This is benign. Syphilis serology should still be sent if bilateral.
SCENARIO 4 - Bilateral Miotic Irregular Pupils in an Older Patient
Presentation: A 65-year-old male with known longstanding psychiatric illness (treated with antipsychotics for years) is found to have bilateral small, irregular pupils that do not react to light but constrict normally when asked to focus on a near object. Syphilis serology comes back positive.
Diagnosis: Argyll Robertson pupils - classic for neurosyphilis (tabes dorsalis/general paresis of the insane).
Key feature: Light-near dissociation - "accommodates but doesn't react."
Mechanism: Pretectal midbrain lesion (Treponema pallidum) interrupts the light reflex arc (dorsal pretectal fibers) while sparing the more ventral near reflex pathway.
Management: Treat the underlying neurosyphilis (IV penicillin G).
SCENARIO 5 - The Unconscious Patient in ICU
Presentation: An 18-year-old student is brought unconscious after a suspected opiate overdose. He has bilateral pinpoint pupils (barely 1 mm each), reactive under magnification.
Diagnosis: Opioid intoxication - bilateral pinpoint pupils are the hallmark. Opioids act on μ-receptors in the Edinger-Westphal nucleus causing massive parasympathomimesis AND inhibit the locus coeruleus (sympathetic inhibition).
Treatment: Naloxone (opioid antagonist) - pupils will dilate as a positive response.
Compare: If a comatose patient has unilateral dilated fixed pupil - this is uncal herniation compressing CN III = neurosurgical emergency, NOT a drug overdose.
SCENARIO 6 - Swinging Flashlight Surprise
Presentation: A 24-year-old female with a history of one episode of unilateral loss of vision 2 years ago that recovered. Now presents with another episode of right eye blurring. Pupils are EQUAL bilaterally in normal light. On the swinging flashlight test, when you swing the light to the RIGHT eye, both pupils DILATE.
Diagnosis: Right RAPD (Relative Afferent Pupillary Defect) - indicating damage to the right optic nerve. In the context of recurrent episodes: Multiple Sclerosis (optic neuritis).
Key teaching: In RAPD, the pupils are EQUAL at rest - do NOT expect anisocoria. The abnormality is only revealed on the swinging flashlight test.
8. PHARMACOLOGICAL EFFECTS ON THE PUPIL - Quick Reference
| Drug Class | Effect on Pupil | Examples |
|---|---|---|
| Muscarinic agonists (parasympathomimetics) | Miosis | Pilocarpine, physostigmine |
| Muscarinic antagonists (parasympatholytics) | Mydriasis | Atropine, tropicamide, scopolamine |
| Alpha-1 agonists (sympathomimetics) | Mydriasis | Phenylephrine |
| Opioids | Miosis (pinpoint) | Morphine, heroin, fentanyl |
| Cocaine | Mydriasis (blocks norepinephrine reuptake) | - |
| Amphetamines | Mydriasis (releases norepinephrine) | - |
| Alpha-blockers | Miosis | Prazosin, terazosin |
| Organophosphates/nerve agents | Miosis (cholinergic excess) | Sarin, malathion |
9. EXAMINATION TIPS
- Always examine both pupils - compare size in both light and dark
- Swinging flashlight test is the most sensitive bedside test for optic nerve/retinal disease
- Anisocoria worse in bright light = parasympathetic defect (large pupil is the abnormal one)
- Anisocoria worse in dim light = sympathetic defect/Horner (small pupil is the abnormal one)
- Preserve the PLR in metabolic coma - loss of PLR strongly suggests structural brainstem pathology
- Painful Horner = vascular emergency (carotid dissection)
- Pupil involvement in CN III palsy = surgical emergency (compressive aneurysm)
- Near reflex testing is always done in cases where you suspect light-near dissociation
Sources: Costanzo Physiology 7th ed.; Bradley and Daroff's Neurology in Clinical Practice; Localization in Clinical Neurology 8e; Kanski's Clinical Ophthalmology 10th ed.; Adams and Victor's Principles of Neurology 12th ed.; Plum and Posner's Diagnosis and Treatment of Stupor and Coma; Goldman-Cecil Medicine
This is a shared conversation. Sign in to Orris to start your own chat.