Parathyroid gland
Reading File
Finding Sources
Finding Sources
Searching Images
parathyroid gland anatomy histology
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Here is a comprehensive overview of the parathyroid glands drawn from multiple authoritative medical textbooks.
Parathyroid Glands
Anatomy & Location
There are four parathyroid glands located on the posterior surface of the thyroid gland. They are small, oval, reddish-brown structures — each roughly 3–5 mm in diameter and weighing 30–50 mg.
- Superior parathyroids derive embryologically from the 4th pharyngeal pouch and are relatively constant in position, though they may occasionally descend into the tracheoesophageal groove.
- Inferior parathyroids derive from the 3rd pharyngeal pouch (with the thymus) and migrate further, making them more prone to ectopic positions — including the mediastinum, within the thymus, or embedded in the thyroid.
Vascular Supply
Both superior and inferior glands are primarily supplied by the inferior thyroid artery (a branch of the thyrocervical trunk), with anastomoses from laryngeal, pharyngeal, esophageal, and tracheal arteries providing collateral supply. Ligation of the inferior thyroid artery during thyroidectomy does not always compromise parathyroid blood supply for this reason — but transient hypoparathyroidism from ischemia still occurs in up to ~20% of patients after total thyroidectomy.
(Cummings Otolaryngology)
Histology
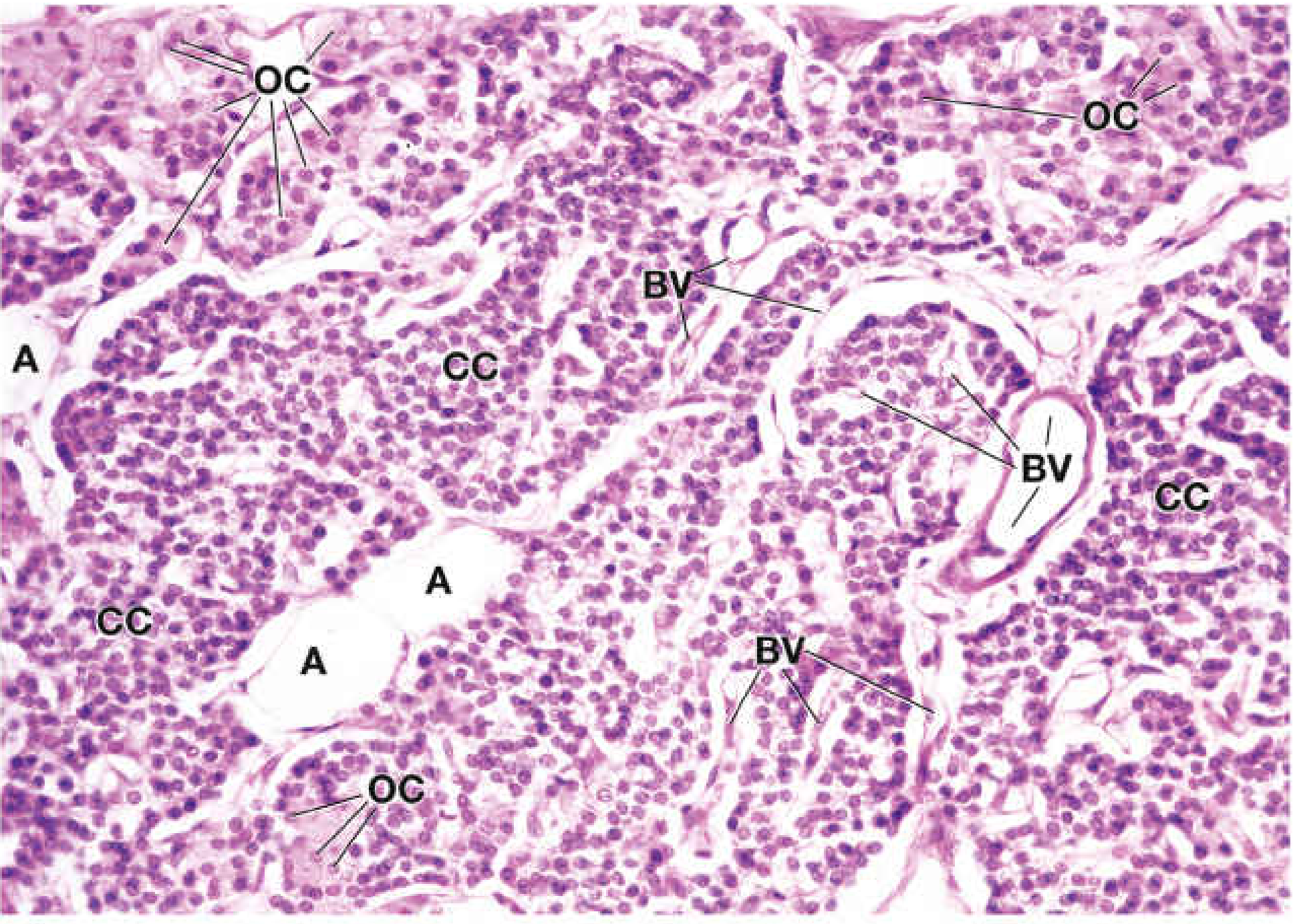
The parenchyma is arranged in cords or sheets separated by capillaries and delicate connective tissue septa. Two main cell types are identifiable on H&E:
| Feature | Chief Cells (CC) | Oxyphil Cells (OC) |
|---|---|---|
| Abundance | More numerous | Less numerous |
| Size | Smaller | Larger |
| Nucleus | Spherical, central | Slightly smaller, more intensely staining |
| Cytoplasm | Scant, lightly staining | Abundant eosinophilic (many mitochondria) |
| Function | Primary PTH synthesis & secretion | Uncertain; accumulate with age |
| Appearance | Uniform sheets | Clusters scattered among chief cells |
Oxyphil cells appear at the end of the first decade and become more numerous around puberty and in older individuals. Stromal adipose cells increase with age and are used as a marker of normal vs. hyperplastic parathyroid tissue.
(Histology: A Text and Atlas)
PTH — Structure and Physiology
PTH is an 84-amino-acid single-chain peptide. The amino-terminal fragment PTH(1–34) is biologically active and highly conserved; synthetic fragments as small as PTH(1–11) can activate the receptor at high concentrations.
Actions of PTH
| Target Organ | Effect |
|---|---|
| Bone | Stimulates osteoclast-mediated Ca²⁺ and phosphate release |
| Kidney (distal tubule) | Enhances Ca²⁺ reabsorption |
| Kidney (proximal tubule) | Increases phosphate excretion; stimulates 1α-hydroxylase → ↑ 1,25(OH)₂D |
| Intestine (indirect) | ↑ 1,25(OH)₂D → ↑ Ca²⁺ absorption |
Net result: ↑ serum Ca²⁺, ↓ serum phosphate.
Regulation of PTH Secretion
PTH release is regulated by a negative feedback loop via the calcium-sensing receptor (CaSR), a G protein-coupled receptor (Gαq) expressed on chief cells:
- ↑ Plasma [Ca²⁺] → CaSR activation → ↑ IP₃ → Ca²⁺ release from ER + PKC activation → inhibits PTH granule secretion (paradoxical inhibition)
- ↑ [Ca²⁺] also inhibits PTH gene synthesis
- 1,25(OH)₂D acts through nuclear receptor → ↓ PTH release and synthesis
- FGF23 (phosphaturic hormone) can also suppress PTH secretion
Small decreases in free plasma [Ca²⁺] produce large, steep increases in PTH release.
(Medical Physiology)
PTH Receptor
PTH binds PTH1R (also responsive to PTHrP), coupled via G proteins to both adenylyl cyclase (↑ cAMP) and phospholipase C. PTH1R is most abundant in the proximal and distal convoluted tubules of the kidney and in bone.
Disorders
Hyperparathyroidism
Primary hyperparathyroidism — usually due to a solitary adenoma (~85%), multigland hyperplasia (~15%), or rarely carcinoma (<1%). Adenomas are monoclonal/oligoclonal neoplasms; genetic drivers include CCND1 (cyclin D1) rearrangement and loss of the MEN1 tumor suppressor. Presents with hypercalcemia, low phosphate, elevated PTH.
Secondary hyperparathyroidism — occurs in chronic kidney disease; reduced 1,25(OH)₂D and phosphate retention drive compensatory PTH elevation.
Hypoparathyroidism
Deficient PTH → hypocalcemia, hyperphosphatemia. Most commonly caused by postsurgical damage to the glands. Also seen in DiGeorge syndrome (22q11.2 deletion — absent parathyroids due to 3rd/4th pouch agenesis).
Pseudohypoparathyroidism (PHP)
Peripheral resistance to PTH despite elevated PTH levels. Caused by inactivating mutations in GNAS1 (Gsα subunit). Type IA = Albright hereditary osteodystrophy (short stature, round face, brachydactyly with sparing of the 2nd digit, soft tissue calcification).
Familial Hypocalciuric Hypercalcemia (FHH)
Autosomal dominant. Inactivating mutations in the CaSR gene → right-shifted Ca²⁺-PTH curve → mild hypercalcemia with normal/mildly elevated PTH and low urine calcium. Subtotal parathyroidectomy has no effect on calcium levels — an important distinguishing feature from primary hyperparathyroidism.
Humoral Hypercalcemia of Malignancy (HHM)
Cancer cells overproduce PTHrP, which acts through the same PTH1R receptor, mimicking hyperparathyroidism biochemically.
Key Clinical Points
- Calcimimetics (e.g., cinacalcet) activate CaSR → suppress PTH — used in secondary hyperparathyroidism and parathyroid carcinoma.
- Calcilytics (negative allosteric CaSR modulators) show promise in autosomal dominant hypocalcemia type 1 (activating CaSR mutations).
- Teriparatide = PTH(1-34) analog — used for osteoporosis and hypoparathyroidism replacement.
- Tc-99m sestamibi preferentially accumulates in oxyphil cells (due to their high mitochondrial content) — basis for parathyroid scintigraphy.
Sources: Harrison's Principles of Internal Medicine 22E • Medical Physiology (Boron & Boulpaep) • Cummings Otolaryngology • Histology: A Text and Atlas • Quick Compendium of Clinical Pathology 5th Ed.
This is a shared conversation. Sign in to Orris to start your own chat.